This chapter deals with all tissues of the injured eye, not only the retina: even if it is not initially apparent, the posterior segment is commonly injured; consequently, it is often the vitreoretinal surgeon who is the key person treating the child.
STANDARDIZED LANGUAGE OF OCULAR INJURIES: THE BIRMINGHAM EYE TRAUMA TERMINOLOGY
Birmingham Eye Trauma Terminology (BETT) (2) is used in this chapter as the language of eye injury terminology (Table 56.1). In BETT an unambiguous definition applies for each type of mechanical eye injury. Regardless of injury type, the tissue of reference is always the entire globe, obviating the need to specify the tissue involved. For example, in “corneal penetrating injury” “corneal” refers to the location of the wound, not to the type of trauma (Fig. 56.1).
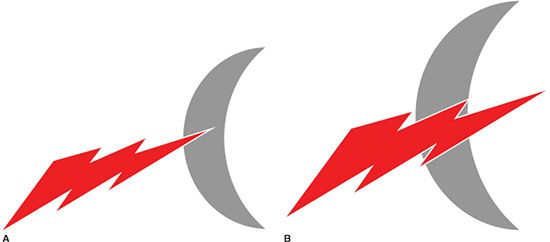
FIGURE 56.1 The tissue of reference, not just the term used, determines the injury type. A: The tissue of reference is the cornea. This is a penetration into the cornea but not into the inside of the eye; therefore, it is a closed globe injury. B: The tissue of reference is the globe. This is a penetration through the cornea and into the inside of the eye; therefore, it is an open globe injury.
TABLE 56.1
Definitions in the BETTa
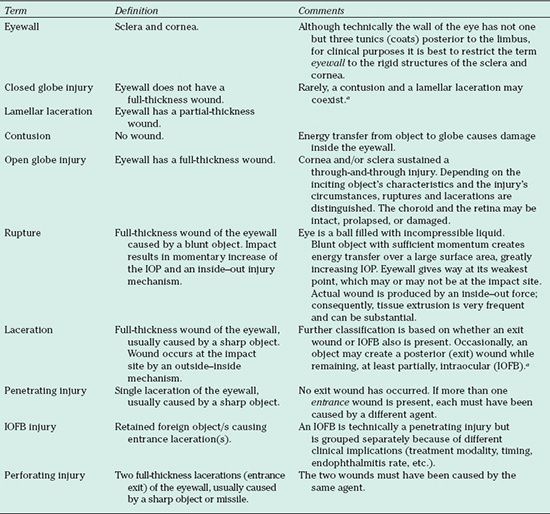
BETT, Birmingham Eye Trauma Terminology; IOFB, intraocular foreign body; IOP, intraocular pressure.
aRarely, the injury is so atypical that characterization is very difficult or it may be complex: an eye may have simultaneously sustained a perforating and IOFB injury. BETT does not incorporate eyes that have been totally destroyed, leaving enucleation as the only option. The clinician should use his or her best judgment, based on the information provided here.
The wall of the eye is defined as the sclera and/or cornea, regardless of whether there is choroidal or retinal involvement. There are two major injury categories, depending on whether a full-thickness wound of the eyewall is present: open globe injury or closed globe injury.
In the closed globe category, a lamellar (partial-thickness) laceration is distinguished from a contusion. A lamellar laceration does not violate the entire width of the tissue (Fig. 56.1A), whereas a contusion is caused by a blunt object that transfers its kinetic energy without the creation of a wound. Contusions are often, erroneously, described in the literature as “blunt trauma.” The error lies in the fact that a blunt trauma can result in not only a closed globe injury but also an open globe injury if the blunt force is great enough.
In the open globe category, ruptures and lacerations are differentiated. The underlying cause of a rupture is elevated intraocular pressure (IOP) via energy transfer from a blunt object. As opposed to a contusion, however, in this case the increased internal pressure exceeds the resistance of the eyewall and a wound occurs (inside–out mechanism). The wound forms where the eyewall is the weakest, which is rarely at the impact site; the object almost never enters the eye. Ruptures have the worst prognosis of all injury types, in part because there is so much tissue extrusion. Thus, it is important to distinguish ruptures from lacerations.
