QUESTIONS
1 Which statement about the orbital septum is false?
A) During entropion repair, it is very important to recognize the orbital septum of the lower eyelid as being different from the aponeurosis or lower eyelid retractors.
B) The orbital septum arises from a condensation of the periosteum of the orbital rim called the arcus marginalis.
C) The orbital septum inserts on the superior border of the tarsus in the upper eyelid.
D) The orbital septum serves as a barrier to the spread of infection from the superficial eyelids to the orbital tissues.
2 Which statement concerning the medial canthal area is true?
A) All of the attachments anchoring the tarsi to the medial orbital wall lie anterior to the lacrimal sac and attach to the maxillary portion of the frontal bone.
B) The lacrimal sac lies posterior to the orbital septum.
C) The muscle pump of the lacrimal pump mechanism is innervated by the fifth cranial nerve.
D) Lockwood ligament attaches posterior to the lacrimal sac.
3 Which statement regarding fat encountered during eyelid surgery is false?
A) Preaponeurotic fat is orbital fat.
B) Extraconal orbital fat is an important landmark in identifying the levator aponeurosis.
C) The removal of fat from the upper eyelid nasal, central, and lateral fat pads may be done with impunity.
D) In the upper eyelid, the nasal fat pad is small, whereas the lateral fat pad is the small fat pad in the lower eyelid.
4 Which statement regarding Whitnall ligament (superior transverse ligament) is false?
A) Whitnall ligament attaches medially to the trochlea, laterally to the capsule of the lacrimal gland, and to the lateral orbital wall.
B) This ligament is a condensation of the sheath of the levator muscle and serves as a check ligament to prevent excessive elevation of the eyelid.
C) Whitnall ligament acts to change the direction of pull of the levator muscle from horizontal to vertical.
D) This ligament passes anterior to the lacrimal gland.
5 Which statement about eyelid anatomy is false?
A) The gray line is formed by the muscle of Riolan and represents the observable edge of the pretarsal orbicularis at the eyelid margin.
B) The posterior lamella of the eyelid consists of the conjunctiva and tarsus.
C) The mucocutaneous junction occurs where the eyelashes emerge from the eyelid.
D) The peripheral and marginal arterial arcades allow for anastomosis between the internal and external carotid systems.
6 Features of the orbicularis muscle include:
A) closure of the eyelid, depression of the eyebrow, and facilitation of tear drainage.
B) pretarsal orbicularis inserts temporally to become the lateral canthal tendon, contraction narrows the palpebral fissure, and the orbital portion of the muscle inserts medially on the posterior lacrimal crest.
C) the deep head of the medial pretarsal muscle is called Horner tensor tarsi and innervation of the orbicularis muscle by cranial nerve III is divided into three segments (pretarsal, preseptal, and orbital).
D) the zygomaticofacial nerve innervates the upper lid orbicularis, the frontal branch of cranial nerve VII sends motor fibers to the upper lid orbicularis, and the preseptal orbicularis divides to encompass the lacrimal gland.
7 Which one of the following muscle groups is paired incorrectly?
A) Tensor tarsi muscle—deep head of the pretarsal orbicularis
B) Nasalis—preseptal orbicularis
C) Superciliary corrugator muscle—orbital orbicularis
D) Frontalis—procerus muscle
8 Which structure and its bony framework are paired incorrectly?
A) Lacrimal sac fossa—lacrimal and maxillary bones
B) Optic canal—greater and lesser wings of the sphenoid bone
C) Inferior orbital fissure—maxilla, zygomatic bone, palatine bone, and greater wing of the sphenoid bone
D) Anterior and posterior ethmoidal foramen—ethmoid and frontal bones
9 The carbon dioxide laser has all of the following characteristics except:
A) wavelength in the infrared spectrum
B) able to be seen by the human eye
C) utilized for orbital tumor excision
D) operates at 10.6 µm
10 The site of action of botulinum toxin type A (Botox), when used to treat facial movement disorders, is the:
A) motor nerve terminal, inhibiting acetylcholine release
B) motor nerve terminal, promoting cholinesterase release
C) plasma membrane (sarcolemma) of the striated muscle, inhibiting acetylcholine release
D) plasma membrane (sarcolemma) of the striated muscle, promoting cholinesterase release
