CHAPTER 8
Vial Preparation and Immunotherapy
RATIONALE AND BACKGROUND OF IMMUNOTHERAPY
In the mind of the public, specialty allergy care is equated with immunotherapy. Patients of all ages are familiar with immunotherapy. This treatment approach, which has been in use since about 1910 and has proved effective in a large percentage of cases, is available only from a specialist. Other approaches to allergy management are available but have drawbacks. Environmental control has always been difficult. Before the use of air conditioning (both in homes and public buildings) became widespread, environmental control represented an essentially impossible approach for the patient faced with avoiding more than a few isolated offenders. The limitations of geographic relocation have already been discussed. Although it is true that various medications have been used for the better part of a century to treat allergic problems, drugs that are truly effective in controlling allergy symptoms while being relatively free of side effects have been available for less than two decades. Even today, as noted in the discussion of pharmacotherapy, the effects of long-term use of some of the newer medications are unclear. Like environmental control, pharmacotherapy, although greatly improved in today’s medical climate, has its limitations.
The current generation is also more likely to choose immunotherapy because it has been taught to emphasize maintaining fitness and wellness, to limit costs of drugs, and to inquire about the availability of other approaches. Patients have been advised by the media to take charge of managing their medical problems to the greatest degree possible. Many patients are reluctant to take medications, which they consider foreign substances, regularly for prolonged or indefinite periods. This attitude is by no means universal, but every practitioner has heard patients voice concern about the possible risks and side effects of drugs. Although immunotherapy may be perceived as an inconvenience, it is potentially “curative,” and therefore many patients are willing to “put up with all those shots” rather than depend on medications for a lifetime.
Furthermore, patients are presented daily, through many sources, with treatment options for allergy that are outside the mainstream of standard medical practice. Although some of these approaches may eventually be validated, others remain merely ineffective nostrums that may delay appropriate treatment. Knowledgeable patients, and those educated by the physician, are generally willing to avoid such uncertain methods of management, opting instead for immunotherapy, which has been proven effective by many decades of experience.
From a more pragmatic standpoint, numerous medications for allergy control are now available over the counter, and many allergic patients have tried several of these treatments before electing to engage the services of a physician. Probably, the referring physician has utilized one or more prescription preparations in an attempt to control the patient’s symptoms. The physician offering more medications of a similar nature without at least discussing immunotherapy is likely to encounter little enthusiasm on the part of the patient. This is especially true in the present era of managed care, when referral to a specialist may be difficult to obtain. When this referral has been obtained and consultation accomplished, something more definitive in the way of care is usually expected. In most cases, the patient who has proceeded this far is prepared for immunotherapy.
Many practitioners of allergy have been concerned with the introduction of therapies such as anti-immunoglobulin E (IgE). These hold out the promise of long-term immunomodulation without the need for definitive allergy testing and years of injections. It well may be that such methods of treatment eventually will supplant conventional buildup specific immunotherapy (SIT). Already, however, it is being suggested that combining the use of anti-IgE with SIT provides better results than either alone,1 especially in patients who are allergic to multiple allergens. At present, and until long-term results prove otherwise, SIT, administered using the methods espoused in this text, remains one of the best long-term solutions for patients with severe allergy of the upper respiratory tract.
BENEFITS OF IMMUNOTHERAPY
Immunotherapy offers one benefit not provided by either avoidance or pharmacotherapy. It is the only approach that offers the probability of providing long-term, permanent relief from most or all of the patient’s allergic problems by a direct action on the immune system. Many patients are not aware of the fact that immunotherapy today is not expected to be continued for a lifetime, and that 80 to 90% of patients, properly treated, will be able to discontinue immunotherapy after 3 to 5 years and remain comfortable. Some medical supplementation may be required when allergen exposure is especially heavy, but this will usually be on an as-needed, temporary basis rather than a regular one. This makes immunotherapy a definitive approach to allergy care.
The limited and defined duration of treatment needed under an immunotherapy program has several benefits. First, albeit on a somewhat nebulous basis, it tends to reassure the somatically focused patient. Because a specific, limited treatment time is projected, the patient feels that the body is being cured rather than symptoms simply being masked. To many patients, this factor is of major importance.
Some patients are concerned about the mechanism of immunotherapy The patient may be advised that the allergens used for treatment are essentially merely the substances that are causing the allergic reactions, and not foreign material. The offenders are being presented to the patient’s immune system repeatedly in such a way that the immune system is able to adjust to the exposure and build up protection rather than experience an adverse reaction.
Patients also question why continual exposure to an allergen during the blooming season does not build up resistance. The answer is the need for higher antigen levels to accomplish this. The amount presented in a single injection of ragweed, for instance, generally exceeds the normal body exposure to ragweed during a single season. This is, of course, an oversimplification, but many patients are able to relate to it.
Clarification of another benefit of a defined and limited course of immunotherapy may require some education of both the patient and the third-party payer involved in reimbursing for care. The initial negative reaction to immunotherapy, in addition to discomfort, involves cost. Immunotherapy, including both testing and treatment, is perceived as quite expensive. It usually surprises both patient and payer to find that immunotherapy is not only the most definitive form of allergy care, but allows significant savings over a lifetime of pharmacotherapy. This cost balancing requires a little explanation. There can be no question that when all costs are considered, properly administered immunotherapy on properly selected patients is the most cost-effective form of allergy care. The operative words, however, are “properly selected” and “properly administered.” In addition to a savings on medications, other benefits that accrue to the patient treated by immunotherapy are fewer sick days, improved quality of life, and increased productivity.2
PRINCIPLES OF PATIENT SELECTION FOR IMMUNOTHERAPY
Treatment Choices
A variety of formats for providing immunotherapy are in common use. In this text, the format that will be primarily discussed is the one typically practiced by otolaryngic allergists, as well as many other physicians from other disciplines. This format is based on the principles of skin end-point titration (SET), which is the prototypical methodology for the system now more commonly known as intradermal dilutional testing (IDT). IDT-based immunotherapy is based on quantitative testing, and provides the same safety and efficiency found in the testing methodology. Before presenting the details of immunotherapy, we should first consider the results that can be expected from it, as well as details about patient selection.
Age
It is rare to find significant inhalant allergy in a patient younger than 2 years of age. There simply has not been enough time for exposure to potential allergens to have resulted in sensitization. If no significant inhalant allergy is present, it is axiomatic that no immunotherapy is indicated, as immunotherapy functions by building specific blocking mechanisms against specific allergens. If these allergies have not yet become a part of the patient’s makeup, even if the genetic propensity is there, immunotherapy will not prevent the development of allergy. Unless there is a very strong history of inhalant allergy symptoms under very specific exposure conditions, testing with a view to immunotherapy in a child under the age of 2 would be rare. It is advisable to explain this to the parents, who may well be anticipating a recommendation for immunotherapy. The physician does not want to give the impression that such a response represents a wish to avoid treating small children, which the parents may easily feel to be the case. After all, small children tend to be noisy, time-consuming, and frequently messy. They can disrupt the smooth functioning of a busy office. Children of any age, however, tend to respond extremely well to appropriate allergy care and frequently provide some of the best advertising obtainable for the new allergist.