A laceration is caused by a sharp object. The wound always occurs at the impact site with the object entering the eye (outside–inside mechanism). The object can then exit via the same route, be retained, or exit at a site distant from the entry wound.
When a single wound is present, it is termed penetrating injury: the object exits through the entry wound. An intraocular foreign body (IOFB) injury is similar to a penetrating injury but is distinguished because of its special management and prognostic implications due to the presence of the retained foreign material. Finally, if the object exits the eye via a different wound, a perforating injury is encountered (“through-and-through injury”). An overview of BETT is provided in Figure 56.2.
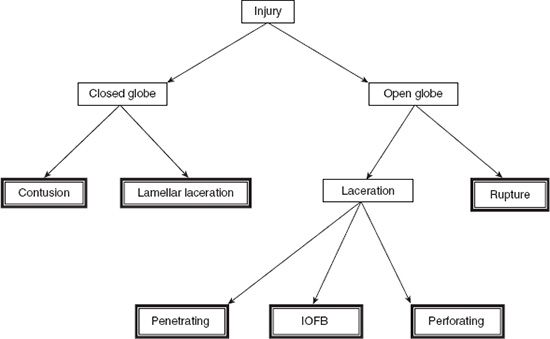
FIGURE 56.2 In the BETT system, the double-framed boxes show the diagnoses used in clinical practice.
To identify areas in which prevention can be effective, valid epidemiologic data are needed. Numerous epidemiologic studies of ocular trauma have been published (3–13), although comparative analysis is difficult, because there are differences in target population, definition of the pediatric age, the country or region surveyed, type of study (whether hospital or population based), and the method and length of surveillance. Relevant clinical information is discussed below regarding circumstances of injury, injury types, tissue involvement, and functional outcomes.
Brief Literature Review
Children suffer a disproportionate number of eye injuries, sustaining up to 52% of all ocular trauma (9). Injury is the leading cause of monocular blindness in children (14), and about a quarter of children seen at the emergency room present with severe trauma (15,16). In a population-based study from Maryland, the estimated incidence rate for those aged 0 to 15 years was 15.2 per 100,000 population-years (12). From Scotland, it was reported that 22% of those hospitalized for ocular trauma were under 15 years (5). Among assault-related open globe injury cases, 17% involved children (17). In Oman, the prevalence of traumatic monocular visual damage was 0.19% in a cohort of almost 700 children aged 6 to 12 years (18).
The risk of injury is greatest in children from poor socioeconomic populations, especially those younger than 5 years. The risk to child bystanders is also significant, with a victim rate of up to 44% in a study from Brazil (19).
Male preponderance is less pronounced in children than in adults, and the ratio increases with increasing age (12).
The home is the most common place for ocular trauma to occur in children or adults, reported in up to half of the cases in children (8).
Local factors greatly influence the causes of the injury. Most reports identify sports as the most common activity resulting in eye injury. Forty-one percent of all sports-related trauma occurred in children under 15 years of age (20) (Table 56.2). However, a Nigerian survey showed that 30% of injuries occurred during domestic activities, such as fetching firewood, gardening, and collecting seeds, and that “only” 24% occurred during play and sports (21). More than half of injuries were found to be agent-related in India (13), with bows and arrows as the most common cause and household appliances as the second (22). In one US study, 32% of injuries were shown to be agent related or caused directly by toys (7). In another US study, accidental blows and falls were responsible for 37% of injuries (12).
Air guns are a serious, preventable source of eye injuries. In one study from Kansas and Seattle (23), the average victim was 11 years old, and 51% were shot by a friend or sibling. A total of 71% of the shootings were unintentional, and 3% of the victims died. The consequences of air gun–related eye injury are severe: 32% lost an eye and 53% lost light perception (24). In the greater Ottawa area from 1974 to 1993, 60% of enucleations were performed for trauma among those under 18 years; of these, 25% were caused by air guns (25).
War games and paint ball injuries constitute a relatively new source of ocular trauma, especially if these sports are played in a nonorganized or unofficial capacity. In a review of 101 reported cases, only 12% of patients wore eye protection, and even this may have been inadequate, that is, goggles instead of face guards. The trauma often was severe. Only 43% of eyes had final visual acuity of 20/40 or greater (26).