11 Which one of the following is not a feature of basal cell carcinoma?
A) Pearly elevated margins
B) Likely spread to regional lymph nodes
C) Ulcerated epithelium
D) Telangiectatic vessels
12 The following factors are all associated with cutaneous cancers except:
A) increased sun exposure
B) increased age
C) red hair
D) increased natural skin pigmentation
13 Features most consistent with a malignant eyelid lesion include:
A) tenderness, erythema, alteration in pigment pattern
B) disruption of tarsal architecture, raised pearly margins, pruritus
C) lash loss, central ulceration, rapid growth
D) ipsilateral lymph node metastasis, hyperkeratosis, dark pigmentation
14 A 40-year-old, red-haired, blue-eyed man of Irish descent living in Tucson, Arizona, presents with a raised firm nodule with telangiectasia on his lower eyelid. This lesion most likely represents:
A) nodular basal cell carcinoma
B) morpheaform basal cell carcinoma
C) squamous cell carcinoma
D) sebaceous adenocarcinoma
15 Features of a keratoacanthoma include all of the following except:
A) spontaneous resolution
B) loss of eyelashes
C) ulcerated crater filled with lipids
D) rapid growth
16 The 5-mm raised skin lesion with central ulceration is least likely to be which of the following?
A) Keratoacanthoma
B) Squamous cell carcinoma
C) Basal cell carcinoma
D) Malignant melanoma
17 The CT examination in Figure 6-1 is from a 55-year-old man. Which one of the following is least likely in the differential diagnosis?
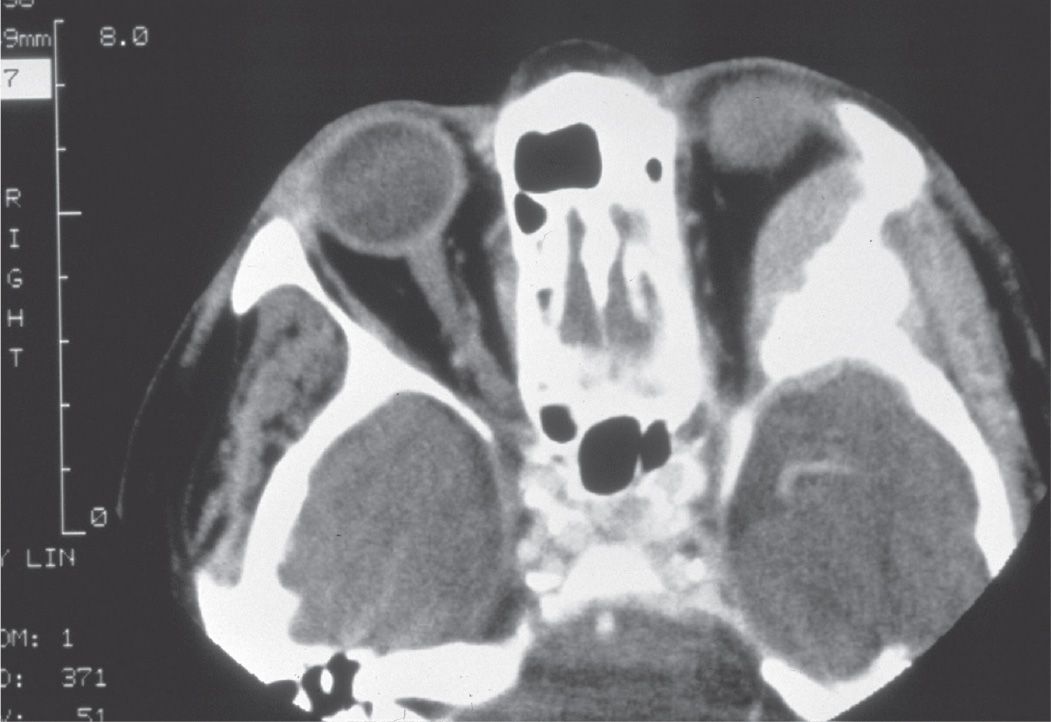
A) Metastatic prostate carcinoma
B) Sphenoid wing meningioma
C) Fibrous dysplasia
D) Metastatic melanoma
QUESTIONS 18 and 19 The defect of this eyelid (Fig. 6-2) of a 65-year-old woman resulted after a Mohs surgical procedure.
