FIGURE 6-1. Blepharophimosis. This child has classic changes of blepharophimosis with ptosis, telecanthus, and epicanthus inversus. This must be differentiated from simple epicanthus (see Fig. 6-2).
EPICANTHUS
Epicanthus is a medial canthal fold that is usually caused by immature midfacial bones. The condition is usually bilateral and will resolve as the child’s face matures. Epicanthus is associated with certain eyelid syndromes.
Epidemiology and Etiology
• Age: Congenital
• Gender: Equal
• Etiology: Immature midfacial bones are considered to be the cause.
History
• Noted at birth
Examination
• There is an extra fold of skin and subcutaneous tissue medially involving the eyelids. This may make the child appear esotropic. Four types of epicanthus have been described:
• Epicanthus tarsalis: Fold is more prominent on the upper eyelid.
• Epicanthus inversus: Fold is more prominent on the lower eyelid.
• Epicanthus palpebralis: Fold is equally on the upper and lower eyelids (Fig. 6-2).
• Epicanthus superciliaris: Fold runs from the eyebrow region to the lacrimal sac.
Special Consideration
• Epicanthus tarsalis can be a normal variant of the Asian eyelid. Epicanthus inversus is part of blepharophimosis syndrome.
Differential Diagnosis
• Blepharophimosis
Treatment
• Most cases of epicanthus resolve with normal facial maturation, so any potential treatment should be delayed until the child is mature.
• The exception is epicanthus inversus, which rarely disappears with facial maturation.
• If surgical treatment is required, these cases respond well to a Y–V-plasty or Z-plasty.
Prognosis
• Excellent. Most cases resolve as the child grows.
• If surgery is required, the results are good.

FIGURE 6-2. Epicanthal folds. These folds can often be seen as an isolated finding in young children. Unless severe, these epicanthal folds will lessen and even disappear as the child’s face matures.
EPIBLEPHARON
Epiblepharon is override of the pretarsal muscle and skin, which causes the cilia to assume a vertical position although the eyelid margin is in a normal position. This disorder is usually asymptomatic with no corneal staining and requires no treatment.
Epidemiology and Etiology
• Age: Congenital
• Gender: Equal
• Etiology: Immature facial bones are felt to allow for this excess skin and muscle.
History
• There are usually no symptoms.
Examination
• There is an excess of skin overriding the eyelid margin, which may even come in contact with the eye. If this skin can be pulled back, the eyelid margin under it is in a normal position.
• There is rarely any corneal staining.
• If there are corneal changes, consideration must be given to surgical correction (Fig. 6-3).
Special Considerations
• It is often very difficult to differentiate epiblepharon from congenital entropion, especially in an awake child who is squeezing his or her eyes shut.
• If there are significant corneal changes, then it is likely the eyelid is entropic and surgery is required.
Differential Diagnosis
• Congenital entropion
Treatment
• No treatment is needed in most cases.
• If there are corneal changes, then excision of the excess skin and muscle is the treatment of choice.
Prognosis
• Excellent. Most cases resolve as the facial bones mature. The rare case that requires surgery will respond well.
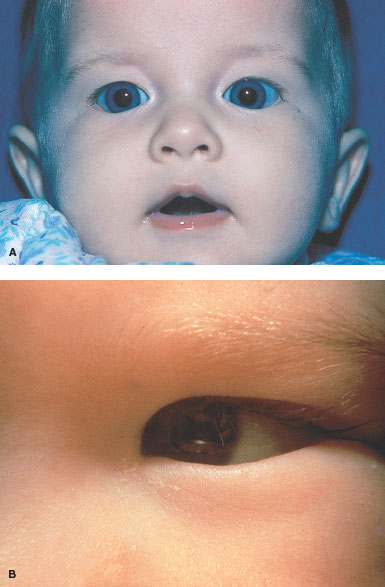
FIGURE 6-3. Epiblepharon (A&B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


