Purpose
To investigate long-term efficacy and prognostic factors of half-dose photodynamic therapy (PDT) in chronic central serous chorioretinopathy (CSCR).
Design
Retrospective multicenter interventional case series.
Methods
Patients with chronic CSCR undergoing half-dose PDT between 2005 and 2011 were reviewed. Main outcome measures included resolution of serous retinal detachment (SRD) with single PDT, change in best-corrected visual acuities (BCVAs), and recurrence rate of CSCR at 36 months after PDT. Prognostic factors of visual outcome and recurrence of CSCR after PDT were identified with multivariate regression analysis.
Results
A total of 136 eyes of 123 patients were followed up for 57.7 ± 16.2 months. At 36 months after PDT, 132 eyes (97.1%) achieved complete resolution of SRD with single PDT and 4 eyes (2.9%) had CSCR recurrence. The mean logMAR BCVA improved from 0.36 ± 0.29 (Snellen equivalent 20/46; range: 0.1–1.2) at baseline to 0.15 ± 0.23 at 36 months (Snellen equivalent 20/28; range: 0.1–1.5; P < .001) and 0.16 ± 0.24 (Snellen equivalent: 20/29; range: 0.1–1.5; P < .001) at final follow-up. Forty-four eyes (32.4%) had ≥3 lines of BCVA gain while 5 eyes (3.7%) had ≥3 lines of BCVA loss at 36 months after PDT. Nine eyes (6.6%) developed CSCR recurrence at final follow-up. Baseline BCVA was significantly associated with the BCVA ( P = .009) and the improvement in BCVA ( P < .001) at final follow-up. History of bilateral CSCR was significantly associated with CSCR recurrence at final follow-up ( P = .036; odds ratio = 15.84, 95% confidence interval = 1.20–208.32). Eight eyes (5.9%) had complications related to PDT.
Conclusions
Chronic CSCR patients treated with half-dose PDT can achieve long-term stable visual acuity and resolution of SRD. Patients with chronic CSCR are recommended to undergo half-dose PDT before they have significant visual deterioration. Patients with bilateral CSCR are more likely to develop CSCR recurrence after half-dose PDT.
Central serous chorioretinopathy (CSCR) is characterized by 1 or more serous detachments of the neurosensory retina commonly associated with retinal pigment epithelium (RPE) detachments. There is a broad spectrum of clinical presentations. Although the visual prognosis is usually good in acute manifestations, chronic CSCR can be associated with complications such as RPE loss, geographic atrophy, chronic cystic retinal changes, subretinal fibrinous accumulation, subretinal fibrosis, and secondary choroidal neovascularization (CNV). These complications can be associated with permanent visual loss.
The pathogenesis of CSCR is poorly understood but is believed to be related to an abnormal choroidal circulation, as demonstrated by indocyanine green angiography (ICGA). Congested and dilated choroidal vessels, choroidal staining, and hyperfluorescence have been shown in the middle and late phases of ICGA in CSCR patients. In recent years, photodynamic therapy (PDT) has been reported as an effective treatment option for CSCR. PDT works by causing short-term choriocapillaris hypoperfusion and long-term choroidal vascular remodeling, which reduces choroidal congestion, vascular hyperpermeability, and extravascular leakage. However, PDT has the potential of causing RPE tear and subretinal or sub-RPE hemorrhage, a particular concern in eyes with good pretreatment visual acuity. Some studies have reported treating CSCR with modified PDT parameters, including reduced dose (3 mg/m 2 ) of verteporfin or reduced fluence (25 J/cm 2 ) of irradiation, which can minimize side effects. Despite the short-term success of PDT on persistent CSCR, there have been few studies about the long-term efficacy and safety of PDT in treating CSCR. The aim of this study is to evaluate the long-term outcomes and identify predictors of visual outcome and disease recurrence in patients with chronic CSCR treated with half-dose PDT.