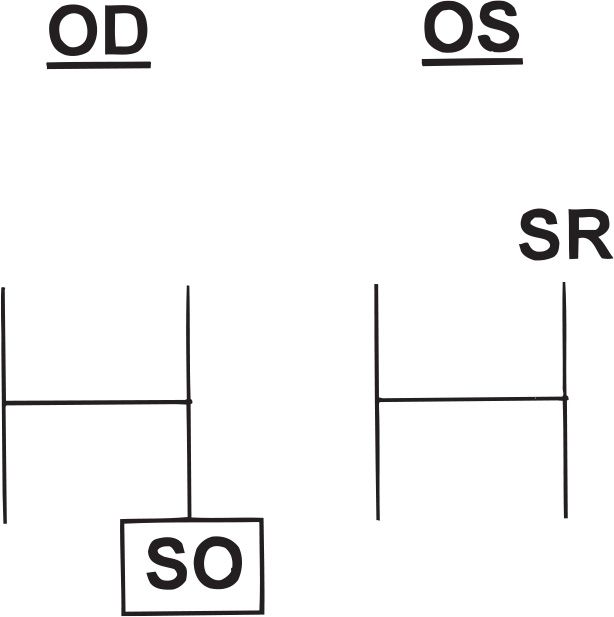
18 What surgical method would be the most appropriate for reconstruction of the posterior lamella?
A) Cutler–Beard flap
B) Bipedicle myocutaneous flap
C) Full-thickness skin graft
D) Hughes tarsoconjunctival flap
19 What is the least likely cause that led to the eyelid defect pictured in Figure 6-2?
A) Basal cell carcinoma
B) Metastatic cancer
C) Sebaceous cell carcinoma
D) Squamous cell carcinoma
20 All of the following statements concerning lymphatic and venous drainage are true except:
A) Lymphatic vessels of the orbit drain along the lateral portion of the cavernous sinus.
B) Lymphatic vessels serving the medial portion of the upper eyelid drain into submandibular lymph nodes.
C) Lymphatic vessels serving the lateral portions of the upper eyelid drain into preauricular nodes.
D) Pretarsal venous drainage of the medial upper eyelid is into the angular vein and the lateral venous drainage is into the superficial temporal vein system.
21 Xanthelasma eyelid lesions have all the following features except:
A) associated with systemic hyperlipidemic conditions in approximately 25% of patients
B) located in the basal epithelial layer of the skin
C) associated with the Erdheim–Chester disease
D) microscopically contain foamy histiocytes
22 Which of the following glands are matched with their correct types of secretions?
A) Moll—apocrine, main lacrimal gland—eccrine, meibomian glands—apocrine
B) Glands of Krause—holocrine, gland of Zeis—apocrine, goblet cells—holocrine
C) Glands of Wolfring—eccrine, gland of Moll—apocrine, goblet cells—holocrine
D) Main lacrimal gland—eccrine, meibomian glands—holocrine, gland of Zeis—apocrine
23 Which gland does not contribute to the aqueous layer of the tear film?
A) Krause
B) Main lacrimal
C) Zeis
D) Wolfring
24 Which statement about eyelid abnormalities is false?
A) Congenital coloboma of the eyelid always involves the lower eyelid and can vary from a small notch to a complete absence of the eyelid.