Allergy care for the very young child should be approached initially by history and dietary regulation, as foods are a more frequent offender than inhalants in the first 2 years of life. This approach is more likely to be successful than immunotherapy, is easier for the parents to provide, and instills in the parents a feeling that the physician is sincerely motivated to provide the best care for the child. If it is necessary to demonstrate the presence or absence of inhalant sensitivity, a screening panel of allergens may be tested by the radioallergosorbent test (RAST). These allergens should always include perennials, which are the most common inhalant allergies in young children: the dust group, pets in the home, and a representative mold. If a screening RAST produces no significant responses, the test will have convincingly demonstrated that immunotherapy need not be considered. If positive responses are obtained, as avoidance and environmental control are possible for the perennial antigens, such measures should be instituted before any consideration of immunotherapy.
For the child of 2 to 5 years of age who is genetically predisposed to become allergic, inhalant allergy may be developing if the allergen exposure is heavy. As noted, usually the first sensitivity to be seen is to perennial allergens. If the child has definite symptoms of inhalant allergy at this stage of development, limited testing by either skin testing or RAST methods may reveal an allergic response strong enough to warrant immunotherapy. If such a response is demonstrated, it may be wise to inform the parents that spontaneous resolution of the condition is unlikely, as people think that most such children will “outgrow their allergies.” This impression may be the result of seeing food-allergic children improve symptomatically as the lining of the gastrointestinal tract matures, limiting the absorption of macromolecules of food that previously stimulated the immune system to produce reactions indistinguishable from those of inhalant allergy. This response to foods, known as the “leaky gut” syndrome, is not uncommon in small children and is not in anyway related to the mechanism of inhalant allergy. When inhalant allergy becomes manifest, the tendency is for the sensitivity to the established allergens to increase, and for new allergies to appear as exposure to new potential allergens continues.
Although in vitro testing is often more acceptable to parents and children, skin testing is also possible. This may be accomplished in several ways. If the child requires a general anesthesia for adenoidectomy and/or myringotomy and tube insertion, IDT can easily be done at this time, and if appropriate responses to controls are obtained, the results of testing under anesthesia can be relied upon. An alternative to IDT is the use of a multiple-prick test, but this methodology, although easier and more rapidly applied than IDT, does not provide the quantitative results that are most desirable should immunotherapy be necessary.
Immunotherapy at an early age will probably be successful, but it is necessary to realize that it is effective only for the allergens that have already produced a hypersensitivity reaction. If new allergies develop, the apparent success of the immunotherapy already under way will gradually be diminished, as only a limited number of the total offenders are being treated. The physician treating an allergic child must be prepared to test for new allergens, according to the emerging symptom pattern, and to add these to the treatment regimen when they have been identified. This may require a second treatment vial and an additional injection for a short period of time, as a maintenance level of vaccine concentration may have been reached for the allergens already under treatment, whereas a dosage escalation schedule will be necessary for the new offenders. The antigens may be combined into one vial when a maintenance level has been reached for all.
Pollen sensitivity rarely appears before the age of 5 years. When a seasonal pattern emerges, it may be time to consider an inhalant allergy screen. (If one has been done at an earlier testing and was negative, it must be considered that new sensitivities often develop as children are exposed to antigens). This testing may not be necessary if only a single season of short duration is involved, but the probability is that the single season will expand into additional seasons and may eventually become a perennial problem. Certainly if more than one season produces allergic symptoms of significant severity, the course of the allergic disease is becoming evident and demands attention. If results of the initial screening tests (described in Chapter 4) are positive, they may be expanded to include all the likely offenders. This should be done before instituting immunotherapy, as the addition of more allergens to a treatment regimen entails additional injections. Although new allergies may be expected to develop from time to time as new prolonged exposure occurs, at some point a decision must be made about the benefits of delaying definitive care to allow for the possibility of the eventual appearance of new sensitivities.
The decision as to whether or not to start immunotherapy at the earliest sign of active sensitization must be an individual consideration. If the child is not responding to dietary manipulation and environmental control, if the symptoms are severe and not controlled easily by medication, or if the patient reacts poorly to medical therapy, immunotherapy may be indicated. If this is not the case, it may be advisable to defer immunotherapy until the patient is a little older.
Although new problems may develop with time, there is an additional benefit to instituting immunotherapy in children as soon as a significant pattern of allergic disease has been identified. This is the reduction of the “total allergic load,” a condition related to the “priming effect.” The more uncontrolled allergy that is present, the greater the symptoms that are produced by the same allergen exposure. Priming is the phenomenon whereby at the start of an allergy season, high degrees of allergen exposure may be needed to produce symptoms, whereas toward the end of the season, a minor exposure will produce severe symptoms. Priming may also cause exposure to minor allergens to result in marked symptoms, although such exposure produced no symptoms at the start of the season. The patient’s immune system has become “primed.” By the same token, in the patient whose allergic problems have been brought under control, severe symptomatology is much less prone to develop after new exposures because the allergic load has been reduced.
Avoiding priming and minimizing the total allergic load allows the allergist to treat for a more limited number of key antigens, concentrating on the more severe offenders and still obtaining good results. It should be evident that it may be impossible (and certainly impractical) to treat routinely for every major and minor allergen to which a patient has any degree of sensitivity. For example, antigenic extract may not be available for some of the more minor substances, and other allergens may not be evident to the investigator. Cross-reactivity, significantly further reduces the total number of allergens needed for treatment, so that immunotherapy with a reasonable number of antigens is effective.
The previous discussion has been directed primarily at considerations of immunotherapy for the developing child, but many of the same considerations are equally applicable to the allergic adult. Allergy may appear at any time in life, and when the criteria described are met, immunotherapy is one of the treatment modalities warranting consideration.
Season and Circumstances
Immunotherapy is a valid means of therapy for inhalant allergy, but it may not always be the best choice. Not every patient demonstrates the same progression of disease; the rapidity of the progression and degree of symptom expression are highly variable. For the patient who has symptoms only on specific exposure to avoidable antigens, such as the cat-sensitive patient, careful avoidance and environmental control may be all that is needed. The patient with symptoms only during the relatively short tree-blooming season, for example, may find medical treatment to be entirely adequate. The exception is the patient who responds poorly to medication and resists taking any such medication, either because of side effects or merely personal preference. These patients may request immunotherapy, and there is no reason to deny their requests, as the immunotherapy should be as effective as that given to patients with multiple-season symptoms. The ideal candidate for immunotherapy, of course, is the patient whose symptoms have progressed to last 6 months or more of the year and who is young enough to anticipate many decades of problems requiring treatment of some type.
