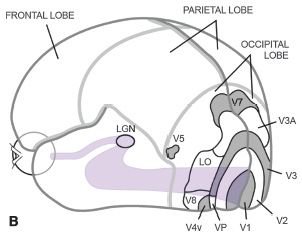
FIGURE 9.1 A:Visual pathways. The retinocortical pathway transfers information through the lateral geniculate body (LGN) to the primary visual cortex and through the tectal pathway via the superior colliculus (SC) to pulvinar (PU) and the parietal, occipital, and frontal lobe. The two parallel visual pathways make it possible that certain areas of the brain can get normal visual information via the tectal pathway when the main pathway is damaged posteriorly. The two main directions of the flow of the visual information from the occipital cortex are called the dorsal stream (DS) toward the posterior parietal lobe where visual functions are related to orientation in space and eye–hand coordination and the ventral stream (VS) toward the inferior temporal lobe where visual functions include recognition-related tasks. B: The primary visual cortex (V1) and other visual cortices. C: The cortical visual networks, the ventral and the dorsal stream, and the mirror neuron system (MNS) are depicted by arrows on the surface of the brain. (A mirror neuron is one that fires both when an animal or person acts and when the animal observes the same action performed by another.) (Reprinted from Hyvärinen L, Jacob N. What and how does this child see?: Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013, with permission.)
In the assessment of the visual system, several considerations are made: (i) eyes are the receivers of visual information; (ii) the long visual pathways are a part of active processing; and (iii) the brain ultimately processes visual information. Visual processing begins in the occipital lobe as early processing and continues in numerous functions of the ventral and dorsal streams and the mirror neuron system.
FACTORS THAT MAY INFLUENCE ASSESSMENT OF VISION
When assessing vision in visually impaired children, especially visually impaired children with other disabilities, numerous factors can affect children’s responses: A child may be seriously ill, weak, or sleepy because of medications. It is wise to inquire when medications are given and choose a time when they least affect alertness. A best time for assessment is often during and after the midday meal or later in the afternoon.
Communication needs to be at the level of the child. Observation on how the parents interact with the infant/child helps the vision specialist to choose the most effective type of communication for a particular child.
The child’s visual sphere is observed, so that testing can be performed well within it. The size of the visual sphere is influenced by the visual qualities of objects, their movement, and emotional value in the space in which the child uses vision. For communication, the parent’s or the tester’s face is one of the best objects to test the range of a child’s visual sphere.
Visual attention often varies. Sometimes shifting attention is so difficult that the child uses a head movement because the normal saccadic movement cannot be initiated or performed.
Ocular motor functions are observed for some time while the parents interact with the child and are assessed using regular clinical tests: fixation to penlight and to details of a small picture, tracking, saccades, convergence, miosis during convergence, accommodation, and nystagmus. Ocular motor functions, especially convergence, miosis, and accommodation, should be also assessed by the early intervention team together with the kindergarten teacher and therapists as observers. Refraction and accommodation need to be especially carefully measured before the assessment in infants with Down syndrome and all infants with brain damage and hypotonia. The signs are described to therapists, teachers, and parents and preferably recorded on video. If a child uses a compensatory head turn or tilt to avoid diplopia or nystagmus, this should be clearly explained to each new person involved in the care of the child to avoid the inappropriate redirection of a child’s head to a “correct” position, which would make it nearly impossible for the child to have useful sight.
Accommodation should not be forgotten in the assessment of healthy-looking infants, especially if the infant has difficulties in early visual communication. The three frames from a video in Figure 9.2 show the effect of near correction on insufficient accommodation: The 4-month-old healthy infant who refused visual communication sees the face of the mother clearly for the first time through the +4 lenses, has eye contact, looks surprised for a few seconds, and then smiles her first social smile.

FIGURE 9.2 Effect of compensation for weak accommodation with near correction. (Reprinted from Hyvärinen L, Jacob N. What and how does this child see?: Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013, with permission.)
Clinical assessment of visual sensory functions includes measurement of distance vision acuity, near vision acuity, visual acuity at low contrast levels, grating acuity, reading acuity, visual field, color vision, visual adaptation, and motion perception.
VISUAL ACUITY AS RECOGNITION ACUITY
Visual acuity as recognition acuity is used most often in the assessment of vision. The definitions of proper visual acuity tests are poorly known, and therefore, there are numerous tests that do not comply with the international recommendations. In 1980, the Committee on Vision (2) set guidelines for the structure of visual acuity charts: (i) optotypes on each test line were to be equally discriminable; (ii) since this was not possible even with the most commonly used letter optotypes, the 10 Sloan letters, the optotypes on each test line were and are arranged to result in an equal average difficulty per line, which resulted in the Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity charts (3).