B) Cryptophthalmos is a rare condition that is caused by a lack of differentiation of eyelid structures and is characterized by absence of a palpebral fissure with uninterrupted skin from the forehead over the eye to the skin of the cheek.
C) Ankyloblepharon filiforme adnatum is a form of ankyloblepharon in which the eyelid margins are connected by thin strands of tissue.
D) Distichiasis is a condition in which an accessory row of eyelashes grows from or are posterior to the meibomian orifices.
25 A patient calls to report pain, sudden swelling, and decreased vision the night after a blepharoplasty procedure. What should be done?
A) Advise the patient to use ice packs to decrease the swelling.
B) Set up an appointment for the patient to see you the next day.
C) Make arrangements to see the patient as soon as possible.
D) Reassure the patient that discomfort, swelling, and blurry vision are normal postoperative findings.
26 Which one of the following is found in the blepharophimosis syndrome?
A) Euryblepharon
B) Ankyloblepharon
C) Epiblepharon
D) Telecanthus
27 A 10-year-old girl has bulging and blepharoptosis of both upper eyelids and repeated episodes of eyelid inflammation and swelling. What is the most likely diagnosis?
A) Blepharochalasis
B) Dermatochalasis
C) Steatoblepharon
D) Blepharospasm
28 The best choice below for surgical repair of a ptotic upper eyelid exhibiting a high eyelid crease, a margin to reflex distance (MRD) of 0 mm, and excellent levator function would be:
A) resection of the superior tarsal muscle
B) unilateral frontalis suspension using autogenous fascia lata
C) reattachment of the dehisced levator aponeurosis
D) plication of the levator muscle (16 mm)
29 The most common form of blepharoptosis is:
A) involutional blepharoptosis (aponeurotic ptosis)
B) neurogenic blepharoptosis
C) myogenic blepharoptosis
D) mechanical blepharoptosis
30 In myogenic congenital ptosis, the levator complex (in the ptotic eye) is:
A) disinserted from the tarsus
B) histologically different from normal levator complex with decreased muscle fibers and fatty infiltrates
C) innervated by cranial nerve VII
D) absent below Whitnall ligament
31 In patients with ptosis, the 2.5% phenylephrine hydrochloride test:
A) may activate the sympathetic receptors in Müller muscle, resulting in elevation of the lid
B) can be used to assess the approximate elevation of the lid with external levator advancement
C) dilates the pupil so that the contralateral eyelid may drop
D) does not affect blood pressure through systemic absorption of the phenylephrine
32 Which one of the following statements regarding blepharoplasty is false?
A) Repair of lower eyelid dermatochalasis and/or steatoblepharon may be followed by lower eyelid retraction.
B) A retroblepharoplasty (transconjunctival blepharoplasty) is a procedure primarily used to perform upper eyelid surgery when trying to avoid an anterior incision.
C) The advantage of eyelid crease fixation in conjunction with blepharoplasty is that it aligns the eyelid crease and the postoperative scar.
D) Damage to the inferior oblique muscle is a potential complication of both anterior and posterior approaches to lower eyelid blepharoplasty.
33 Materials used for frontalis suspension of the eyelid include all of the following except:
A) silicone
B) fascia lata
C) nylon (e.g., Supramid)
D) polyglactin 910 (e.g., Vicryl)
34 All of the following statements are true in describing the lacrimal gland except:
A) The lateral horn of the levator separates the orbital and palpebral lobes.
B) The orbital and palpebral lobes have separate excretory glands that empty into the conjunctival fornix approximately 5 mm above the superior margin of the tarsus.
C) The lacrimal glands are exocrine glands.
D) Blood supply is provided by the lacrimal artery, a branch of the ophthalmic artery.
