Purpose
To devise and implement a practice algorithm that would enable rapid detection and appropriate furlough of hospital employees with adenoviral conjunctivitis in order to prevent healthcare-associated epidemic keratoconjunctivitis.
Design
Evaluation of an ongoing quality assurance/improvement initiative.
Methods
Employees of Johns Hopkins Hospital with signs and symptoms of adenoviral conjunctivitis underwent evaluation by nurse practitioners in Occupational Health and rapid diagnostic testing by real-time polymerase chain reaction (PCR). Sequencing was used to determine serotype when adenovirus was detected. Signs, symptoms, diagnosis, and disposition of employees with eye complaints as well as PCR and serotype results were recorded.
Results
Over a 36-month period approximately 18% of initial employee visits were due to unique, eye-related complaints. Viral conjunctivitis was suspected in 542 of 858 employees with eye complaints (62%); adenovirus was detected by PCR in 44 of 542 suspected viral conjunctivitis cases (8%) or 44 of 858 employees with any eye concern (5%). Fourteen of the 44 employees had adenoviral serotypes and clinical presentation consistent with epidemic keratoconjunctivitis (type 37 [n = 6], 8 [n = 4], 4 [n = 3], 19 [n = 1]). Other serotypes found in individuals with less severe conjunctivitis were 3 (n = 5), 4 (n = 5), 56 (n = 4), 1 (n = 2), 42 (n = 1), and 7 (n = 1). No healthcare-associated adenoviral conjunctivitis outbreaks occurred after algorithm implementation, and fewer employees required furlough than had clinical diagnosis alone been used.
Conclusions
The algorithm is an effective infection prevention tool that minimizes productivity loss compared to clinical diagnosis and allows for determination of prevalence and serotype characterization of adenoviral conjunctivitis in hospital employees.
Adenoviral eye infection is a public health concern, with manifestations ranging from self-limited conjunctivitis to prolonged ocular morbidity in the case of epidemic keratoconjunctivitis (EKC). Some adenoviral infections, however, may not be easily distinguishable from EKC at presentation; the 3 other clinical scenarios are nonspecific follicular conjunctivitis, pharyngeal conjunctival fever, and acute hemorrhagic conjunctivitis. EKC is most commonly caused by serotypes 8, 19, and 37 ; less typical serotypes associated with EKC are 4, 53, and 54. EKC is more clinically obvious and induces more morbidity than the other adenoviral eye conditions and is associated with a longer disease course and significant injection, chemosis, and keratitis that can impair vision.
Outbreaks in hospitals and eye clinics result in substantial morbidity and lost productivity. In response to healthcare-associated EKC outbreaks, one of which resulted in the temporary closure of a large eye institute, a “red-eye room,” where persons with potentially infectious conjunctivitis could be triaged and isolated, was established in 1990 in the Wilmer Eye Institute Emergency Room (ER), Department of Ophthalmology, at the Johns Hopkins Hospital (JHH). This arrangement was part of an infection prevention program consisting of ophthalmic instrument decontamination, hand hygiene, use of single-dose eye drops, and employee furloughs. When institutional changes led to the permanent closure of the Wilmer ER and the red-eye room at the end of January 2008, a multidisciplinary team composed of a cornea specialist and stakeholders in infection prevention, employee health, and the clinical virology/molecular infectious disease clinical diagnostic laboratory was convened in order to devise and implement a new practice algorithm for preventing healthcare-associated transmission of adenoviral eye disease. Twenty-month pilot data have been published. Here we report 36-month data on adenovirus detection rates and the results of adding serotype determination to this infection prevention practice algorithm as applied to healthcare workers with red eye.
Methods
The Institutional Review Boards of Johns Hopkins Medicine ruled that publishing of an evaluation of this quality improvement initiative did not require approval as it “does not involve human subjects research under the Department of Health and Human Services or Food and Drug Administration regulations.”
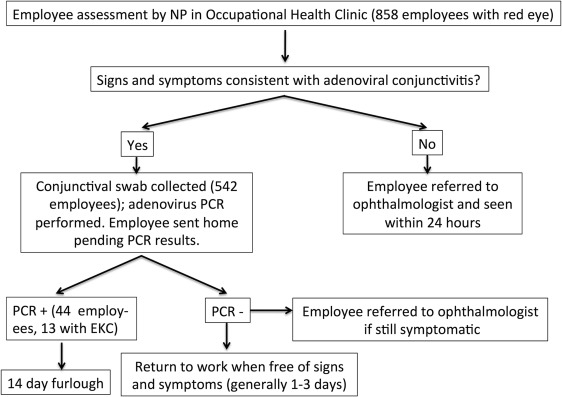
The new red-eye employee practice algorithm, which is in effect at all times, is shown in Figure 1 . It consists of initial evaluation by nurse practitioners in the Occupational Health clinic and rapid diagnostic testing by real-time polymerase chain reaction (PCR) in individuals with signs and symptoms consistent with adenoviral conjunctivitis. The Occupational Health clinic sees employees with health concerns that arise during work hours and may impinge on their ability to work. In order to limit the possibility of transmission within the clinic, employees seeking red-eye evaluation are required to call ahead to make an appointment.