In 1984, the Visual Function Committee of the Consilium Ophthalmologicum Universale wrote its Visual Acuity Measurement Standard. This stated that the basic visual acuity test is the line test that has at least five optotypes (test symbols) on the test lines with spaces between the optotypes that are equal to the width of the optotypes of that line and where the distance between the test lines is equal to the height of the lower line (4). In 2003, the World Health Organization published its recommendation for measurement of visual acuity in surveys (5) and added the following to the recommendations: the luminance level should be between 80 and 160 (candela/square meter) and pointing should not be used in the basic measurement. In a child with impaired vision, pointing at the optotype to be read may improve visual acuity value threefold (6). Measurement with pointing as a second test is often worthwhile after the threshold value without pointing is recorded because it may reveal fixation difficulties and the importance of visual reference for fixation during reading.
In pediatric services, visual acuity charts can be used to examine older children. For infants, young children, and children with very limited communication, other tests are needed. Visual acuity measurements thus cover a broad area, including (i) detection acuity measured with small objects; (ii) grating acuity as detection acuity by preferential looking; (iii) grating acuity by resolving orientation of lines; (iv) recognition acuity using optotype tests: single optotype tests, line tests, and crowded tests; and (v) reading acuity.
Detection Acuity, Measured with Small Objects
Dark-colored cake decorations <2 mm in diameter on light-colored surfaces are better test objects than light-colored sweets on dark surfaces. If the child has uncorrected hyperopia and insufficient accommodation, light-colored small pieces on a dark surface are seen as blurred images like haloes. Thus, the large size of the object with halo does not give an accurate impression of detection acuity.
To perform the test, both hands are moved over the top of the light-colored surface in front of the child and a few pieces of sweets are dropped onto the surface without stopping the movement. Several observations are made: (i) how the child scans the surface to find the sweets and (ii) whether errors in localizing the small objects might be caused by defects in the central visual field or problems in eye–hand coordination.
Grating Acuity as Detection Acuity
If visual acuity cannot be measured with optotype tests because of communication difficulties, a rough estimate of the function of the visual pathways may be possible using grating acuity measurements. When a striped pattern is presented in front of an infant simultaneously with a gray surface of the same size and luminance, the infant is likely to preferentially look at the striped pattern. The original Teller Grating Acuity Cards (no longer available) and LEA Gratings are used in the United States. Children can detect the grating lines even if they see them badly distorted, so grating acuity values should not be converted into optotype acuity values.
Grating Acuity by Resolving Line Orientation
True grating acuity is measured if the subject is able to resolve the orientation of lines on gratings printed on round tests that can be presented in different orientations. Again, in this test situation the orientation of grating can be seen even if the lines are badly distorted. The size of the stimulus affects the grating acuity value when there are scotomas, diffuse or circumscribed loss of functioning cone cells, in the area that is investigated. This was documented in one of the early investigations on grating stimuli in measuring contrast sensitivity (CS) (7). Therefore, large, 10- to 20-degree grating stimuli are needed in basic measurements. It is possible to learn about the function of the central visual field by using a small area of the grating to determine whether grating acuity becomes lower (for details, see the Ref. (7)).
Recognition Acuity, Optotype Tests
When testing adults, it is customary to test distance vision first, followed by near vision. When testing children, better results are obtained by starting with near vision tests before proceeding to distance vision tests at 3 meters. Binocular vision is tested first and then each eye separately.
There are numerous pediatric visual acuity tests with a variety of pictures that measure picture perception and recognition but not recognition of abstract forms like letters and numbers. Most sets of picture optotypes have not been calibrated with the Landolt C, the reference optotype, and have optotypes with variation in total size, form, and amount of black color, and/or their layout does not follow the international recommendations. Visual acuity values measured with such picture tests are, therefore, not comparable to those measured with calibrated tests and Landolt C test and do not measure recognition of letters. Among the picture tests, the LEA Symbols test is the only test with optotypes calibrated with the Landolt C. The symbols are so abstract in their forms that they are close to letters and numbers in recognizability if the abstract words “circle,” “square,” “pentagon,” and “fruit” are used during testing. Yet, if we use the names of pictures of concrete objects, such as “ring,” “window,” “house,” “apple,” or any other name of concrete objects, the symbols can be recognized at an earlier age than the fully abstract letters and numbers and still earlier if matching is used in answering. In vision screening, preschool and school-aged children can thus be tested using LEA Symbols charts and single symbol tests until calibrated letter (ETDRS) or number (LEA Numbers) charts can be used.
