FIGURE 58.1A: Opening the eyes did not change the image, so the baby kept the eyes shut. B: After the operation of the right eye, she received near correction glasses and learned to use vision. C: She caught up with the delay in motor development and has developed normally despite her severe loss of vision. (Reprinted with permission from Hyvärinen L, Jacob N. What and how does this child see? Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013.)
In general, pediatric surgical services and active (re)habilitation start before and continue immediately after surgical interventions. Growth and developmental issues are central in the total care and immediate early intervention before and after surgery, including ophthalmic surgery. Anticipated functional vision should be discussed with the family before surgery, especially whether surgery is likely to prevent further vision loss, improve vision, or just save the eyeball. If the parents are given false hopes of the infant/ child becoming sighted after surgery alone and do not understand the importance of visual (re)habilitation and the special care of severely visually impaired infant/child, they may neglect to provide for their child’s functional needs and leave it all to the therapists. Disappointment after surgery or a visit to the hospital may prevent the parents’ motivation and cooperation for months.
The number of infants with brain damage and other conditions with several functional losses is increasing in all Western countries and the developing world. This makes the diagnostic investigations long and exhausting for the parents who “learn every day—often from a new person—that their infant has another abnormal structure or function.” Ideally, all information should be communicated to the parents by one person who knows the complexity of the situation and has the authority to arrange an early intervention professional to have time for the family in crisis. The stress that the infant undergoes during the often painful examinations and treatments may be detrimental to the developing infant’s brain. To counteract the stress, parents should be able to hold the infant close in quiet and comfort and offered a protected place in which breast-feeding is not disrupted. Many hospitals have good routine care for the delivery of “bad news.” The advice on all the aspects of care of the infant and the family during the diagnostic period should be collected into a manual for training of personnel. This would lead to a better standard of care of patients and parents everywhere.
The phrase “developmental emergency” was first used by Patricia Sonksen et al. (4) to describe the need of immediate care of an infant and the family, if diagnosis of impaired vision is made during the 1st year of life. The emotional stress may lead to depression in the mother or father; therefore, the families of disabled children should be considered as patients during and after the diagnostic period and treatments and supported in the demanding care of their infants.
EARLY INTERVENTION AT THE LOCAL LEVEL
Early intervention services at the local level vary from adequate to none. Visual impairment is still believed to be so rare that the infant’s pediatrician may have never before created a local team for early intervention that provides for the needs of the infant/child, parents, and siblings. Such a team is needed. Often, contact with other families with a similar experience, peer support, would help to decrease anxiety related to the child’s future. To promote this, contact with the local or national organizations of the blind should also be arranged so that families can learn about other families with visually impaired infants and children and how to contact them.
There is such a great variation in the organization of early intervention, rehabilitation, and special education of children with impaired vision in different countries and even in the different states in countries like the United States and Germany that generalizations are not possible. In countries and states where awareness of the importance of vision in early development and the role that impaired vision plays in learning prevails, it has led to added information on vision in the training of therapists and teachers, early referral by pediatric neurologists to ophthalmologists, and there are even ophthalmologists in the pediatric early intervention teams of hospitals. Increasing teaching about vision and visual functioning in all pediatric medical training programs and training of teachers, optometrists, and psychologists have been effective ways of improving the quality of services without increasing the need for care providers.
Passive “vision stimulation” is used in many local services. It should be used only initially when working with an infant who has so little vision that he or she is unaware of its presence. Even in that early phase, activities should be multimodal and include motor functions of the hands so that the visual experience is more concrete and supports learning (Fig. 58.2). Videos like “Leo learns by doing” (5) (Good-Lite), which depicts family activities that had led to normal motor and cognitive development of Leo, an infant with septooptic dysplasia and only light perception, can be instrumental in training early intervention workers and families alike in all cultures and should be easily available to all young parents.

FIGURE 58.2 Training the infant’s therapist to include activation of vision in Bobath therapy. An accompanying video can be found at the Web site (see Ref. 12). (Reprinted with permission from Hyvärinen L, Jacob N. What and how does this child see? Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013.)
Early intervention should consider all developmental areas in each case and find an answer to the basic question: “How much and what kind of vision is present for different functions and for the development of each particular function?” “For which functions should the infant/child be taught to learn strategies of exploration typical to blind children?”
Training of vision-related brain functions can start during the first assessment, which also serves as an introduction for the local therapist into work with visually impaired infants. The local therapist has usually met the infant at home before the first assessment of visual functioning (Fig. 58.2) and introduced himself or herself to start the assessment. If an infant has been in hospital for a long time and experienced that a “new voice” means “a new type of pain,” using the local therapist in the beginning of the assessment makes the situation easier for the infant. If the infant is relaxed and expects a pleasant play situation, several functions may be assessed at their best level. The test situation is also a smooth introduction of a child’s vision into the therapist’s usual neurodevelopmental therapy.