Fireworks are another easily preventable source of pediatric eye injury (Fig. 56.3). In Sweden, 75% (27) and in Austria, 49% (24) of fireworks-related injuries affected those under 18 years with ocular involvement in up to 38% of the cases. While one-third of fireworks-related injuries are caused by illegal devices, the legal bottle rocket is the main culprit for causing eye trauma. They were responsible for 80% of the 185 fireworks injuries in the Eye Injury Registry of Alabama and affected bystanders in 67% of the cases (28).
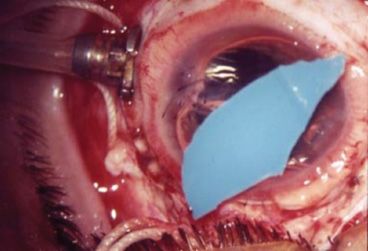
FIGURE 56.3 Large piece of plastic removed from an eye with a fireworks injury.
Motor vehicle crashes used to be responsible for around 10% of eye injuries in the pediatric population (12), but the rate is decreasing, mainly due to the enforcement of seat belt and child seat belt laws.
Serious assaults are an uncommon cause of eye trauma in children, although a review of those hospitalized for ocular trauma in Scotland (8) reported a rate of 14%.
Among open globe injuries, mostly sharp objects are the culprit: 67% in one study (29). In another report (30), the breakdown was darts 16%, glass 15%, and knives 14%. In a large city, guns were responsible for open globe injuries in 22%, sticks and tree branches 11%, and missiles 9% (31). While projectiles, sticks, and falls are common sources of eye trauma, reports of unusual causes also abound and include magpies, tarantula hairs, and bites by other spiders. Education regarding sharp toys and the dangers of explosion from glass bottles and caps is especially important in the pediatric age group.
Having an adult present is widely believed to reduce the injury risk; most injuries occur during unsupervised play.
The majority of reports found no difference in the laterality of eye involvement. However, among those injured by exploding glass bottles, the left eye was more likely to be involved, whereas among children with self-inficted injuries, the right eye was injured much more frequently (32).
Although children sustain the entire spectrum of ocular trauma seen in adult patients, burns are an uncommon cause of serious eye injury; in one study, only 4% of injuries occurred from chemical injuries (33). The outcome in most burn cases is good, with rare permanent effects.
Depending on the type of study, the proportion of open globe trauma among all eye injuries varies between 9% and 84% (3). In a study of those hospitalized for eye trauma in Scotland (8), 65% of the cases were contusions, 28% were open globe, and 4% had IOFBs. Penetrating trauma is more common than rupture (79% vs. 13%) (34).
Data from the United States Eye Injury Registry
The United States Eye Injury Registry (USEIR), the surveillance arm of the American Society of Ocular Trauma (ASOT), is the world’s largest database on serious eye injuries and is a model for affiliate registries operating under identical guidelines in many other countries. The USEIR collects and publishes information on all types of “ocular trauma that threatens permanent and significant structural or functional change to the eye/adnexa.” The USEIR encourages all ophthalmologists to report on the epidemiology and clinical characteristics of serious eye injuries via the Internet (useironline.org in the United States and weironline.org internationally). The epidemiologic and clinical analysis we performed for this chapter represents the largest dataset of pediatric injuries available in the literature. In addition to presenting information on the pediatric age group, we also provide data on adult patients (aged 19 and above, group AD) for comparison.
The pediatric patients (group CH) were divided into three age groups: 0 to 4 years (group A, n = 560 [13%]), 5 to 14 years (group B; n = 2, 485 [57%]), and 15 to 18 years (group C, n = 1,288 [30%]).
The male-to-female ratio was 4.5:1 in group AD and 3.4:1 in group CH, with the following breakdown: group A, 1.9:1; group B, 3.6:1; and group C, 4.1:1. These ratios confirm the trend reported in many publications that the male-to-female ratio increases with age.