Patient Cooperation
For the full benefits of immunotherapy to be achieved, the patient must be prepared to cooperate in the program. Achieving this cooperation requires a significant degree of discussion with the patient before such a course is undertaken, usually augmented by some printed material that may be reviewed by the patient at regular intervals, and continued by members of the allergy team as immunotherapy progresses. It is best to identify potential “dropouts” before treatment is begun. Immunotherapy may be the most cost-effective form of allergy care, but this is true only if a full course of treatment is performed.
One of the major benefits of immunotherapy, and also one of the factors most subject to misunderstanding on the part of the patient, is the early response to treatment usually seen in patients treated by immunotherapy based on IDT. Because treatment for each antigen is started at the highest concentration found to be safe by testing, beneficial results are frequently seen within a matter of several weeks. This response may represent a double-edged sword. The benefits are evident: prompt improvement, even during a major allergy season, with little potential risk for reactions. The drawback is the tendency of the patient to feel that because improvement has occurred, further treatment may safely be neglected. Stopping treatment too early is not dangerous to the patient’s health, but it definitely negates the potential long-term benefits of this form of treatment. Likewise, the allergist must not be lulled into a false sense of security by early favorable results from immunotherapy, holding the dosage at a symptom-relieving level. As will be pointed out later, escalation must continue past this early stage.
Years ago, before the current degree of understanding of the mechanism of immunotherapy was reached (it is still far from complete), it was recommended that allergy patients undergoing immunotherapy continue their injections throughout life. Allergy was known to be a genetically determined condition, and it was assumed that such a problem would be irreversible. Within the past decade or more, it has been determined that providing immunotherapy at high dosage levels during a period of about 3 to 5 years will, in the vast majority of patients, produce an immunologic response that makes further immunotherapy unnecessary. The exact nature of this response is still unclear. The effects now known to occur include a gradual decrease in allergen-specific IgE and increase in specific IgG, an increase in allergen-specific suppressor T cells, a decrease in proallergic cytokines, and a decreased reactivity of both basophils and lymphocytes to antigens. Currently, a treatment regimen of 3 to 5 years of immunotherapy, with at least 1 year at maintenance level, is still recommended. It is not yet known with total certainty how long immunotherapy must be administered without a risk for regression when it is discontinued, and most investigations of this question thus far have involved treatment with a single antigen, a concept not favored by most oto-laryngic allergists.
Time Requirements
If a patient does not continue treatment as long as is necessary for a more permanent reversal of the allergic process to develop, immunotherapy must be resumed when the initial beneficial effects disappear. If the process of prematurely discontinuing therapy is repeated, the same result may be expected. This sequence does not harm the patient, but it reinforces the earlier, erroneous concept of lifetime dependence on immunotherapy. When inadequate or repeatedly interrupted immunotherapy is administered, the cost benefits are lost. In our modern climate of managed care, it is often necessary to emphasize to a third-party payer the benefits of covering immunotherapy care on the basis of the limited and finite time needed for such care. The coverage for immunotherapy must be weighed by the third-party payer against a lifetime of symptom-relieving medication, which is not inexpensive. If this long-term benefit of immunotherapy provided for 3 to 5 years is not evident, it would not be surprising to see a denial of all coverage for immunotherapy.
The selection of patients for immunotherapy, as for all other forms of therapy, depends heavily on patient commitment and is strongly influenced by information supplied by the physician. Immunotherapy is an excellent form of treatment, and probably the best choice currently available for the management of inhalant allergy. Its greatest benefit, however, is the potential for long-term success after a well-defined period of treatment. The time and dedication that the patient is prepared to commit to immunotherapy directly affect the degree of success that may be expected. A patient in transit or who travels often, for example, and thus who cannot or is not willing to follow through on regular injections, is a poor immunotherapy candidate. Improvement may occur even with sporadic injections, but it will rarely be maintained. A patient with a history of starting allergy injections but discontinuing them after a few months will not often benefit from immunotherapy to the degree expected. The unfortunate part of this situation is that the patient usually blames the failure either on the physician directing the treatment or on the treatment modality itself. After a few failures, it is difficult to persuade the patient to accept responsibility for the poor result and again commit to a trial of therapy of the same basic type. Even if the patient listens closely to the new information provided and takes more printed material home to study at leisure, the commitment professed often weakens over a period of time. This is not to say that no successful responses to immunotherapy ever occur in such patients, but the physician should be alerted to the likelihood of another failure through no fault on the part of the clinician. Failures breed guilt, and the new allergist is especially susceptible to such situations. For some reason, patients who have failed in the past to respond to competent therapy because of poor compliance tend to converge on the new allergist. This may be a consequence of rejection by those who have previously initiated proper therapy, only to see minimal compliance produce failure, or of an eternal search on the part of such patients for a quicker, simpler form of treatment that entails no need for cooperation on their part. Regardless of the reason, the physician just starting to offer good, comprehensive allergy care may expect to see an unusually high number of poor-risk patients in the practice’s early stages. This may, but should not, discourage the properly trained clinician utilizing appropriate techniques from pursuing this new aspect of practice.
NURSE’S NOTE
Testing has been done. Results indicate that the patient is allergic, and the patient has symptoms that correspond with the test results. Furthermore, the patient is willing to follow through a course of immunotherapy that will last 3 to 5 years. It is time to prepare for treatment. However, at this point, the allergy care provider should again go over the anticipated benefits of immunotherapy, remind the patient (and the family, if the patient is a child) of the commitment of time and effort necessary, explain the usual time course involved of 3 to 5 years, and be certain that the patient’s expectations of the results of immunotherapy are realistic, It is always better to do this at the time immunotherapy is begun than to deal with problems that arise later from unrealistic expectations or lack of understanding.
SPECIFIC INDICATIONS AND CONTRAINDICATIONS FOR IMMUNOTHERAPY
The administration of immunotherapy is predicated on the patient’s meeting the criteria for an acceptable candidate for such treatment. Such patients should have proven atopy (mediated by IgE) to one or more antigens that are not readily avoidable. They should have symptoms that are inadequately relieved by pharmacotherapy, or should be intolerant to pharmacotherapy (because of side effects or other considerations). Their symptoms should be multiseasonal, spanning more than one allergy season, or if present during only a single season, the symptoms should be severe. The patients should be motivated and likely to be compliant with a program of allergy immunotherapy.