Visual field can be measured using an illuminated ball, that is, a penlight illuminating a small plastic ball with uneven surface (a toy for kittens with a bell in it). If the infant responds only in the midline, the use of the visual field can be activated by helping the infant to see his or her hands as shadows against the illuminated ball. Information about the form and surface of the ball combined with the movements of the hand and arm may help the infant to watch his or her hand for the first time. The better functioning hand is used first; then the hemiplegic arm and hand are supported to a position where the infant can see the fingers against the light.
Vision loss affects nearly all areas of development. The most important areas of functioning in which vision plays a central role are
• Communication and interaction
• Motor functions and balance
• Body awareness, visual spatial concepts, and orientation in space
• Auditory spatial concepts, typically built within the normal visual space
• Object permanence
• Language
• Incidental learning
• Social skills
Many of the functional areas mentioned above are included in the usual therapies for infants. Development of visual functions and their use in all areas of functioning can and should become an integral part of therapies and enrich the therapist’s work. Therapists need vision for communication with the infant and are highly motivated to learn about the infant’s visual functioning in detail. They also have the opportunity to observe the development of the infant two to three times a week and can teach the parents to use the training activities several times each day.
Communication and interaction are the first activities on the list, because they are the most important functions for the emotional development of the infant and parents and the bonding between them. Tactile and haptic exploration of parent’s faces is started early, especially if there is suspicion that hearing might also be affected.
Tadoma, the technique of speech reading by feeling the mouth, facial muscles, and the vibration of the vocal cords with an adult’s hand, is modified for the little hands to feel the movements of the mouth and the vibration of the vocal cords in turn (Fig. 58.3A).

FIGURE 58.3 A: Training of Baby Tadoma. Hearing was impaired in this boy with microphthalmia and colobomas of both eyes. B: In Bobath therapy he was guided to explore his body, which supported the development of normal spatial concepts and motor functions. C: The more microphthalmic and less functioning myopic eye was trained during therapy, and when parents read books to the boy, built with blocks, or later explored miniature animals and houses, his visual acuity in the poorer right eye remained low but would be of some help if something happened to the left eye. An accompanying video can be found at the Web site (see Ref. 12). (Reprinted with permission from Hyvärinen L, Jacob N. What and how does this child see? Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013.)
We do not assess visual communication of visually impaired young children in detail and are usually unaware of a child’s poor motion perception. Due to poor motion perception, the lips appear blurred. During exploration of face in front of a magnifying mirror, a well-functioning 6-year-old child may ask, “Does the voice come through the mouth?” and when answered “Yes, why do you ask?” the answer was “I thought that it comes through the ears.” In this case, nobody had been aware of the girl’s poor perception of the fast lip movements. She experienced lip movements since her hand happened to be close to the lips when she said something. We use lipreading without thinking how complex visual information it requires. Lipreading should be carefully assessed at least in all infants and children with hearing loss.
Exploring the parents’, siblings’, and caregivers’ faces makes these important persons concrete and real. Father’s face is especially interesting if explored before he shaves in the morning, next when one-half of the face has been shaved, and a third time when the shaving is completed. This experience gives the infant much to ponder until the father comes home in the afternoon, again slightly different. Mother’s face should be explored as well although she never changes like the father.
We do not assess visual communication of visually impaired young children in detail and are usually unaware of a child’s poor motion perception. Due to poor motion perception, the lips appear blurred. During exploration of face in front of a magnifying mirror, a well-functioning 6-year-old child may ask, “Does the voice come through the mouth?” and when answered “Yes, why do you ask?” the answer was “I thought that it comes through the ears.” In this case, nobody had been aware of the girl’s poor perception of the fast lip movements. She experienced lip movements since her hand happened to be close to the lips when she said something. We use lipreading without thinking how complex visual information it requires. Lipreading should be carefully assessed at least in all infants and children with hearing loss.
Exploring the parents’, siblings’, and caregivers’ faces makes these important persons concrete and real. Father’s face is especially interesting if explored before he shaves in the morning, next when one-half of the face has been shaved, and a third time when the shaving is completed. This experience gives the infant much to ponder until the father comes home in the afternoon, again slightly different. Mother’s face should be explored as well although she never changes like the father.
Motor development and vision are closely related. When a normally sighted infant sees his or her hand and brings it to the mouth, the early asymmetrical tonic neck reflex is counteracted. If a visually impaired infant does not see his or her hands, there is no incentive to explore them with the mouth, and the early reflex pattern may remain. Therefore, playing with the infants’ hands, guiding them to meet in the midline, and bringing them into the mouth are important in play therapy.