If a child has problems in reading, the first thing to learn is how he or she sees letters, whether he or she recognizes all letters, what kind of words are the most difficult, and whether they have something in common in structure. If the child cannot see letters, then the problem is not a reading problem but a problem in the basic visual function of perception and recognition of letters. Inability to recognize letters in school age is rare among children with normal cognitive functions. In 30 years of the use of the LEA Symbols, only two children, who had very specific difficulties in perceiving letters, also had difficulties perceiving and naming LEA Symbols. The first one was a bright teenage girl who had basic problems in perceiving length of lines visually but was able to correctly grasp the LEA Rectangles, that is, the awareness of length was available to parietal visual functions (eye–hand coordination) but not to the inferotemporal functions (recognition). She could not perceive geometric forms visually but had learned by herself to move her finger above the forms and use the information from movement to create the image. She used this technique first to recognize letters and ultimately learned to read. She could not recognize geometric forms visually. The distance between two nonmoving LEA Rectangles had to be 13.5 cm for her to perceive them as two separate black objects. However, if the black rectangles were moved, she could perceive them as two distinct objects when the distance was 0.5 cm. It was understandable why she had difficulty in visually recognizing LEA Symbols (8) that are close to geometric abstract forms. She had no difficulty in perceiving numbers in the LEA Numbers test, with which her visual acuity was 1.6 (20/12.5).
The second child with specific loss of letter and number recognition was a 7-year-old girl who had been examined earlier and found to have visual acuity of 6/9 (20/25) as measured with Kay pictures. She had learned to recognize and write four of the five letters in her name, one as a mirror image when writing her name from right to left. She recognized no numbers. When she should have written number 3, she wrote 3 small circles. She had difficulties in recognizing the LEA Symbols in a line test, and visual acuity measured with single symbols was low (6/38, 20/125). Since the child saw the LEA Symbols for the first time and used more abstract names “circle,” “square,” “pentagon,” and the more concrete “apple,” this suggested that the measurement needed to be repeated to collect more information on early perception functions. If a child does not recognize letters and abstract forms and has no difficulty recognizing pictures of concrete objects, Kay pictures, which are noncalibrated pictures of concrete objects unrelated to letters, may lead to an overestimation of visual acuity.
Measurement of visual acuity is complex. There are different age groups that can have different abilities to understand concepts used in testing and many different communication techniques. Several visual recognition and detection tests are needed when choosing the correct test for each child. The test chosen should assess best the visual function of interest but take into account how difficult the test might be for a particular child. Tests must also conform with the international recommendations (2–4). (For more details, please visit www.lea-test.fi Vision Tests.)
Of the pediatric tests based on letters, the acuities of the HOTV test differ significantly from the reference optotype Landolt C test (P < 0.029) and have significant differences in discriminability of optotypes within the test (9).
Before testing starts, a method of communication must be established, such as naming (signing) or matching. If the child does not spontaneously name the test symbols, you may ask “What should we call this?” and suggest two common names to choose from. If a child does not talk, he or she can use a key card to match, which slows testing and requires changes in accommodation when testing at a distance, except when the LEA Puzzle board is used as the tactile keycard.
Children with very limited communication are tested with single optotype tests and the presentation is varied to meet the communication needs of each child.
Training is often needed when testing young children and children with developmental delay. The child needs to develop the concept of same, which is learned first when comparing colors and next with forms. Playing with colorful test optotypes on the LEA Puzzle can be first used in training (Fig. 9.3) and then the black-andwhite side of the Puzzle. The next concept to be learned is the concept of pictures representing objects comparing the puzzle pieces and flat pictures on the key card. When this concept has developed, smaller and smaller pictures can be used, that is, the play situation becomes a measurement of visual acuity with single optotypes. Infants as young as 13 months and regularly at 18 months are able to play with puzzles if given the opportunity; thus, measurement of visual acuity may be possible even before the age of 2 years.

FIGURE 9.3 A young child with Down syndrome training for testing with LEA Symbols. (Reprinted from Hyvärinen L, Jacob N. What and how does this child see?: Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013, with permission.)
A line of optotypes is considered to have been seen when more than 50% (e.g., 3 of 5, 4 of 6) of the optotypes presented have been read correctly. The visual acuity value is printed next to the test line. If pointing is used in a second measurement, it is recorded in the report.
The test distance should be kept as the standard distance of the test or, if needed, at 1/2, 1/3, or 1/4 of the standard distance. Testing always should be performed well within the visual sphere of the child. During near testing, the cord fixed on the near test helps to maintain the standard distance.
Near vision is functionally more relevant than distance vision in a young child. When examining normally sighted children, the card should be held at the standard distance of the test card. For visually impaired children, it is useful to allow the child to use the preferred distance and angle and use the refractive correction for that distance during the first test. Vision at the standard distance can be measured later. Visual acuity value is not equivalent to the print size used in learning because nobody likes to read at the level of his/her threshold.