Indications
Although the best treatment of inhalant allergy is avoidance, there are many circumstances in which complete (or even effective partial) avoidance of an inciting allergen is impossible or impractical. Each case must be considered on its own merits, and patients should not be denied immunotherapy simply because the allergist feels that they “should” be able to avoid their antigenic triggers. The classic example is the cat owner, who would rather part company with the allergist than with the cat. At times, rigid adherence to best practice must be tempered with an understanding of the complexities of the human character.
The admonition to treat only multiseasonal allergies with immunotherapy is firmly entrenched in tradition, if not in science. However, given the track record of safety and effectiveness of the methods for testing and immunotherapy described in this text, patients with single-season allergies (especially if severe) should be considered for definitive treatment by allergy immunotherapy.
Some patients are content to utilize various pharmacotherapeutic measures to relieve their allergic symptoms, and if such treatment is not disruptive of their lifestyle and they experience no adverse effects, there is no need to press the matter of immunotherapy. As a practical matter, most patients don’t like to take pills or use nasal sprays on a regular basis, and are happy to consider a therapeutic program that may eventually allow them to use their medications less frequently or not at all. Although great strides in the pharmacotherapy of inhalant allergy have been taken in the past 50 years, the search continues for medications that are free of potential side effects, drug interactions, or other adverse effects.
It is important for the physician, nurse, or some other member of the allergy team to counsel patients before immunotherapy, frankly detailing the expenditure of time, effort, and money involved. A great deal of needless frustration can be avoided if immunotherapy is begun only after a joint commitment on the part of both patient and health care provider.
Contraindications
The only absolute contraindication to allergy immunotherapy is the absence of allergy. In addition, patients who test positive for human immunodeficiency virus (HIV) are not good candidates for immunotherapy, as its efficacy in these patients is uncertain and it does not appear desirable to administer treatments aimed at immune modulation in this situation. Relative contraindications to the initiation of immunotherapy (requiring a decision based on individual circumstances) include β-blocker therapy, pregnancy, and immune dysregulation.3
It is unusual, but not impossible, to encounter HIV-positive patients with severe nasal allergic symptoms. For these patients, symptomatic control should be sought through appropriate pharmacotherapy. Only if prolonged systemic corticosteroid therapy is required for the management of allergic symptoms in such patients is consideration of immunotherapy justified.4
It appears that patients receiving β-adrenergic blocking drugs may be more prone to severe allergic reactions (from any cause) than other patients.5 Beta blockade may be “proallergic” through blocking smooth-muscle relaxation (contributing to possible bronchospasm) and amplifying production of various mediators of inflammation produced in an allergic reaction. Although some question exists as to the exact degree of increased risk, it is probably even more important to realize that noncardioselective f$ blockers significantly affect the possible treatment of an anaphylactic reaction, should one occur during testing and treatment.6 If epinephrine is given to a patient in the presence of a β-adrenergic blocker, unopposed α-adrenergic stimulation may occur, resulting in a hypertensive crisis. This is discussed in detail in Chapter 11. It is prudent to discuss with the patient’s primary care physician a possible change to another agent, such as a calcium channel blocker, angiotensin-converting enzyme (ACE) inhibitor, or diuretic, before skin testing and initiation of immunotherapy. If this is not possible, a switch to a cardioselective β blocker may reduce the risk for potentiating bronchospasm, but it does not alleviate the possibility of an enhanced hypertensive response to epinephrine.
It is generally accepted that immunotherapy that has been initiated before pregnancy may be continued during pregnancy.7 It is unwise to begin immunotherapy in a pregnant patient for several reasons, however. First, it is likely that the degree of sensitivity of the patient will vary with the immunologic changes that occur during pregnancy. Thus, levels of reactivity determined during pregnancy may be inaccurate after delivery. More importantly, there is a very real risk for hypoxia and fetal damage if the mother experiences anaphylaxis. Because most reactions to immunotherapy occur during initiation and dose advancement, subjecting a pregnant patient to this risk is ill-advised. On the other hand, patients who are receiving immunotherapy and become pregnant may continue to receive their injections (with the approval of the obstetrician). It is best not to attempt to increase the dose of antigen administered during this period, but maintenance therapy is generally considered to be safe.
The question of immunotherapy in patients with autoimmune disorders remains controversial.8 Although immunotherapy has not been definitely shown to cause or worsen autoimmune disorders, sufficient questions have been raised in this regard to require a thorough consideration by such patients and their physician of the risk-to-benefit ratio of immunotherapy for inhalant allergy.
PREPARING THE TREATMENT EXTRACT
The decision has now been made to treat the inhalant allergic patient by immunotherapy. Before the treatment is started, a vial of treatment extract must be prepared specifically for the patient to be treated. This should be done in advance of the first treatment visit, with the same care and freedom from interruptions required for proper preparation of testing dilutions. This vial serves to initiate treatment and to allow early progression of immunotherapy toward a point of symptomatic relief. It would be rare to have this first treatment vial represent a final level of maintenance, but unless problems arise, the preparation of successive treatment vials of increasing strength is based on the formula used in the initial vial.
For the beginning allergist, treatment vials may be made directly from the testing board. Later on, as the patient volume increases, it may become desirable to make a separate board for treatment, using larger vials or extract with the same fivefold dilution prepared in the testing board but with all successive dilutions containing 10% glycerine as a preservative. This is not necessary at the start, and many allergists prefer always to make their treatment vials from the testing board, adding glycerine to the vial after preparation to bring the glycerine concentration to 10% or above. This concept will be clarified shortly. Initially, let us concentrate on the procedure for making the initial treatment vial.
The treatment format is based on IDT, taking advantage of the relative quantification of sensitivity to the various allergens and highest safe initial dose provided by this testing procedure. It has been established that the end point identified by this form of testing is a safe level at which to initiate immunotherapy for any specific allergen.
Treating for a Single Allergen
Strictly speaking, treatment of a single allergen need not be discussed under preparation of vials for therapy. There is really no need to prepare a vial to treat a single allergen. Such patients may receive treatment from the stock antigen vial on the board. For teaching purposes, however, we begin by considering treatment with one antigen.
It has been established that the end point is a safe level at which to initiate treatment. In establishing this end point, several negative wheals have been produced, all containing minute amounts of antigen insufficient to initiate an immunologic reaction. Then the end-point wheal was produced. This wheal contains 0.01 mL of extract, the amount necessary to produce a 4-mm wheal. A confirmatory wheal has also been produced from the next stronger dilution. This wheal contains the same 0.01 mL of extract, but it is five times more concentrated, making it the equivalent of 0.05 mL of the extract producing the end point. Thus, during testing the patient has received 0.06 mL of the end-point extract, plus an additional small amount from the negative wheals. If no adverse reaction has occurred during testing, it may be assumed that it is safe to administer 0.05 mL of the end-point dilution as an initial treatment dose. The first treatment dose, therefore, is 0.05 mL of the end-point strength.