In group AD, information on eyewear at the time of the incident was known in 6,076 of cases; of these, none was worn in 90%, prescription or sunglasses in 3%, and safety glasses in 3%. In group CH, information on eye-wear at the time of the incident was known in 3,175 of cases; of these, none was worn in 98%, prescription or sunglasses in 1%, and safety glasses in <1%. Children were less likely to wear eye protection than adults.
Injuries to bystanders are rarely reported in the literature, although commonly the bystanders are the victims. Fifteen percent of the 6,283 known cases in group AD and 37% of the 3,090 known cases in group CH were bystanders. The risk of sustaining a bystander injury is twice as high in children than in adults.
The place of injury varies with age (Table 56.3). In developed countries, the home is the most common place of injury. The younger the child, the greater is the risk of sustaining trauma in the home. The risk of sports-related injuries increases with increasing age of the child.
TABLE 56.3
Place of injury in a USEIR study of serious eye injuries
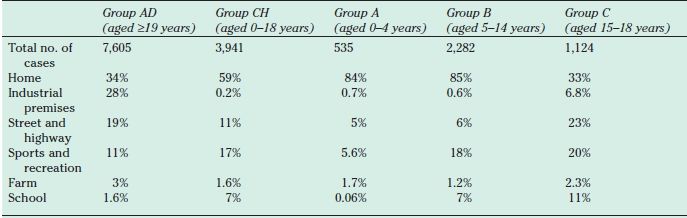
USEIR, United States Eye Injury Registry.
The older the child, the more similar are the causes of the injury to those seen in adults (Table 56.4).
TABLE 56.4
Cause of injury in a USEIR study of serious eye injuries
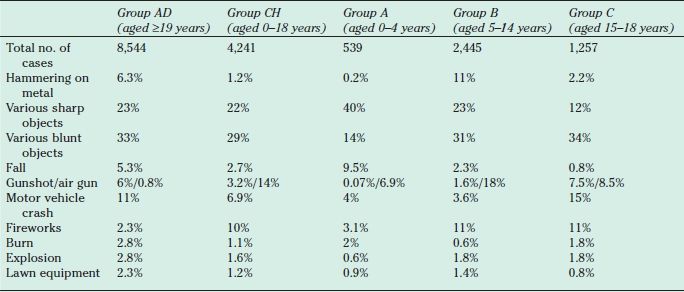
USEIR, United States Eye Injury Registry.
There is a consistent, yet unexplained, shift with age from right to left eye preponderance.
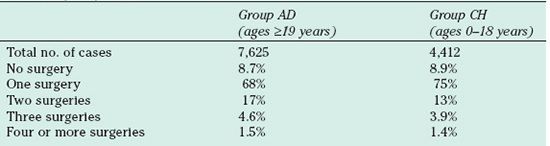
The posterior segment is involved in 44% in group AD and in 43% in group CH. Retinal detachment was found in 10% in group AD, 8% in group CH, 4.6% in group A, 7.8% in group B, and 10% in group C. Almost half of serious eye injuries involve the posterior segment, which is the primary factor determining the final outcome. The rate of retinal detachment increases with age. We found no difference in the number of surgeries performed on children versus adults (Table 56.5).
TABLE 56.5
Number or surgical procedures performed in a United States eye injury study of serious eye injuries
The initial visual acuities are given in Table 56.6. Final visual acuity, defined as at least 1 month postoperatively for this study, was available for 3,562 eyes in group AD and 1,750 eyes in group CH. The results are given in Table 56.7.
TABLE 56.6
Age-related initial visual acuity in a USEIR study of serious eye injuries
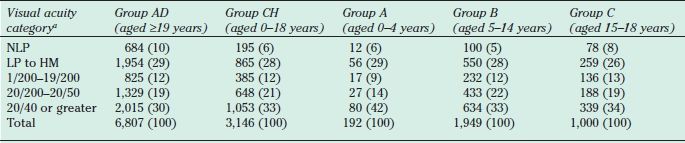
Values are given as number (percent). Percentages do not add up to 100 because of rounding.
aThe visual acuity categories are identical to those used in the development of the Ocular Trauma Score.