Distance testing follows exactly the same procedure as near vision testing. The line above the line to be read can be covered to help the child in keeping fixation on the correct line.
Even with standardized testing and testers trained to perform precisely to the standard, there are still surprising variations in some children’s visual acuity values. We cannot standardize the most important variable in the test situation: the child! The mood and the concentration of the child can vary so much that the results can be two lines better or worse. Thus, a drop in a visual acuity value might be within normal variation, and the test should be repeated the same day or within a few days before considering referral for further evaluation.
In the measurement of optotype acuity/recognition acuity, we should:
• Use age-appropriate tests with correct layout and optotypes or large enough grating stimuli and correct luminance levels and follow the instructions of each test
• Adjust communication to the level that is comfortable for the child
• Test first at near, then at distance
• Test with single, line, and crowded tests when needed and report the name of the test
These basic facts in psychophysics can be condensed into one sentence: always think what you want to measure and choose the test that is designed to measure that function in question.
Even though much time is spent measuring visual acuity at high contrast, it depicts visual information that is rarely of use to a young child (i.e., small details at high contrast) until she/he becomes interested in letters and numbers. Therefore, visual acuity should also be measured at low contrast levels (as discussed in Contrast Sensitivity).
Reading Acuity
When a child knows letters, reading acuity should be measured using the size and spacing of the text that gives optimal reading speed. This is usually a task for special educators, who produce appropriate grade-level texts, and for the low vision team.
If a child can read but makes atypical reading errors, the cause might be a small scotoma on the right side of the fixation point (when reading from left to right). The scotoma can cause one or two letters to disappear. When the eye and, therefore, the scotoma move to another location, the child sees the missed letters and corrects the error. By magnifying or enlarging the text, the scotoma covers smaller parts of the word until, at a certain text size, it no longer interferes with reading. If errors disappear by increasing the size of the text, the child is likely to have a visual field problem, not dyslexia.
Refraction should be corrected so that the best possible image is available to the child for near vision and intermediate distances within the child’s visual sphere and for distance vision if it is used. A child may use a different preferred retinal locus at near than at distance or uses one eye at distance and the other at near. These possibilities should also be considered.
CS measures the ability to see details at low contrast levels. Visual perception at low contrast levels is particularly important (i) in communication, because faint shadows in motion on our faces carry visual information related to facial expressions; (ii) in orientation and mobility, because curbs, stairs, and shadows can be of low contrast; (iii) in everyday tasks at low contrast like cutting an onion on a light-colored surface, pouring coffee into a dark mug, or checking for wrinkles on an ironed shirt; and (iv) in near vision tasks that have lowcontrast information, like reading a newspaper, looking at pastel-colored pictures, or writing with a pencil.
CS is the reciprocal of the contrast at threshold: the lower contrast shadows a person perceives, the higher is his/her CS. Measurement of CS resembles audiometry. The CS curve or visuogram (Fig. 9.4A) shows the contrasts perceived by the person at different optotype sizes or different widths of grating lines. There are two types of low-contrast optotype tests, (i) tests with only one optotype size and (ii) low-contrast LogMAR visual acuity charts. The most common tests with one optotype size for examination of adult patients are the Mars and the Pelli-Robson tests. When used according to the instructions, the size of the Sloan letter optotypes in the Pelli-Robson test corresponds to a low visual acuity value (20/630). The very low–contrast threshold (point A) above the broad vertical arrow (Fig. 9.4B) depicts contrast levels of faint shadows on newly fallen snow on a cloudy day, not contrast levels in everyday tasks (the same way as a high visual acuity value alone does not depict quality of vision). Measurements at the functionally important contrast levels of 1% to 5% would be easy with the Pelli-Robson or Mars test by using longer test distances, shown by thin arrows in Figure 9.4B.
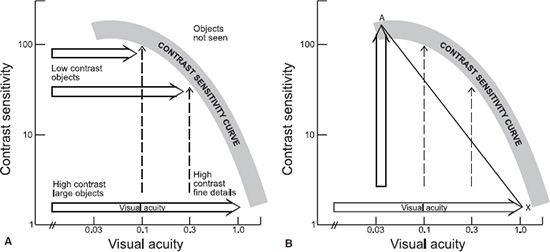
FIGURE 9.4 A: CS curve can be measured using one optotype size by decreasing contrast (the dashed vertical arrows) or using low-contrast visual acuity charts (broad horizontal arrows). B: The straight line between the Pelli-Robson contrast threshold (point A) and visual acuity at the full contrast (point X) does not depict the CS curve, whereas measurements of thresholds at longer distances (dashed vertical lines) would result in values on the slope of the CS curve and thus would define the curve. (Reprinted from Hyvärinen L, Jacob N. What and how does this child see?: Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013, with permission.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