To treat for a single antigen, this dose may be drawn from the vial producing the end point and administered subcutaneously. Such treatment injections are given subcutaneously for slower absorption and greater patient comfort, using (if available) special treatment syringes rather than those used for skin testing. Successive doses may be drawn directly from the testing vial and given as described previously. There is no need to prepare a treatment vial unless the patient is to take it elsewhere for therapy, in which case the same procedure used in preparing a multiple-antigen, multiple-dose vial is followed.
NURSE’S NOTE
Two reminders are necessary. First, the larger the number, the more times the antigen has been diluted. Second, the larger the number of the patient’s end point, the higher the patient’s sensitivity (and the greater the need for caution). For this reason, antigens at #4, #5, and #6 strengths are frequently placed in a vial separate from the #3, #2, and #1 strengths. This allows greater flexibility in adjusting doses.
Preparing the Multiple-Antigen, Multiple-Dose Vial
The vast majority of patients requiring immunotherapy are sensitive to several allergens. Theoretically, treatment for any number of allergens could be performed exactly as described for single-allergen treatment, starting each allergen treatment with a 0.05-mL dose of the extract producing the end point. Practically, this would involve multiple injections of different allergens at each visit, which is unpleasant for the patient. The simplest solution to this problem would be to place 0.05 mL of each antigen in the same syringe and give it all as a single dose. This approach, however, is also impractical, as the total quantity of extract used in adding 0.05 mL of the end point of 10 or 15 different antigens quickly produces a larger amount of fluid than is comfortably tolerated in a single injection. Furthermore, the amount would increase even more with each successive injection while the treatment dose is escalated. What is needed is a means of reducing the volume of extract while preserving the potency needed to equal that of the end point of each antigen, allowing escalation without an undue increase in volume. Each injection should also contain all the antigens to be treated for in a single dose. Although this may seem like a monumental project, it is actually quite simple to carry out after the principle is understood.
The principles used in both testing and treatment by IDT are based on certain human limitations, specifically the ability to measure wheals accurately and to measure minute quantities of extract contained in a syringe. Whenever the logistics of vial preparation are described, the question of why the calculations cannot be shortened, with certain steps skipped, always seems to arise. Decades of experience in teaching the fundamentals of oto-laryngic allergy have shown that any such shortcuts invariably produce a poor understanding of the process, resulting in problems in vial preparation. Adhering to the proven format gives a uniform, reproducible system that experience has shown to be effective. When the process is firmly understood, measures to make it more efficient may be considered.
Testing requires that extracts be diluted in such a way that wheals of a uniform size, which can be produced repeatedly, will respond uniformly. Treatment requires concentration of the same extracts in such a way as to allow for easy, reliable measuring for vial preparation and injections. The fivefold dilution that is made for testing is basically reversed to provide the material needed in treatment.
STEP 1: CALCULATIONS AND PROCEDURE TO MAKE THE INITIAL TREATMENT VIAL
The results of IDT are recorded on a testing sheet indicating the end points identified for each allergen (Fig. 8-1). At the right side of the sheet, immediately after the numbered columns, is a column in which the end points identified by testing are recorded. From these end points, the calculations are made to determine the contents of the treatment vial.
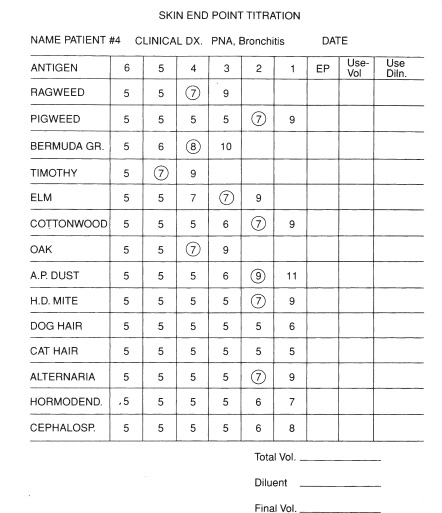
Figure 8-1 Completed titration sheet for skin testing.
The definition of the end point for IDT has been covered in Chapter 5. Briefly, the end point of titration represents the antigen strength that produces the first positive (reacting) wheal followed by progressively larger positive wheals; that is, the end-point concentration is the dilution that initiates progressive positive whealing.
Even if the initial testing has been done by RAST (used here to refer to a quantitative in vitro method, whatever the marker employed), the principles involved in vial preparation are based on IDT In the past, it has been popular to utilize different methods to calculate vial composition when testing has been done by in vitro methods such as RAST This is unnecessary. One of the major advantages of the Fadal-Nalebuff modified RAST (F/N mRAST) is that the increments of that scoring system match the fivefold dilutions determined by Rinkel in his modified titration system to yield the most accurate and reproducible results. Experience has shown that F/N mRAST classes parallel the end-point classes in IDT, although the results of IDT generally indicate sensitivity about one class greater than is found by F/N mRAST In other words, an end point by IDT of #5 would correspond to an F/N mRAST class IV. For further explanation of this relationship, the reader is referred to Chapter 10. This correlation may also exist with other in vitro methodologies, but the practitioner will have to ascertain whether such is the case before utilizing those results in preparing vials by this method. Because of this relationship, if vials are to be prepared from RAST results instead of IDT, one may substitute in the end-point column a number equal to the RAST class score plus one. Because a higher number indicates a more dilute solution, this has been called a RAST minus one level, but actually it represents the addition of one to the RAST score. This has been a source of confusion to many novices, but the terminology is firmly entrenched in the literature and in tradition. For a RAST class IV response, the end point 5 would be entered. Vials may then be prepared in the usual fashion.
The mathematical calculations needed to determine the volume and specific dilution of each antigen that must be placed in the treatment vial are simple and very basic. It is important, however, to understand the principles behind these calculations, as at some time it may be necessary to make a change in the procedure. This may occur, for instance, as a result of the developing standardization of extracts. Alterations in the set formula are required should the physician wish to make a smaller or larger treatment vial to accommodate the needs of particular patients. The format presented has been developed to require the smallest number of calculations practical, and to correlate the calculations with the established fivefold dilution format to avoid confusion. Repeated studies have shown that the new allergist or the technician preparing the treatment vials is able to follow this format with a minimal risk for error. This simplicity is of special benefit during training of a new allergy assistant. It is not the most economical method of preparing a treatment vial (because the examples involve 5-mL vials), but the minor waste of antigen in the early stages of practice is more than compensated for by the simplicity of the preparation and reliability of the result. The concept of a 0.5-mL maximum injection size has been utilized because that is the maximum volume that can be comfortably tolerated by most patients. After the methodology is firmly understood, vials of any size, utilizing therapeutic injections of any amount, may be prepared using the same principles.