Methods
This retrospective multicenter review was approved by the Clinical Ethics Committees of New Territories East Cluster and Kowloon Central Cluster. The research adhered to the tenets of the Declaration of Helsinki. Consecutive patients with chronic CSCR undergoing half-dose PDT at Hong Kong Eye Hospital, Prince of Wales Hospital, and Alice Ho Miu Ling Hospital between January 1, 2005 and December 31, 2011 were studied retrospectively.
Chronic CSCR was defined as idiopathic serous retinal detachments (SRD) in the macular area associated with RPE changes or leakage on fluorescein angiography (FA) with associated visual symptoms for at least 3 months. The inclusion criteria included (1) patient who received half-dose photodynamic therapy; (2) presence of SRD involving the fovea in the optical coherence topography (OCT) images; (3) patient with age of 18 years or older; (4) absence of spontaneous resolution or improvement induced by empirical treatment such as acetazolamide or ketoconazole. Exclusion criteria included (1) previous treatment with PDT or focal thermal laser photocoagulation before the first time point of PDT for CSCR; (2) follow-up period less than 3 years; (3) iatrogenic CSCR caused by systemic corticosteroids; (4) FA or ICGA findings of CNV or polypoidal choroidal vasculopathy (PCV); (5) other maculopathy on clinical examination; (6) media opacity such as cataract that could interfere with adequate acquisition of OCT, FA, and ICGA images.
Patients’ age, sex, first episode or recurrence of CSCR, and duration of the latest onset at their initial visits were recorded. At baseline, all patients had a complete ophthalmologic examination, including measurements of best-corrected visual acuity (BCVA) and intraocular pressure (IOP) by Goldmann tonometry, slit-lamp examination, FA (TRC-50IX; Topcon Corp, Tokyo, Japan), ICGA (TRC-50IX; Topcon Corp), and OCT with 1 of 2 OCT systems including Stratus 3 OCT (Carl Zeiss, Dublin, California, USA) or Spectralis OCT (Spectralis; Heidelberg Engineering Inc, Heidelberg, Germany). Enhanced depth imaging (EDI) was not used for any of the patients in this study. ICGA findings during the middle phase (around 10 minutes after the ICG injection) were classified as intense or intermediate hyperfluorescence or as having no hyperfluorescence according to previous studies.
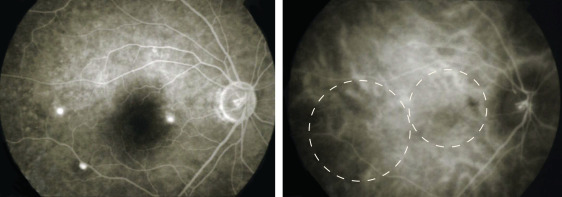
PDT was performed using half-dose verteporfin (Visudyne; Novartis AG, Bülach, Switzerland). In brief, 3 mg/m 2 of verteporfin was infused over 10 minutes, and 5 minutes thereafter the laser treatment was applied. Half-dose PDT was the standard of treatment for patients with chronic CSCR in all involved centers. All chronic CSCR patients would receive half-dose PDT. The area of irradiation was set to cover the area of choroidal dilation and hyperpermeability in ICGA. The total light energy delivered to the area of hyperpermeability was 50 J/cm over 83 seconds. If multifocal, nonconfluent lesions were responsible for the subretinal fluid, consecutive, nonoverlapping laser spots (83 seconds for each spot) were used according to the lesion size in ICGA ( Figure 1 ).
Patients’ records during their follow-up visits at the nearest time points from the first, third, sixth, and twelfth month after PDT and every 6 months thereafter were reviewed. At the follow-up visits, Snellen BCVA, slit-lamp examination, fundus examination, and macular OCT were performed. The same OCT machine was used at pre-PDT and all post-PDT time points for the same patient to measure the central foveal thickness (CFT). The CFT obtained with Stratus 3 OCT was converted to corresponding measurement with Spectralis OCT using the conversion formula previously reported.
