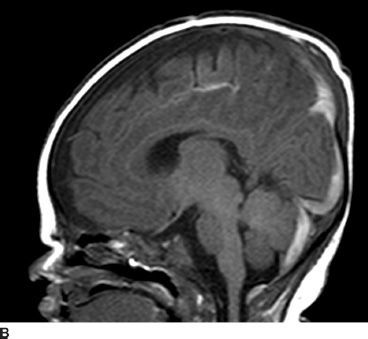

FIGURE 57.1 Baby girl, 1 month old. Nonaccidental head trauma. Diffuse subdural and subarachnoidal hematomas (arrows) located into the tentorium, the interhemispheric space, and over the left hemisphere (A,B). Parenchymal anoxic ischemic injuries in the left frontal and occipital lobes (C). (Courtesy of Pr C. Adamsbaum.)
The conjunction of hypoxia, venous congestion on immature vessels, intracranial hypertension, and general hypertension can explain the subdural and retinal hemorrhages.
SDH is reported to be a thin layer at the surface of the cortex probably secondary to ischemia or a thicker collection when bridging veins rupture (14,15).
Finite mathematical models of the eye and its motion show that shaking (at a rate of 4 cycles/seconds) applies a 50-fold increased force to the retina because of inertia and resonance compared to a single trauma from a 45-cm fall onto hard ground (15).
Diffusion-weighted MRI studies have confirmed the importance of ischemia in NAHI, evidenced by the extent of a hyperintense signal from brain hypoxia early in the evolution (16,17).
The eye examination has to be conducted as soon as possible by a trained ophthalmologist, using a speculum and topical anesthesia. Facial and lid bruises are carefully reported. Visual acuity assessment of the ability to fix and follow is determined. Anterior segment status is also recorded, and fundus examination is performed using indirect ophthalmoscopy with a 28- or 30-diopter lens following pupil dilation when possible. If available, a fundus wide-field photograph is taken by a RetCam, or a detailed drawing is performed after the examination is completed (Table 57.1).
TABLE 57.1
Main NAHI case studies
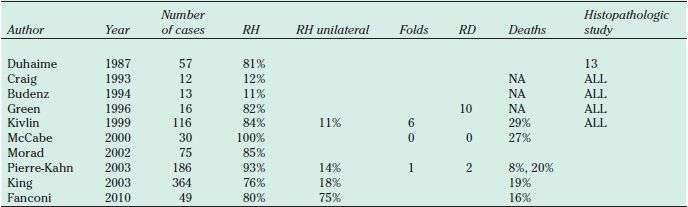
NAHI, nonaccidental head injury; RH, retinal hemorrhages; RD, retinal detachment.
Retinal Hemorrhages
Retinal hemorrhages are the most specific and common findings of NAHI. They are present in 70% to 93% of the cases (3–7,10,13). Unilateral retinal hemorrhages are reported in 12% to 40% of the cases (6,18).
Pierre-Kahn et al. (7) compiled a prospective case series from January 1996 to September 2001 on 241 consecutive infants hospitalized for an SDH. Children were divided into three categories based on the degree of certainty that they had been shaken: children presumed to have been shaken (group 1), children with signs of head trauma without a relevant history of accidental trauma (group 2), and children with proven severe accidental trauma (group 3). Intraocular hemorrhage was seen in 77.5% of children in group 1, 20% of children in group 2, and no children in group 3, leading the author to conclude that intraocular hemorrhages are suggestive of SBS.
Vinchon et al. (19) reported that 53% to 80% of children with NAHI had retinal hemorrhages, whereas only 0% to 10% of children following accidental trauma had retinal hemorrhages. The investigators conducted a prospective analysis of 150 cases of head trauma collected over 3 years and calculated a sensitivity of 75%, specificity of 93.2%, positive predictive value of 89.4%, and negative predictive value of 82.9% for retinal hemorrhage and child abuse.