USEIR, United States Eye Injury Registry; HM, hand motion; LP, light perception; NLP, no light perception. (From Umeh R, Umeh O. Causes and visual outcome of childhood eye injuries in Nigeria. Eye 1997;11:489–495).
TABLE 56.7
Age-related visual outcomes in a USEIR study of serious eye injuries
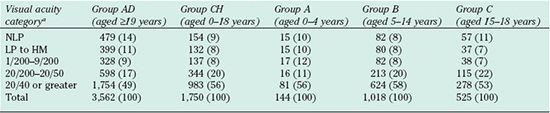
Values are given as number (percent). Percentages do not add up to 100 because of rounding.
aThe visual acuity categories are identical to those used in the Ocular Trauma Score. (Kuhn F, Maisiak R, Mann L, et al. The Ocular Trauma Score (OTS). Ophthalmol Clin North Am 2002;15:163–166).
USEIR, United States Eye Injury Registry; HM, hand motion; LP, light perception; NLP, no light perception.
General Ophthalmologic Examination
History taking is always an art, requiring expertise and patience; it is an especially complex proposition when a child is injured. Very young children commonly do not recall the events at all or do so inaccurately because they may not have the capability to remember important details or differentiate between what is significant and what is not, are overwhelmed by fright or pain, are in denial, or fear punishment with disclosure of the truth. Fabrication (Munchausen syndrome) is rather common even in older children; it is, therefore, desirable to identify an adult eyewitness, although this is usually not possible. Furthermore, if a caregiver was present at the time of the injury, a word of caution is in order: he or she also may be interested in giving false information (see Nonaccidental Trauma below and also Chapter 57) so as to avoid personal responsibility. Table 56.8 lists the most important questions for the ophthalmologist. As a general rule, the ophthalmologist should primarily trust the findings from examination and be skeptical if these findings and the child’s/caretaker’s description of events are in conflict.
TABLE 56.8
The most important questions to ask when a child is injureda
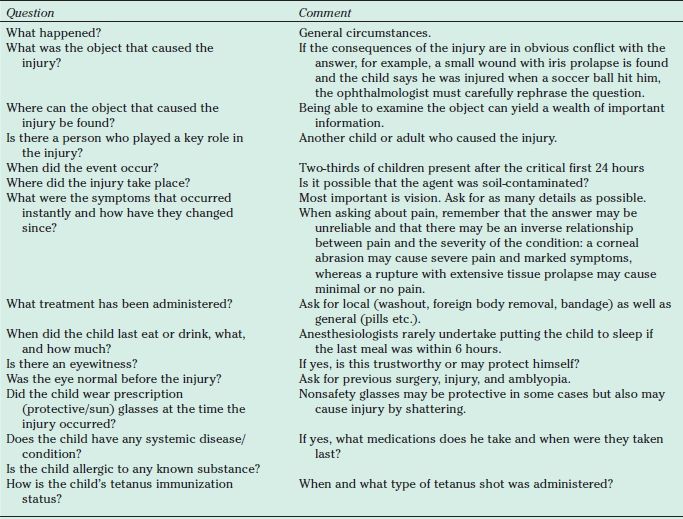
aThese are some of the most basic questions: According to the injury’s specific circumstances, the line of questions has to be modified in each individual case. The order must be changed accordingly, and, in some cases, for example, chemical injury, questions should be asked after emergency care has been delivered.
It may be advisable for the ophthalmologist not to wear a white coat when dealing with smaller children, who commonly associate the white coat with something negative such as pain.
Bilateral injury occurs in <3% of injuries in children. The unaffected eye offers an excellent control to which the injured eye can be compared if there is any doubt regarding the diagnosis.
The actual evaluation starts with an external inspection. The ophthalmologist must look for any injury-related tissue damage or foreign material on the lids and bones, the position of the globes (exophthalmos, enophthalmos, any deviation in primary position), and any asymmetry in the appearance of the eyes or orbits. A recent preinjury picture is useful to provide a basis for comparison. If possible, the child is asked to move the eyes in all directions to see if motility is retained. Motility restriction presents early in a blowout fracture if it is the trapdoor type. Small lid wounds may hide thin, long, and potentially life-threatening intraorbital foreign bodies that can protrude intracranially. When a penetrating orbital injury and systemic symptoms are present, always suspect brain injury (35). The history is often negative with organic intraorbital foreign bodies; hence, the skin and conjunctiva must carefully be examined.