Outcomes and Statistical Analysis
The primary outcomes included change in BCVA and proportion of eyes with complete resolution of SRD after single PDT at 36 months after treatment. Secondary outcome measures included change in CFT, number of PDT treatments, any recurrence of CSCR, and the time to a recurrence. A recurrence was defined as the appearance of a new SRD in the OCT images after disappearance following the initial half-dose PDT. Complications of PDT were also recorded.
The Snellen visual acuity was converted to logarithm of the minimum angle of resolution (logMAR) units for statistical analysis. Comparisons of categorical variables between 2 groups were performed using the χ 2 test or the Fisher exact test. Continuous variables were compared using a 2-tailed t test for parametric distribution or Mann-Whitney U test for nonparametric distribution. Association between clinical parameters and the BCVA as well as improvement in BCVA in patients’ final follow-up visits after PDT were analyzed with a multiple linear regression model. A multiple logistic regression model was used to identify the independent predictors of recurrence of CSCR in patients’ final follow-up. Statistical analysis was performed using SPSS version 20.0 (SPSS, Inc, Chicago, Illinois, USA). A P value of <.05 was considered as statistically significant.
Results
One hundred forty-four eyes of 131 patients with chronic CSCR were included in the study. Six eyes of 6 patients were excluded owing to follow-up period less than 3 years. Two eyes of 2 patients with associated CNV or PCV were excluded. One hundred thirty-six eyes of 123 patients were eventually included in the study. The mean age of the patients was 49.4 ± 9.0 years (range: 29–80 years). There were 94 (76.4%) male and 29 (23.6%) female subjects. The mean duration of follow-up was 57.7 ± 16.2 months (range: 36–96 months). The mean duration of symptoms was 8.53 ± 6.96 months (range: 3–52 months). Twenty-three patients (18.7%) had history of bilateral CSCR. Nineteen eyes (14.0%) had history of recurrent CSCR before PDT. The mean baseline logMAR BCVA was 0.36 ± 0.29 (Snellen equivalent 20/46; range: 0.1–1.2).
Presence of subretinal fluid (SRF) was found in all eyes at presentation. Pigment epithelial detachment (PED) was found in 55 eyes (40.4%). The mean baseline CFT was 387.70 ± 105.45 μm. The pattern of leakage on FA was an inkblot pattern in 128 eyes (94.1%) and 8 eyes (5.9%) had a smoke-stack pattern. The ICGA intensity was intermediate hyperfluorescence in 80 eyes (58.8%), intense hyperfluorescence in 49 eyes (36.0%), and no hyperfluorescence in 6 eyes (4.4%). The ICGA of 1 eye was missing in the clinical records.
The mean spot size of the first PDT was 3773.5 ± 1084.5 μm (range: 1500–6400 μm). At 36 months after the PDT treatment, 132 eyes (97.1%) achieved complete SRD resolution with a single PDT treatment. Three eyes (2.2%) of 3 patients received second half-dose PDT for persistent SRD and all these eyes achieved complete SRD resolution after repeat treatment. The remaining eye had spontaneous resolution of SRD after 36 months and did not receive further PDT until the final follow-up. The logMAR BCVA significantly improved from 0.36 ± 0.29 (Snellen equivalent 20/46; range: 0.1–1.2) to 0.15 ± 0.23 at 36 months after PDT (Snellen equivalent 20/28; range: 0.1–1.5; P < .001). Forty-four eyes (32.4%) had ≥3 lines of BCVA gain while 5 eyes (3.7%) had ≥3 lines of BCVA loss at 36 months after PDT. The BCVA at 3, 6, 12, 24, and 36 months and at patients’ last follow-up were all significantly ( P < .001) better than that at baseline ( Table 1 ). The CFT improved from 387.70 ± 105.45 μm at baseline to 244.23 ± 53.74 μm at 36 months post PDT. The CFT at 3, 6, 12, 24, and 36 months and at patients’ final follow-up after PDT treatment were all significantly ( P < .001) better than at baseline ( Table 1 ). Multiple linear regression model showed that baseline BCVA was positively associated with BCVA at patients’ final follow up ( P = .009, standardized β = 0.662; Table 2 ). Baseline BCVA was also negatively associated with improvement in BCVA at patients’ final follow-up ( P < .001, standardized β = −0.609; Table 3 ). Age, sex, duration of symptom, PDT spot size, baseline CFT, history of recurrent CSCR, history of bilateral CSCR, FA pattern, grade of ICGA intensity, coexistent PED, resolution of SRD after first PDT, and CSCR recurrence were not significantly associated with BCVA and change in BCVA at patients’ last follow-up. Duration of symptoms was significantly correlated with baseline BCVA (r = 0.309, P < .001, Pearson correlation). Eyes with baseline Snellen BCVA of 20/40 or better (28 of 83 eyes) were significantly more likely than eyes with worse than 20/40 baseline vision (5 of 53 eyes) to achieve BCVA of 20/20 or better at the final follow-up after PDT ( P = .001; odds ratio [OR] = 4.89, 95% confidence interval [CI] = 1.75–13.65, Fisher exact test).