Clinical Aspects of Retinal Hemorrhages
Histopathologic studies of postmortem eyes have shown that retinal hemorrhages in NAHI are diffuse and extend from the posterior pole to the far periphery (Fig. 57.2). They mainly involve the superficial layers, under the inner limiting membrane (30% to 38%), or the nerve fiber layer but have been reported to be intravitreal and retrohyaloidal (47%) (Fig. 57.3). More rarely, can the hemorrhage be intraretinal or subretinal (10%). In 15% of cases, hemorrhages present as Roth spots, with fibrin in the centers of the hemorrhages. Recent optical coherence tomography (OCT) studies have confirmed in vivo that pathologic findings are localized detachments of the posterior hyaloid at the posterior pole, double-layered epiretinal membranes, macular holes, retinal folds, and retinal schisis in the area of hyaloidal adherence, which exerts vitreous traction as part of the pathophysiology (20,21).

FIGURE 57.2 Two-month-old infant with NAHI: diffuse hemorrhages in all retinal fields and subhyaloidal posterior hematoma. Circular retinal fold around the posterior pole. (Courtesy of Pr Claude Speeg from Strasbourg.)
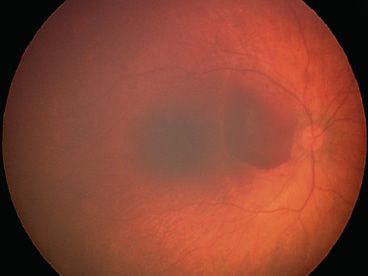
FIGURE 57.3 Mild form of NAHI with localized macular retrohaloidal hematoma.
Differential Diagnosis
Retinal hemorrhages are highly specific of NAHI. In 182 cases of children under 2 years of age, admitted for a first episode of seizures, Curcoy et al. (22) reported that only two had retinal hemorrhages. In accidental brain injury with direct brain trauma, the proportion of children presenting with retinal hemorrhages is <10% (13,16) and usually exists from very specific trauma with a predominant crush factor. Convulsions and vomiting are not recognized to induce retinal hemorrhages.
Other causes of retinal hemorrhages are rare and include coagulation deficiencies: homozygous protein C deficiency, Hermansky-Pudlak syndrome, vitamin K deficiency, glutaric aciduria type 1, and X-linked retinoschisis. Osteogenesis imperfecta with brain trauma and Terson syndrome are other rare causes of intraocular bleeding (23) (Table 57.2).
TABLE 57.2
Causes of retinal hemorrhages
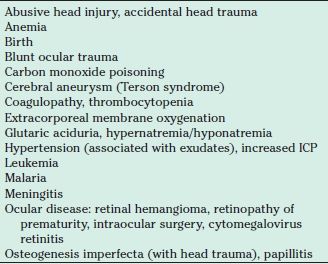
ICP, intracranial pressure.
Schisis
Retinoschisis due to NAHI has been described in severe cases and has been evidenced by OCT studies of affected babies (20,24). The features reported are multilayered retinoschisis affecting areas where the vitreous remains attached. Vitreous traction could explain the mechanism of these lesions.
Macular Changes
Besides epiretinal or subhyaloid hemorrhages, macular holes have been reported in rare cases and documented by OCT (20). Epiretinal membranes are a common finding in survivors of NAHI (25) and often present as a two-layered structure, corresponding to a proliferating structure and the internal limiting membrane.
Neovascularization and Retinal Ischemia
In 1999, Brown and Shami (26) reported the first case of optic disc neovascularization after NAHI, which developed 4 months after the shaking episode. Initially the 4-month-old baby had diffuse extensive retinal hemorrhages and intravitreal hemorrhage and, after 4 months, had documented florid optic disc neovascularization on angiography performed under anesthesia (26). We reported three cases of tractional retinal detachment due to extensive neovascular proliferation in infants having a history of NAHI (27) (Fig. 57.4). Wide-angle angiography performed in patients after NAHI has shown wide areas of peripheral retinal ischemia (28), raising the necessity of long-term follow-up and consideration of laser retinal ablation in these cases (Fig. 57.5). A shearing mechanism due to vitreous traction or secondary retinal ischemia due to hypoxia may explain these findings (24,29).
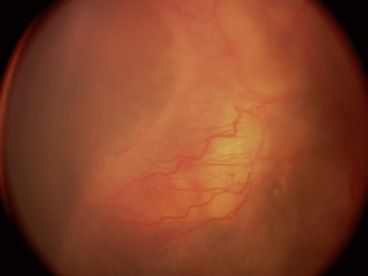
FIGURE 57.4 Total retinal detachment with diffuse neovascularization and ridge-like structure in the midperiphery, in a 7-month-old NAHI baby.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