A corneal specialist taught nurse practitioners in the Occupational Health clinic to recognize signs and symptoms of probable viral conjunctivitis (vs conditions like suspected corneal abrasion or subconjunctival hemorrhage) and how to collect swab specimens of the inferior conjunctival fornix. The nurse practitioners were instructed to swab only when viral conjunctivitis was suspected. Swabs (polyester, Dacron, or rayon with plastic or aluminum shafts) were placed in M4 medium and sent at room temperature for PCR testing performed daily at the JHH Clinical Virology/Molecular Infectious Disease Diagnostic Laboratory. Screening criteria included duration of symptoms, presence of viral prodrome, discharge or tearing, and unilateral onset. Employees with suspected viral conjunctivitis were evaluated, swabbed, and discharged home within 30 minutes of intake. Nurse practitioners notified employees of PCR results and furlough status by 8 PM if specimens were received in the laboratory by 3 PM. If adenovirus was detected by PCR, a 2-week furlough was invoked. Direct sequencing of specimens found to contain adenovirus DNA was performed retrospectively for epidemiologic purposes—to determine the proportion of employees infected with EKC-associated adenoviral serotypes (most typically types 8, 19, and 37).
Toward the end of the furlough, the nurse case manager in the Occupational Health clinic contacted employees with adenoviral conjunctivitis by phone to assess symptoms and to schedule a follow-up examination at Occupational Health that was required before return to duty. Furlough was continued if symptoms and signs of conjunctivitis persisted, given probable infectious potential. Employees were sent to the Department of Ophthalmology for consultation for conditions the nurse practitioners deemed an emergency; symptoms including but not limited to persistent redness, tearing, pain, and blurred vision; or conditions in which the nurse practitioners were unsure of diagnosis.
Adenoviral Detection and Serotype Determination
As described in the pilot study, PCR for adenovirus in conjunctival specimens of employees was developed and validated in the Johns Hopkins Hospital molecular microbiology diagnostic laboratory. “Total nucleic acid was isolated from conjunctival specimens (processed volume, 400 microliters) using automated instrumentation (BioRobot M48, using Virus Mini Protocol, version 1.1 software and MagAttract Virus Mini M48 reagents [Qiagen, Germantown, MD];” elution volume, 125 μL). Adenovirus DNA was detected by real-time PCR (primers: 5′-GCC ACG GTG GGG TTT CTA AAC TT-3′, 5′-GCC CCA GTG GTC TTA CAT GCA CAT C-3′; fluorogenic probe FAM 5′-TGC ACC AGA CCC GGG CTC AGG TAC TCC GA-3′ TAMRA) using 7500 Real Time PCR instruments (Life Technologies, Carlsbad, California, USA). The analytical sensitivity (95% detection rate or limit of detection) is 300 copies/mL, and the assay detects at least 16 adenovirus serotypes, including strains from 6 of 7 adenovirus serogroups (A-F). When adenoviruses were detected, serotype was determined by nested PCR of the hexon gene hypervariable regions 1–6 using previously extracted total nucleic acid (outer primers: AdhexF1 (19135-19160) 5′-TIC TTT GAC ATI CGI GGI GTI CTI GA-3′/ AdhexR1 (20009-20030) 5′-CTG TCI ACI GCC TGR TTC CAC A-3′; inner primers: AdhexF2 (19165-19187) 5′-GGY CCY AGY TTY AAR CCC TAY TC-3′/ AdhexR2 (19960-19985) 5′-GGT TCT GTC ICC CAG AGA RTC IAG CA-3′) followed by bidirectional Sanger sequencing using AdhexF2/AdhexR2 as sequencing primers in reactions containing BigDye Terminator v.3.1 (Life Technologies). Sequencing was performed on either a 3100 or a 3500 Genetic Analyzer (Life Technologies). These reagents correctly identified 50 prototype strains; serotypes 15 and 29 have identical sequences in the queried region, cannot be distinguished, and therefore are reported as 15/29. The ability to identify serotypes associated with ocular disease (8, 19, 37) and other serotypes that commonly cause ocular disease (3, 4, 7, 11) was confirmed in house using acquired strains (ATCC, Chantilly, Virginia, USA).