35 The osteotomy site fashioned at the time of a dacryocystorhinostomy (DCR):
A) is adjacent to the valve of Hasner
B) enlarges the opening of the common duct
C) is adjacent to the superior turbinate
D) is within 10 mm of the cribriform plate
36 What is the most common reason for failure of a DCR?
A) Obstruction at the level of the common canaliculus or bony ostomy site
B) Unsuspected lacrimal sac tumor
C) Recurrent infection of the lacrimal sac
D) Dacryoliths (lacrimal stones)
37 The Jones I test (primary dye test):
A) accurately defines the location of a nasolacrimal system obstruction
B) involves irrigating the lacrimal sac with fluid
C) has a high false-negative rate
D) is a reliable indicator of nasolacrimal duct obstruction
38 What is the most frequently seen primary malignant tumor of the lacrimal sac?
A) Fibrous histiocytoma
B) Hemangiopericytoma
C) Squamous cell carcinoma
D) Lymphoma
39 Which one of the following is an indication for probing of the nasolacrimal system?
A) Acute episode of acquired dacryocystitis
B) Intermittent acquired inflammatory nasolacrimal system obstruction
C) Congenital nasolacrimal duct obstruction unresponsive to massage
D) Workup of all patients with epiphora
40 Adult patients presenting with epiphora with a complete obstruction at the sac–duct junction would be expected to have:
A) negative dye disappearance test/positive Jones III
B) positive dye disappearance test/positive Jones I
C) positive dye disappearance test/negative Jones I
D) negative dye disappearance test/negative Jones II
41 Which one of the following statements regarding dacryocystograms is true?
A) They are a required part of the workup in acquired nasolacrimal system obstruction.
B) They are an excellent test for nasolacrimal function.
C) They demonstrate canaliculi well.
D) They demonstrate the nasolacrimal sac well.
42 All of the following statements regarding tumors of the nasolacrimal sac are true except:
A) They may produce painless irreducible swelling of the lacrimal sac.
B) They may produce bleeding on attempted probing.
C) They do not usually produce secondary dacryocystitis.
D) They may produce epiphora.
43 In regard to canalicular trauma, all of the following are true except:
A) One may wait 24 to 48 hours after injury to allow soft-tissue swelling to decrease.
B) Upper canalicular trauma alone should never be surgically repaired so as not to risk damage to the remaining nasolacrimal system.
C) Silicone stents should be left in place for 3 to 6 months.
D) Surgical microanastomosis of the cut canalicular ends with silicone stent intubation offers the best possibility of successful repair.
44 Regarding the canalicular system, which statement is false?
A) The ampulla has the largest diameter of the canalicular system.
B) A common canaliculus is present in approximately 30% of the population.
C) The canaliculus has a diameter of approximately 1.0 mm.
D) The average distance from the punctum to the nasolacrimal sac is approximately 10 mm.
45 Regarding irrigation of lacrimal outflow system, which statement is false?
A) Syringing saline into the lower canaliculus that irrigates into the nose indicates that no obstruction exists and that the system is functioning normally.
B) Irrigation of the upper punctum with regurgitation through the upper punctum suggests an upper canalicular obstruction.
C) Irrigation of the lower canaliculus into the sac with complete regurgitation through the upper punctum suggests obstruction of the nasolacrimal sac or duct.
D) It may be helpful to recover fluid from the nose to examine for casts.
46 Chronic use of the following medications has been reported to cause canalicular stenosis except:
A) echothiophate
B) idoxuridine
C) epinephrine
D) atropine
47 All of the following are indications for a conjunctivodacryocystorhinostomy or CDCR (Jones tube procedure) except:
A) lacrimal canaliculi have been destroyed.
B) canalicular remnants cannot be anastomosed with the intranasal cavity.
C) common canalicular obstruction combined with nasolacrimal duct obstruction.
D) paralytic or scarred eyelids with absent canalicular pumping mechanism.
48 In acute dacryocystitis:
A) topical antibiotics without systemic antibiotics should be prescribed.
B) cool compresses are applied to the medial canthus.
C) diagnostic probing may be therapeutic in adults.
D) most adults will need a DCR for correction of outflow obstruction.