The principles involved in preparing the vial are as follows:
1. The extract should be concentrated as much as possible to reduce the volume of fluid in the injection while maintaining the amount of antigen to match the end-point concentration.
2. It would not be productive to prepare a new antigen mixture each time the patient is due to receive an injection. A reasonable number of escalating injections should be planned and prepared at the same time in the same vial.
3. To treat patients properly with immunotherapy, during escalation each injection should normally contain a greater amount of antigen than was contained in the previous injection. This escalation schedule, which may vary, is discussed later (see Escalating the Treatment Dose). How many injections are actually contained in a single vial will vary, but an arbitrary number must be selected to prepare the vial. For ease of understanding the calculations, the number of injections selected for calculation purposes is 10.
4. When a dose of 0.50 mL is delivered from the first vial, it corresponds to a dose of 0.10 mL from the next stronger vial because the contents of the new vial are five times stronger than the contents of the first. This means that instead of raising the injection volume from the first vial above 0.50 mL, one may (and should) proceed to the next stronger vial, which further reduces the fluid volume without altering the amount of antigen present. This will become clearer when escalation of doses is discussed. For the present calculations, what is necessary is to understand that the maximum dose normally delivered from a vial will not exceed 0.50 mL. Doses above this level will be delivered from a new vial that is five times stronger than the first. (Because the new vial is fresher, and theoretically slightly more antigenically potent, the first injection out of that vial is typically 0.05 mL, rather than 0.10 mL, a variation that is discussed more in detail later.)
Now for the calculations: We would like to reduce the volume of each antigen put into the master vial as much as possible without altering the amount of antigen present, so that we can add all the positive antigens together in a convenient volume and bring the total volume up to the desired amount. This can be done by removing diluent from the injected material. If we prepare a vial from bottles that contain five times less diluent per milliliter than the end-point vial, we end up with an extract that contains more antigen per milliliter, so that 0.1 mL of the new vial contains the antigenic equivalent of 0.5 mL from the end-point vial. Using as a stock vial one that is two fivefold-dilutions stronger than the vial producing the end point provides another reduction of five times the amount of diluent. This concentration is 25 times greater than the end-point dilution (with the same antigenicity) and represents about as much concentration as is practical while still allowing accurate measurements to be performed. The mathematical calculations would be, for example, as follows: 0.50 mL of a #6 (1:312,500) dilution equals 0.10 mL of a #5 (1:62,500) dilution equals 0.02 mL of a #4 (1:12,500) dilution. The amount of antigen in each successively reduced amount of extract is exactly the same (Fig. 8-2).
The patient will receive increasing doses, up to a maximum of 0.5 mL, from the initial treatment vial. The second calculation determines the amount of each antigen needed to provide what has been estimated to be a reasonable number of doses, to be included in the initial treatment vial. To illustrate this calculation, we will assume the amount to be 10 doses of 0.5 mL. This amount of extract in the vial will probably not actually be used, but placing such an amount in the vial provides more than enough properly mixed extract to allow for all the injections necessary from this vial before it reaches its expiration date, and the calculations using this amount are simpler.
We need to calculate the amount of extract from each vial of antigen, at a concentration two dilutions stronger than the vial producing the end-point dilution, to provide 10 doses of 0.5 mL each. This simply requires multiplying the amount needed for a single maximum injection of 0.50 mL by 10. We have already determined that 0.02 mL of extract from the vial two dilutions stronger than the vial producing the end point is equivalent to 0.50 mL of the end-point vial. Then, 0.2 mL (0.02 X 10) from the vial two dilutions stronger will supply the amount of antigen needed for 10 doses of 0.50 mL of the end-point dilution. All that has been removed is diluent. The calculation simply involves determining the strength of the end-point dilution of each antigen, increasing that strength by two concentrations, taking 0.20 mL of extract from this vial, and placing it in a treatment vial (Fig. 8-3). The same calculations are valid for all antigens, although in some instances (such as with standardized antigens or antigens that do not come in 1:20 weight/volume [w/v] stock concentrations), correction factors must be applied.
An added advantage of the system described is the ease of measuring small volumes of extract. Although 0.02 mL is essentially impossible to measure accurately, 0.20 mL may be measured with considerable accuracy by a diligent nurse or technician.
After 0.20 mL of each antigen for treatment has been placed in the treatment vial, an appropriate amount of diluent must be added to the vial. The previous calculations have been described for preparing a 5-mL vial. Enough diluent must be added to the vial to bring the total contents of the vial to 5 mL. This merely requires adding the volume of antigen (in milliliters) already placed in the vial, subtracting that from 5 mL, and adding that amount of diluent.
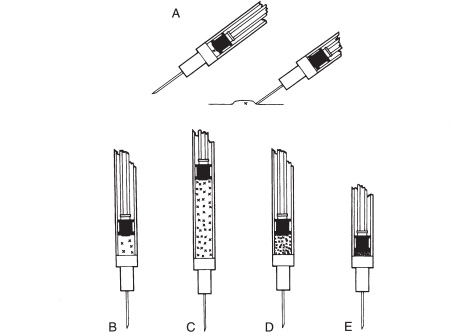
Figure 8-2 Concentrating an antigen dose: A: Although 0.01 cc cannot be accurately measured, it has been shown to produce a 4-mm diameter wheal, so that skin testing applies a known amount of antigen in determining the end point. B: An injection of 0.05 cc is the usual starting antigen dose, whereas C, 0.50 cc is the usual maximum volume injected. The process of vial-making takes advantage of the fivefold relationship between antigen dilutions. The antigenic equivalent of 0.50 cc of a given concentration (C) is contained in 0.10 cc of the next stronger concentration (D) and in 0.02 cc of the concentration that is yet fivefold more concentrated (E). Although 0.02 cc cannot be accurately measured, one can prepare a vial containing 10 doses of 0.50 cc by placing 0.20 cc (10 multiplied by 0.02) of each antigen at two concentrations stronger than the end point in the vial, and adding diluent to bring the volume to 5 cc. (With permission from Cowen DE, Dixon BJ, revised by Ward WA. Skin End Point Titration Technique [manual]. Washington, DC: American Academy Oto-laryngic Allergy; 1980;4.)