Results
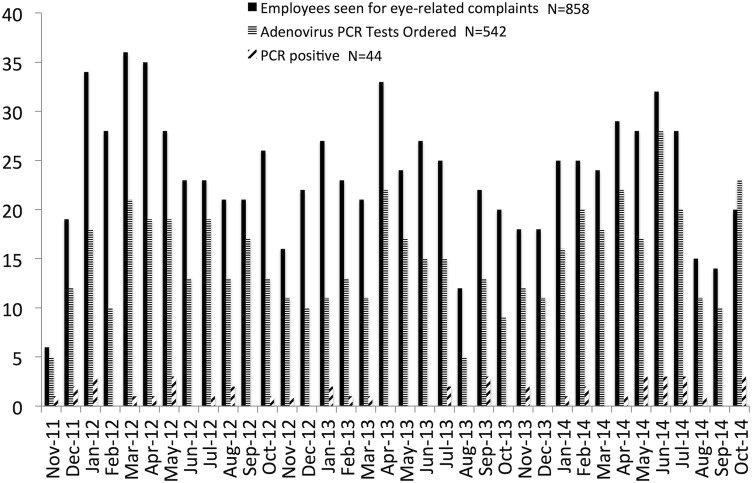
From November 22, 2011 to October 31, 2014, 858 of 4883 initial employee Occupational Health visits (18%) were due to unique, eye-related complaints. The number of employees seen with eye concerns ranged from 6 to 36 per month ( Figure 2 ). Most employees complained of red eye. Of the 858 employees with eye concerns, 542 (62%) underwent conjunctival swabbing and adenovirus PCR testing ( Figure 1 ). Forty-four employees (8% of suspected adenoviral cases, or 5% of all employees with eye concerns) were positive for adenovirus by real-time PCR. Adenovirus serotype could be determined for 32 employees. Overall, 14 employees had serotypes commonly associated with EKC and/or signs and symptoms consistent with EKC. EKC-associated serotypes that were detected included type 37 (n = 6), 8 (n = 4), and 19 (n = 1). Three of 8 employees infected with serotype 4 had signs and symptoms consistent with EKC. The 5 other employees infected with serotype 4 had less severe conjunctivitis. Other serotypes found were 3 (n = 5), 56 (n = 4), 1 (n = 2), 7 (n = 1), and 42 (n = 1). Serotype could not be determined by sequencing for 12 employees. Although adenovirus DNA was detected by real-time PCR from these 12 samples, no PCR products were obtained with the less sensitive nested PCR reaction used for serotype determination. A semiquantitative analysis of cycle thresholds at which adenovirus DNA amplification was detected suggested that samples that could not be serotyped contained approximately 1000-fold less DNA than samples for which serotype was obtained. The median PCR cycle at which adenovirus DNA was detected by real-time PCR was 41 for samples that could not be serotyped, compared to 33 for samples for which a serotype was obtained. None of the 12 patients whose samples could not be serotyped had EKC.
More than half (469/858; 55%) of employees had conditions that were determined to be noninfectious after consultation by a Wilmer or private ophthalmologist; allergic conjunctivitis was most common. The other diagnoses included corneal or conjunctival foreign body, pinguecula, episcleritis, scleritis, corneal abrasion, contact lens overuse, iritis, dacryocystitis, and preseptal cellulitis. The remainder (389/858; 45%) had adenoviral infection confirmed by PCR (44 listed above) or were diagnosed with “viral” or “bacterial” conjunctivitis by an ophthalmologist (either at Wilmer or in the community), a primary care provider, or a doctor at an urgent care center. Conjunctival cultures were not reported for any of these employees, implying that “viral” or “bacterial” was a clinical diagnosis. The majority of employees seen by primary care providers and urgent care doctors were started on topical antibiotic therapy.
To compare the prevalence of laboratory-diagnosed adenoviral conjunctivitis among healthcare employees with eye concerns with the prevalence of this condition among general ophthalmology patients as diagnosed by clinical examination and/or culture, we examined billing data from the Wilmer General Eye Service. Visits with billing diagnoses consistent with adenoviral conjunctivitis (including International Classification of Diseases, 9th revision [ICD-9] codes 372.00, 372.03, 372.71, 379.93, 077.1, 077.3, 077.4, and 077.8) were analyzed. In the 2-year period prior to red-eye room closure (January 2006 through January 2008), there were 9609 patient visits with unique diagnoses (ie, follow-up visits for the same diagnosis for the patient were excluded). An ICD-9 code consistent with adenoviral conjunctivitis was attached to 986 visits; the vast majority of diagnoses were made clinically. Therefore, the prevalence of clinically diagnosed adenoviral conjunctivitis in the General Eye Service was 986 of 9609, or 10%.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