| Characters | Results | P Value |
|---|---|---|
| Pretreatment BCVA (logMAR) | 0.36 ± 0.29 | |
| Posttreatment BCVA (logMAR) | ||
| 3 months | 0.24 ± 0.32 | <.001 a |
| 6 months | 0.20 ± 0.30 | <.001 a |
| 12 months | 0.17 ± 0.26 | <.001 a |
| 24 months | 0.19 ± 0.26 | <.001 a |
| 36 months | 0.15 ± 0.23 | <.001 a |
| Final follow-up | 0.16 ± 0.24 | <.001 a |
| Subgroup of BCVA | ||
| Pretreatment | ||
| ≥20/30 | 42 (30.9%) | |
| 20/40–20/80 | 70 (51.5%) | |
| ≤20/100 | 24 (17.6%) | |
| 36 months | ||
| ≥20/30 | 116 (85.3%) | |
| 20/40–20/80 | 18 (13.2%) | |
| ≤20/100 | 2 (1.5%) | |
| Final follow-up | ||
| ≥20/30 | 114 (83.8%) | |
| 20/40–20/80 | 15 (11.0%) | |
| ≤20/100 | 7 (5.1%) | |
| Pretreatment central foveal thickness (μm) | 387.70 ± 105.45 | |
| Posttreatment central foveal thickness (μm) | ||
| 3 months | 239.61 ± 52.50 | <.001 a |
| 6 months | 238.28 ± 41.82 | <.001 a |
| 12 months | 237.43 ± 44.83 | <.001 a |
| 24 months | 236.45 ± 39.96 | <.001 a |
| 36 months | 244.23 ± 53.74 | <.001 a |
| Final follow-up | 237.78 ± 44.10 | <.001 a |
| Complete SRD resolution with single PDT at 36 months | ||
| Yes | 132 (97.1%) | |
| No | 4 (2.9%) | |
| Number of PDT required at final follow-up | ||
| 1 | 128 (94.1%) | |
| 2 | 8 (5.9%) | |
| Recurrence of CSCR at final follow-up | ||
| Yes | 9 (6.6%) | |
| No | 127 (93.4%) | |
| Time of recurrence | 43.6 ± 33.7 (10–93 months) | |
| Ocular complications | ||
| RPE atrophy | 5 (3.7%) | |
| CNV | 1 (0.7%) | |
| RPE rip | 1 (0.7%) | |
| Macular scar | 1 (0.7%) |
| Predictors | β | Standard Error | Standardized β | 95% CI for β | P Value |
|---|---|---|---|---|---|
| Age (y) | −0.002 | 0.002 | −0.073 | −0.006 to 0.002 | .321 |
| Male | −0.074 | 0.042 | −0.127 | −0.157 to 0.009 | .081 |
| Duration of symptom (mo) | 0.001 | 0.003 | 0.033 | −0.005 to 0.008 | .663 |
| Pretreatment BCVA (logMAR) | 0.560 | 0.067 | 0.662 | 0.427 to 0.694 | .009* |
| History of recurrent CSCR before PDT | 0.067 | 0.051 | 0.093 | −0.035 to 0.169 | .197 |
| History of bilateral CSCR | −0.019 | 0.46 | −0.033 | −0.110 to 0.72 | .685 |
| PDT spot size (μm) | <0.001 | <0.001 | 0.005 | – | .944 |
| Baseline CFT (μm) | <0.001 | <0.001 | −0.152 | −0.001 to <0.001 | .057 |
| Inkblot pattern in FA | −0.009 | 0.068 | −0.010 | −0.144 to 0.125 | .892 |
| Grade of ICGA intensity | 0.003 | 0.033 | 0.007 | −0.062 to 0.069 | .921 |
| Coexistent PED | 0.007 | 0.037 | 0.013 | −0.067 to 0.080 | .860 |
| Resolution of SRD with single PDT | 0.079 | 0.136 | 0.043 | −0.191 to 0.350 | .561 |
| Post-PDT CSCR recurrence | −0.022 | 0.075 | −0.022 | −0.170 to 0.126 | .767 |