Body awareness and the possibility of seeing and feeling one’s own body parts facilitate development of spatial concepts.
Spatial concepts are difficult to create if the visual image of the environment is unclear. These concepts can be trained early using playmats with different structure at the two ends (Fig. 58.4A). Small spaces are important for the development of visually impaired infants and children. A tiny prematurely born infant starts in a shoe box, moves to a boot box, and then to larger and larger brown boxes (Fig. 58.4B). Later, the boxes need to have a sturdy frame; otherwise the infant may push the box to lie on its side. The size of the “little room” should be chosen so that the infant can reach the walls without stretching his arms straight out because infants do not extend like that.
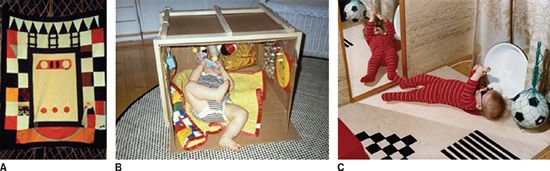
FIGURE 58.4 Examples of easy modifications of environment to support early development. A: Playmat with clearly different ends helps in development of concepts of directions. B: Brown box as a visual, auditory, and tactile space. Toys and objects hanging on the broad rubber band facilitate exploration and the development of object permanence. C: Training listening skills is important in infancy: the echoes of the infant’s voice from a metal washing basin on the right and the red plastic wastebasket on the left are different. Movements cause sounds that are amplified by the resonance board. (Reprinted with permission from Hyvärinen L, Jacob N. What and how does this child see? Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013.)
Large “little rooms” are constructed for blind school-age children with developmental delay. These “rooms” have a clear ceiling, whereas visually impaired infants and children with useful vision should have a nontranslucent ceiling and narrow slits up on the sides so that the space is a visual and auditory space. The walls should have visuotactile areas as landmarks for exploration. Toys and objects hanging from a thick rubber band do not disappear when the infant lets them go, which supports the development of object permanence.
A resonance board makes the infant aware of the movements of the feet even if they are difficult to see (Fig. 58.4C). In therapy the infant’s hands are helped to meet in the midline and, from there, to the mouth: this supports development of motor functions. Hands are also guided to feel feet and legs and together with them create a closed space around a big ball on the stomach, a closed space created with the infant’s own body. Notice that this infant with aniridia has dark glasses to prevent photophobia.
Carrying the baby in a sling gives experiences of movement patterns, creates opportunities for incidental learning, and increases communication between the adult and the infant. If the infant without motor problems is helped to become an active explorer and learner, early development may not notably differ from that of a sighted child. Exploration takes more time and requires thinking when vision does not give its usual firm framework for multisensory experiences. Numerous repetitions of movements are needed to learn and remember the tactilely and kinesthetically studied structure of objects, that is, movements of a door to learn how it sounds and mouthing of objects to explore details with the tip of the tongue and lips. Mouthing and repetitive movements can often be mistaken for autistic behavior in a visually impaired infant/child. Autistic children have similar repetitive movements and actions as visually impaired children. It is not known how often autistic children are visually impaired and have skillfully learned to use techniques that compensate for loss of visual information. We should carefully look for the difference between exploration and meaningless repetitive movements.
MOVING DIFFICULT TEST SITUATIONS TO KINDERGARTEN AND (SPECIAL) SCHOOL
Therapists and special education teachers are trained to pay attention to well-supported postures and facilitation of movements. As a part of their work, they can help in modifying the test situations for children so that these children can be assessed more completely.
Figure 58.5A shows a boy without good support and proper near correction unable to be tested. In Figure 58.5B, he reacts to the frame of the glasses because of hyper-sensitivity of the facial skin. This should not be interpreted as a sign that the child does not want to have glasses. In Figure 58.5C the boy watches the figure-in-motion Pepi test and apparently perceived the dog because his eyes made a quick saccade to the corner where the dog appeared and then followed the dog across the screen several times. This figure-in-motion test thus functions also as an opportunity to observe ocular motor functions.

FIGURE 58.5 A: This boy’s head fell to the side when he tried to bring it to the midline. B: Placing spectacles on a child’s face disturbs the child as long as the frame moves on the skin of the hypersensitive face. C: With proper head support and near correction, the child could participate in the tests. In this picture we see that the eyes have followed the figure-in-motion to the upper right corner. An accompanying video can be found at the Web site (see Ref. 12). The Pepi test is available for download at www.lea-test.fi/GAMES. (Reprinted with permission from Hyvärinen L, Jacob N. What and how does this child see? Assessment of visual functioning for development and learning, 2nd ed. Helsinki: VISTEST Ltd., 2013.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