It has been found by experience in numerous courses and teaching situations that making a 5-mL vial in this manner presents few problems for the novice. When the calculations of students have been checked, a tendency to err has appeared when additional calculations have been introduced. Most of these errors involved a failure to carry out consistent mathematical calculations through the entire process. Whatever the reason, the problem has appeared frequently enough to result in the development of the format presented. It is simple, easy to teach to a new physician, nurse, or technician and easy for any colleague employing IDT to understand whether a patient must be transferred to another physician. The beginning allergist is strongly advised to follow the procedure described scrupulously, at least in the earlier stages of the practice; it also has many benefits when continued indefinitely. When necessary, it is quite possible for the experienced technician to use the same methods to produce larger or smaller vials, as well as vials that deliver more or less antigen in the same volume.
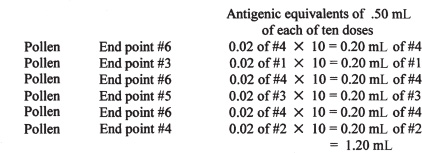
Figure 8-3 Summary of the calculations necessary to make a multiple-dose, multiple-antigen treatment vial. Diluent is added (in this case, 3.80 mL) to bring the volume back to 5.0 mL. (With permission from Cowen DE, Dixon BJ, revised by Ward WA. Skin End Point Titration Technique [manual]. Washington, DC: American Academy Otolaryngic Allergy; 1980;4.)
STEP 2: PREPARING THE ACTUAL VIALS AND CALCULATING DILUENT
Dividing the Vials
The preceding section has explained the concept and described the steps involved in preparing a single treatment vial. These must be understood before the steps outlined later for making vials to treat sensitivity to multiple antigens can be understood. In most cases, the allergic patient will demonstrate a variety of sensitivities to multiple antigens of different strengths on testing, all of which require treatment. Often, a wide range of sensitivities will be present: IDT end points at #6 and #2 or RAST responses ranging from class V to class I. It should be noted here that IDT end points on #1 or RAST class O/I sensitivities are not always considered indications for immunotherapy unless the symptom pattern strongly indicates a relationship between the weak responses and the patient’s symptoms.9 With IDT, it is also necessary that the response from a #1 dilution exceed the wheal diameter for the 10% glycerine control (because this is the glycerine concentration in a #1 dilution), indicating that the reaction is immunologic, not irritative. It is quite possible to place many or all of the individual antigens usually needed for treatment at varying concentrations in the same treatment vial. This is not an ideal solution, however.
Although IDT indicates a safe starting point for initiating therapy for each antigen, it does not establish the treatment level needed for maintenance. This is established clinically. Allergens with higher end points (e.g., IDT #6, RAST class V) generally represent a higher level of sensitivity, and these allergens require therapy to be started at considerably more dilute doses than allergens with end points indicating less sensitivity (e.g., IDT #2, RAST class I). In addition, the allergens to which the patient is most sensitive are more likely to precipitate an adverse reaction during immunotherapy, and therefore must be treated with more caution. Because treatment for the allergens with high end points must be started at a more dilute level, more injections will generally be necessary for these allergens before maintenance doses are reached. For all these reasons, it is more efficient to start treatment with two vials rather than one: one vial containing the allergens with high end points (IDT #4, #5, #6 or RAST classes III, IV, and V) and the other vial containing allergens with low end points (IDT #2 and #3 or RAST classes I and II). Injection doses from the two vials may then be increased individually until maintenance levels of therapy are reached, as discussed later. If a single vial containing all the antigens is used initially, it will often be necessary to divide the vial at some point early in treatment because of local reactions. Starting initially with vials for high and low sensitivity avoids this problem.
Number of Antigens per Vial
The question usually arises as to how many antigens should be, or can be, placed in a single treatment vial. Simple mathematics will give the answer to the second part of this question. Adding 0.2 mL of each antigen to a vial allows a total of 25 antigens to be placed in a 5-mL vial, with no room for diluent. Such a situation rarely, if ever, arises. If such a high number of antigens are placed in one vial, one immediate problem must be considered. Stock vials of antigens are normally purchased in a 50% glycerine solution. Glycerine is an excellent preservative, but it is also quite irritating. This is the reason why a glycerine control is needed during testing. You will recall that this consists of 2% and 10% glycerine solutions, representing the amount of glycerine contained in the #2 and #1 IDT testing dilutions, respectively. If a treatment vial contains a large number of antigens taken from concentrate or the #1 dilution, the total glycerine level may easily exceed 10%. Injections containing this much glycerine are almost guaranteed to produce a local irritation. This is not harmful, but a local reaction is normally the earliest indication that a maximum tolerated dose has been reached. If such a reaction were the result of glycerine irritation, dose escalation would be halted on the assumption that the injected antigens were producing the local reaction, and treatment would not be carried to an appropriate maintenance level. If a quick mathematical calculation shows that a vial will contain more than 10% glycerine, it is well to divide the vial. In some instances, when a large number of antigens are treated using concentrates for preparation, it may even be advisable to divide the antigens among three vials. An alternative, of course, would be to draw up a small amount of diluent into a syringe, and then draw the amount to be injected from the vial, to dilute the glycerine in the injection. This should never be done in the reverse order, for fear of contaminating the diluent vial with antigens carried into it in the tip of the syringe from the treatment vial.
Diluents
This brings up the question of the amount and type of diluent appropriate for a treatment vial during initial treatment and dose escalation. In this respect, more than one approach is possible. Several diluents are available for both testing and treatment mixes. By far the most widely used is buffered pheno-lated saline solution.
Human serum albumin (HSA) has previously enjoyed some popularity for the preparation of testing vials, but it is more expensive than saline solution. Contrary to popular belief, HSA does not act as a preservative. HSA provides only one advantage, the reduction of “walling,” which is the tendency of small amounts of extract to adhere to the walls of a glass vial. This feature is of no real importance in therapy, and of little consequence in testing. In addition, the public has become concerned about the use of blood products, fearing the possibility of transferring viruses such as hepatitis virus or HIV. In point of fact, commercially prepared HSA is heated above the temperature at which pathogenic viruses can survive. Nevertheless, HSA has little to recommend it for routine use as a diluent.
Buffered saline solution contains 0.4% phenol to prevent any viral or bacterial growth, and it is buffered to match the pH level of human blood. It does not contain a preservative, and antigens mixed with buffered phenolated saline solution alone may be expected to maintain full potency for only 6 weeks if kept refrigerated when not in use. This is the reason why all testing boards should be remade every 6 weeks, replacing all dilutions starting with #1. No additional glycerine is ever added to a testing vial, as the glycerine alone may produce a skin reaction, obscuring any allergic response. In preparing treatment vials, however, another option exists.