| Predictors | β | Standard Error | Standardized β | 95% CI for β | P Value |
|---|---|---|---|---|---|
| Age (y) | −0.002 | 0.002 | −0.086 | −0.006 to 0.002 | .321 |
| Male | −0.074 | 0.042 | −0.150 | −0.157 to 0.009 | .081 |
| Duration of symptom (mo) | 0.001 | 0.003 | 0.039 | −0.005 to 0.008 | .663 |
| Pretreatment BCVA (logMAR) | −0.440 | 0.067 | −0.609 | −0.573 to −0.306 | <.001* |
| History of recurrent CSCR before PDT | 0.067 | 0.051 | 0.110 | −0.035 to 0.169 | .197 |
| History of bilateral CSCR | −0.019 | 0.46 | −0.039 | −0.110 to 0.72 | .685 |
| PDT spot size (μm) | <0.001 | <0.001 | 0.006 | – | .944 |
| Baseline CFT (μm) | <0.001 | <0.001 | −0.178 | −0.001 to <0.001 | .057 |
| Inkblot pattern in FA | −0.009 | 0.068 | −0.011 | −0.144 to 0.125 | .892 |
| Grade of ICGA intensity | 0.003 | 0.033 | 0.009 | −0.062 to 0.069 | .921 |
| Coexistent PED | 0.007 | 0.037 | 0.015 | −0.067 to 0.080 | .860 |
| Resolution of SRD with single PDT | 0.079 | 0.136 | 0.051 | −0.191 to 0.350 | .561 |
| Post-PDT CSCR recurrence | −0.022 | 0.075 | −0.026 | −0.170 to 0.126 | .767 |
Clinical Characteristics of Eyes With and Without Recurrence of Chronic Central Serous Chorioretinopathy Post Photodynamic Therapy
Nine eyes (6.6%) of 8 patients developed recurrence of CSCR at their final follow-up ( Figure 2 ). Four eyes (2.9%) of 3 patients had recurrence within 36 months after PDT. Five cases received a second PDT treatment while the remaining 4 cases of recurrent CSCR resolved spontaneously. The mean time to recurrence of CSCR was 43.6 ± 33.7 months (range 10–93 months). The clinical characteristics of eyes with and without recurrence of CSCR at their final follow-up after PDT treatment were shown in Table 4 . Four patients with failed resolution of SRD with single PDT were excluded from the analysis. For patients who had both eyes treated with PDT, only the right eye was included in the analysis. There were no significant differences in the age, sex distribution, duration of symptoms, PDT spot size, baseline BCVA, proportion of coexistent PED, FA pattern, grade of ICGA intensities, history of recurrent CSCR, and resolution of CSCR with single PDT between 2 groups. However, eyes with recurrent CSCR post PDT had a significantly higher proportion of history of bilateral CSCR ( P = .004, Fisher exact test). A multiple logistic regression model ( Table 5 ) with the above parameters showed that history of bilateral CSCR was significantly associated with recurrence of CSCR after PDT ( P = .036; odds ratio = 15.84, 95% CI = 1.20–208.32).