QUESTIONS 49–52 A 12-year-old boy involved in a motor vehicle accident 3 months ago presents with a complaint of left-sided epiphora since the accident, along with a 1-week history of fever and progressive swelling, redness, and pain in the left medial canthal region with mucopurulent discharge from the medial canthus (Fig. 6-3).

49 Appropriate initial workup of this patient includes all of the following except:
A) a complete ophthalmic exam
B) CT scan of the orbits and sinuses
C) probing and irrigation of the left nasolacrimal system
D) culture and Gram stain of the medial canthal discharge
50 Appropriate initial therapy of this patient would include all of the following except:
A) DCR
B) IV antibiotics
C) topical antibiotic drops
D) incision and drainage of any pointing abscess
51 In acquired nasolacrimal system obstruction, where is the blockage most frequently located?
A) Canaliculi
B) Nasolacrimal sac
C) Nasolacrimal duct
D) Inferior turbinate
52 What is the most common bacterial etiology in acute dacryocystitis?
A) Actinomyces israelii
B) Pseudomonas aeruginosa
C) Streptococcus pneumoniae
D) Staphylococcal species
QUESTIONS 53–55 A mother brings her 12-month-old child to you because of chronic right-sided epiphora. She has been massaging the right nasolacrimal sac for the past 6 months; however, the epiphora has persisted (Fig. 6-4).
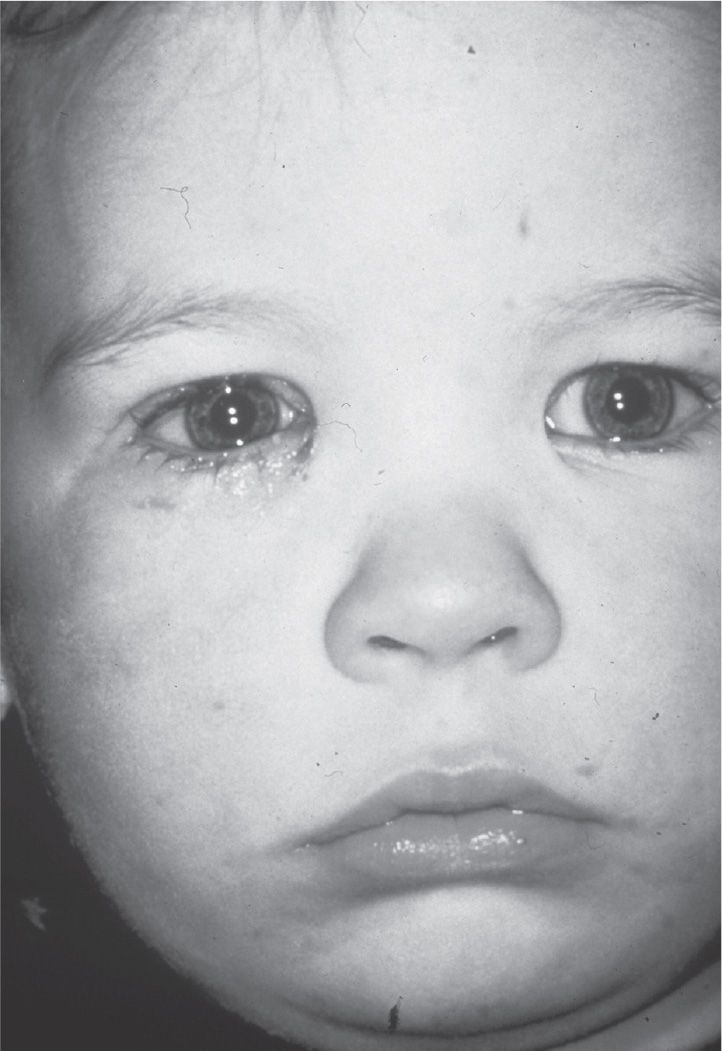
53 In congenital nasolacrimal system obstruction, where is the level of the obstruction?
A) Common canaliculus
B) Lacrimal sac
C) Valve of Rosenmüller
D) Valve of Hasner
54 The next therapeutic recommendation would include:
A) continuing massage
B) nasolacrimal system probing
C) DCR
D) observation, as most congenital obstructions resolve without therapy
55 Silicone stent intubation (with possible inferior turbinate infracture) is indicated in this patient when:
A) massage therapy has proven unsuccessful.