In the initial stages of treatment and while escalating doses, there may be an advantage to not adding glycerine to the treatment vials. One of the indications that the maximum tolerated dose is being approached is the presence of a local reaction at the site of an injection. If no glycerine has been added to the vial, such a reaction may be assumed to be a consequence of immunologic activity, and the level of the vial producing the local reaction can be maintained (or even decreased) for the time being. Proceeding in this manner provides a simple indicator of progress and a clear point at which to evaluate treatment results. This may be a real benefit to the treating physician, especially the novice. The limitation of this approach is that the vial being used in treatment maintains its potency for only a little more than 6 weeks, even when refrigerated, and therefore if the escalation is still proceeding after 6 or 7 weeks, the vial must be discarded. If the patient is on a schedule of two injections a week, this is usually not a problem. However, if the injections are given at weekly intervals, the potency of the extract may become significantly reduced by the time it is necessary to advance to the next stronger vial.
When preparing treatment vials, it is often helpful to be certain that the vial contains a glycerine level of 10%. In this way, the potency of the vial is maintained for at least 3 months, and sometimes longer. In some instances, this may involve using 10% glycerine as a diluent. A simple way to prepare a large bottle containing 10% glycerine is by diluting a stock bottle of 50% glycerine (which may be purchased separately from the allergy supplier) in the proportion of 1 mL of 50% glycerine to 4 mL of buffered saline solution (i.e., a 1:5 dilution), just as is done in making a glycerine control. (In the future, the 10% glycerine control may be taken from this stock bottle, and a 2% glycerine control may be made by a further 1:5 dilution with buffered saline solution.) When all antigens have been placed in an empty treatment vial, a quick calculation will show about how much glycerine is already in the vial, based on the strength and number of antigens that have been placed in the vial.
The glycerine content of the vial can be calculated easily if one considers that antigens added at concentrate level contain 50% glycerine. Because 0.2 mL of each antigen is added to a vial that will ultimately contain a volume of 5 mL, if five antigens at concentrate level are added, five multiplied by 0.2 equals 1 mL of 50% glycerine. Adding 4 mL of diluent (or other antigens containing less glycerine) leaves a final concentration of 10% glycerine in the vial. Therefore, if five or more antigens at concentrate level are contained in a 5-mL vial, no additional glycerine need be added. If more than one but fewer than five antigens at concentrate level are present, the difference between the volume from these antigens and a total of 1 mL may be made up by adding 50% glycerine. In other words, if two antigens at concentrate are present, they provide 0.4 mL of 50% glycerine. Add 0.6 mL of 50% glycerine from a stock bottle, then add other antigens and diluent to a total volume of 5 mL. If no antigens at concentrate level are present, using 1.0 mL of 50% glycerine as diluent for a 5-mL vial brings the glycerine concentration to at least 10%.
Some local reactions may be expected from injections from vials with a glycerine content of 10% or greater, but they will generally be minor. A marked increase in local reactions indicates a treatment level close to a maximum tolerated dose. If a large number of antigens at concentrate level have been placed in the treatment vial, the amount of glycerine in the vial may already be high. In this case, only saline solution need be added. All vials to be used for maintenance therapy may be prepared in this manner to maintain potency for at least 3 months, which usually allows the vial contents to be exhausted before the expiration date.
NURSE’S NOTE
It is imperative that the person preparing treatment vials thoroughfy understand the concepts just presented. This review allows the process to be seen from a second viewpoint, although the principles are exactly the same.
For ease in calculations, a 5-mL vial will be prepared containing 10 doses. To allow several antigens to be mixed in the same vial, providing a dose in a quantity that the patient can easily tolerate, the antigen strength is concentrated 25-fold. The antigens (in concentrated form) are then mixed, and difuent is added to reconstitute them. This is the beauty of a fivefold dilution system: 5 mL of #4 (1:12,500) equals 1 mL of #3 (1:2500) equals 0.2 mL of #2 (1:500).
Each antigen is added to the vial in the strength (determined by the IDT or RAST end point) that indicates a safe starting point. Suppose we wish to make this vial:
Timothy grass #4 (1:12,500)
Ragweed #3 (1:2500)
Oak tree #2 (1:500)
Dust mite #2 (standardized extract; see later)
Each antigen would be taken at two concentrations stronger, so that we would use the following: Timothy grass #2 (1:500) Ragweed #1 (1:100) Oak tree concentrate (1:20) Dust mite concentrate (standardized extract; see later)
For standardized extracts, a rule of thumb is that a strength of 30,000 allergenic units (AU) or bioequivalent allergy units (BAU) may be used as concentrate, whereas a strength of 10,000 AU or BAU is integrated into mixing as though it were a #1 (1:100) concentration.
To match strengths with RAST results, use a dilution weaker by one than is indicated by the RAST score (the RAST minus one level), so that a RAST I level would be treated as a #2 (1:500) level.
Remember that in making vials, a level stronger than concentrate cannot be used. So, for either a #2 or #1 end point, the vial would be made from concentrate.
Each antigen is prepared from a stock vial 25 times more concentrated than the desired eventual strength, so to make a 5-mL vial (10 doses of 0.5 mL each) would require 0.2 mL (5 mL ÷ 25) of each antigen. Using the example just given.
Timothy grass 0.2 mL of #2
Ragweed 0.2 mL of #l
Oak tree 0.2 mL of concentrate (1:20)
Dust mite 0.2 mL of concentrate (30,000 AU/mL)
Total volume of extract 0.8 mL
Diluent to be added 4.2 mL
Total vial size 5.0 mL (10 doses of 0.5 mL)
If this vial were to be used for treatment only, not for testing, we would try to prepare it in such a way as to contain 10% glycerine. Looking at the previous calculations.
Timothy grass 0.2 mL of #2
Ragweed 0.2 mL of #1
Oak tree 0.2 mL of concentrate in 50% glycerine
Dust mite 0.2 mL of concentrate in 50% glycerine
Total volume of extract 0.8 mL of which 0.4 mL is 50% glycerine
To make the total vial contain 10% glycerine would require that 10% of the vial size (10% of 5 mL = 1 mL) be glycerine. So, 0.6 mL of 50% glycerine is added.
Regular diluent is added to bring the total to 5 mL.
Total volume 5.0 mL (10 doses of 0.5 mL, which will maintain potency for 3 months).
If the vial contains less than 10% glycerine, it must be remade in 6 weeks (if kept refrigerated when not in use). If it contains 10% glycerine, it will retain its potency for 3 months. If it contains 25% glycerine, it wilf retain its potency for 6 months. If it contains 50% glycerine (as is the case with stock antigens), its potency will be retained for 2 to 3 years.
After the treatment vial is made, a typical dosing regimen might be as follows: 0,05, 0.10, 0.15, 0.20, 0.25, 0.30, 0.35, 0.40, 0.45, and 0.50 mL. You will note from this that if the injections are given weekly, the vial will expire before 10 doses can be given, unless glycerine is added to bring the concentration to 10%, as already noted.