Dog bites are commonly restricted to the skin and lacrimal system yet can cause severe infection, even death.
The globe is first examined with a penlight. Beforehand, the ophthalmologist should reassure the child that none of what’s coming will be painful and then indeed examine the child carefully so as not to cause pain. The penlight examination will help detect large foreign bodies (Fig. 56.4), significant prolapse of intraocular tissues, and large subcutaneous and subconjunctival hemorrhages. The penlight can also be used to examine the pupils and their reaction to light.
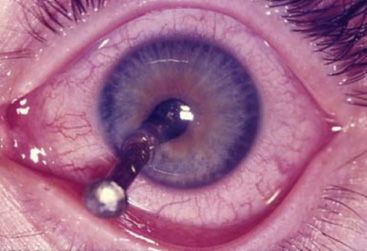
FIGURE 56.4 Intraocular but protruding foreign body raises a dilemma if the child is referred: should it be removed first? Although the decision must be made on a case-by-case basis, the general rule is not to remove it (see text for further details).
Examining very young or uncooperative children may require physical restraining, for which at least one assistant is necessary. Help provided by the parent or somebody closely known to the child is especially valuable. If no such person is available, a second assistant may be needed. The child should be placed on a fat surface, preferably onto a sheet that can be rolled around the child and in more than one layer, to immobilize all four extremities. The parent sits at the child’s legs and holds both legs and the arms, while the assistant, sitting at the child’s head, holds the head.
If adnexal injury is suspected, the ophthalmologist may need to perform a careful physical examination. Palpation may aid in finding bone dislocation, subcutaneous foreign bodies, and crepitus, but it is not always recommended because it also may cause pain and thus be counterproductive. It is, however, important to always examine the orbit, because orbital fractures are rather common in children.
If the lids are swollen, the child continues to squeeze them, or the need for surgical intervention is obvious, no effort should be made to forcibly open the lid: the risk of causing further tissue prolapse in an open globe injury is too great. It is preferred to have a thorough examination under sedation or mask anesthesia in the operating room (Fig. 56.5). Oral medication should be avoided so that general anesthesia remains an option. Consent for surgery should also be obtained prior to examination under anesthesia so that repair, if necessary, can be performed during the same sitting.

FIGURE 56.5 Child with an injury that obviously required surgical intervention. Further evaluation was not performed; the eye is examined only under general anesthesia and careful draping.
If possible, the visual acuity should be determined in both eyes. If the child is willing to cooperate but cannot read, illiterate charts, Allen cards, or the “E” sign can be used.
In older children and in younger children willing to cooperate, a slitlamp examination should be performed. A full evaluation should be attempted as appropriate, from the skin to the anterior vitreous or even the fundus with a 90-diopter lens, but the lids must never be forced open.
Conjunctiva: Smaller and thin hemorrhages are usually without significance, but large and thick hemorrhages may hide scleral wounds (occult rupture); if it is not possible to exclude with absolute certainty the possibility of a scleral wound under the subcon-junctival hemorrhage, exploratory surgery is recommended. A scleral wound also may be present under a conjunctival laceration, although the two wounds are not necessarily at the same location. Especially thick and widespread hemorrhagic chemosis raises the possibility of orbital pathology: fracture, foreign body, or hemorrhage. Bilateral periorbital hemorrhage should alert the ophthalmologist to the possibility of cranial fracture.
Cornea: The examiner must look for epithelial abrasions and ulcerations, stromal opacities, and wounds. Rose bengal stain can show damaged epithelial cells, and fluorescein can show epithelial loss. Signs and symptoms are not proportional to the severity or even the presence of corneal abrasions. For certain stromal injuries, such as those associated with foreign bodies, indirect, retroillumination, or sclerotic scatter can be useful. If a piece of glass is embedded deep in the cornea, it may be preferable to remove it at the slitlamp because the glass often becomes invisible under the operating microscope. If a corneal laceration is found, it must be determined whether the wound is of full thickness. If it is, the Seidel sign is positive: after instilling a drop of 2% fluorescein and viewing the wound under light emitted through a blue filter, a green stream is visible if aqueous is leaking from the anterior chamber. Sometimes slight pressure on the eye is necessary to observe the phenomenon (the so-called pressure Seidel sign). Not all full-thickness wounds require suturing, whereas some partial-thickness wounds, such as those with a displaced or very loose flap, do.