B) dacryocystography (DCG) shows obstruction at the level of the nasolacrimal duct.
C) nasolacrimal system probing has proven unsuccessful.
D) the patient is older than 12 months.
QUESTIONS 56–58 The 60-year-old woman pictured in Figure 6-5 reports a 3-month history of intermittent tearing and mattering in her right medial canthus. Additionally, she has noted focal swelling and tenderness near her lid margins.
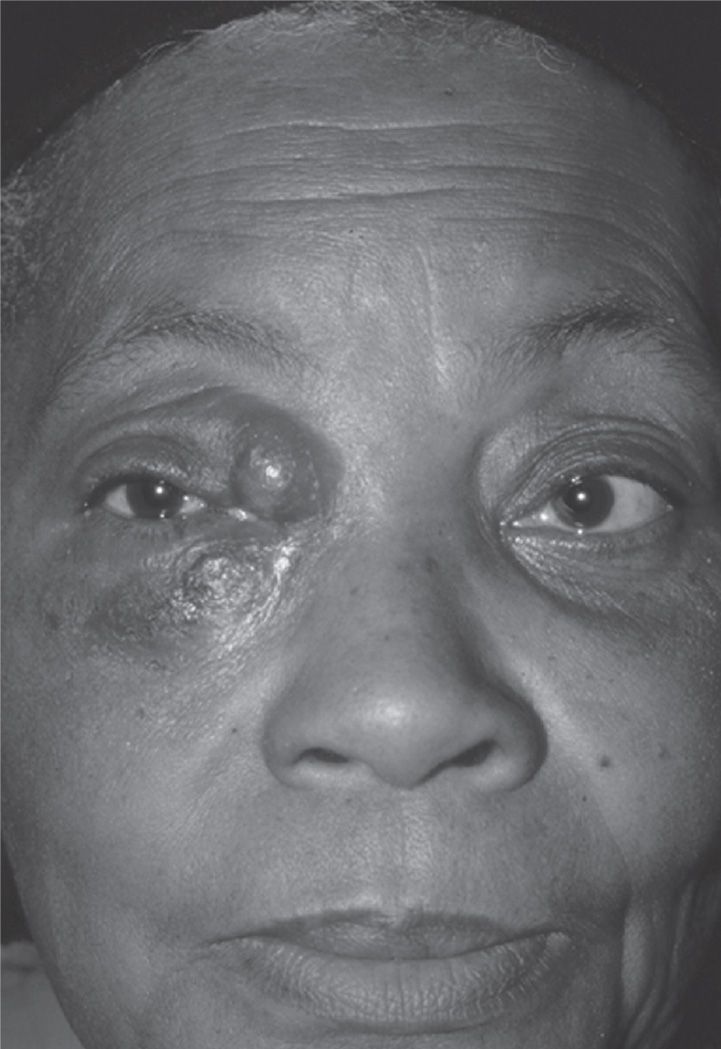
56 All of the following organisms are associated with canaliculitis except:
A) Actinomyces
B) Candida
C) Acanthamoeba
D) Streptomyces
57 Which one of the following suggests a diagnosis of canaliculitis?
A) Mucopurulent reflux from punctum with compression of the lacrimal sac
B) Gritty sensation on probing with yellow-tinged concretions
C) A palpable subcutaneous mass above the medial canthal tendon
D) Palpable masses in the lacrimal sac
58 Treatment of canaliculitis includes all of the following except:
A) canalicular curettage
B) canalicular incision and debridement
C) canalicular irrigation
D) DCR
59 Trachoma can cause all of the following changes except:
A) distichiasis
B) punctal stenosis
C) conjunctival scarring
D) entropion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