Anterior chamber: It must be evaluated for the presence of foreign bodies, fare, inflammatory cells, fibrin, pus, blood, and vitreous. A shallow anterior chamber may indicate aqueous loss, an anteriorly displaced lens, or a hemorrhagic or serous choroidal detachment, whereas a deep chamber may signal the presence of an open globe injury or a lens that has been extruded or posteriorly dislocated.
Iris: It should be examined under both direct illumination and retroillumination for full-thickness or stromal defects and sphincter tears. An iridodialysis or iridodonesis also may be present. To detect iridodonesis, eye movement is necessary.
Pupil: It is evaluated for shape, size, and location. The two pupils should be of equal size and have equal reaction to direct and consensual light. The presence or absence of an afferent pupillary defect (APD) should also be determined. The focused light from a penlight or ophthalmoscope is swung away from the intact onto the injured eye. If there is inadequate light perception or transmission from the injured eye, the pupil in the intact eye will dilate, instead of remaining constricted. Although both pupils should dilate if an APD in the injured eye is present, the advantage of inspecting the uninjured eye is that the pupils may not react in the directly traumatized eye for reasons other than an APD, such as an iris sphincter tear. The presence of an APD has a poor prognostic significance. If leukocoria is found, the ophthalmologist should always ask whether trauma has occurred to the eye.
IOP: It is rarely measured but may be assessed digitally (very cautiously if an open wound is present or suspected). Neither a low nor an elevated IOP is pathog-nomonic for an open wound.
Lens: It is examined for its presence, whether the anterior (and, more importantly, the posterior) lens capsule has been violated; clarity; position (dislocation or luxation); stability (phacodonesis); zonular rupture (often with coexistent vitreous prolapse); and presence of an intralenticular foreign body. All of these lens pathologies can occur in eyes with open globe injury and, with the exception of intralenticular foreign body, with closed globe injuries. For instance, contusion commonly causes anterior capsular rupture and cataract but, less commonly, isolated posterior capsular lesions as well. Of eyes undergoing surgery for traumatic cataract, up to one-half (36) were found to have posterior capsular ruptures.
Anterior vitreous: It is examined for the presence of foreign bodies, cells, fibrin, membranes, and hemorrhage.
Retina: Only easily identifiable pathology such as a retinal hemorrhage, edema, posterior break (macular hole), and detachment should be sought; examination of the retinal periphery is usually deferred until the presence of an open globe injury can be excluded.
Indirect ophthalmoscopy has certain advantages over the slitlamp when examining the vitreous and retina. Ideally, the pupils are dilated with sterile, short-acting, topical medications. Mydriatics should not be applied in the presence of an obvious open wound, and their use should always be documented. The retinal periphery usually is difficult to examine. Although retinal detachment is occasionally found, children usually present late with retinal detachment.
Most of the pathologies described can occur both in closed or open globe injuries. Table 56.9 presents useful hints in differential diagnosis.
TABLE 56.9
Probability of selected trauma-related pathologies in different types of globe injury–differential diagnosis
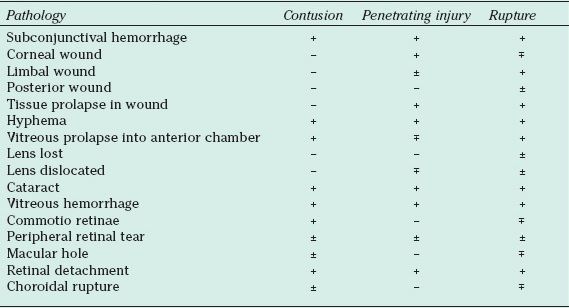
-, no or very rare; ±, rare; ±, relatively common; +, common.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


