FIGURE 5-1. Acute spastic entropion. Patient with a corneal abrasion. Continued irritation and blinking leads to an entropion.
INVOLUTIONAL ENTROPION
Eyelid laxity both horizontally and vertically predisposes to the instability of the lower eyelid. The additional factor required is the ability of the patient’s orbicularis muscle to override the tarsus and drive the eyelid inward. Patients present with red, irritated eyes from the eyelid margin and the eyelashes in contact with the eye itself.
Epidemiology and Etiology
• Age: More common in older patient population
• Gender: Equal occurrence in males and females
• Etiology: Horizontal laxity and orbicularis override result in inversion of the eyelid.
History
• Acute onset of eye irritation. This irritation is sometimes intermittent in nature and becomes more constant.
Examination
• Inverted lower eyelid with inferior corneal superficial punctate keratitis (SPK) or corneal abrasion (Fig. 5-2)
• Entropion is usually associated with horizontal eyelid laxity.
• Orbicularis muscle override is often noted as fullness over the tarsal plate when the lid is entropic.
• The entropion can be intermittent and not always present on examination.
• Placing topical anesthetic drops in the eye, having the patient close the eyes forcefully, and look downward will usually bring out the entropion.
Differential Diagnosis
• Cicatricial entropion
• Acute spastic entropion
Pathophysiology
• Aging of eyelid tissues results in laxity and stretching of supporting structures.
Treatment
• Surgical correction is based on correcting the factors contributing to the entropion, usually horizontal shortening of the eyelid and tightening the eyelid retractors in any of multiple ways.
Prognosis
• Excellent. There is a 5% to 10% chance of recurrence over 5 to 10 years.

FIGURE 5-2. Involutional entropion. Left lower eyelid entropion with involutional changes. The rolled in orbicularis muscle can be seen driving the eyelid margin inward on the left.
CICATRICIAL ENTROPION
Cicatricial entropion is caused by conjunctival scarring pulling the eyelid inward. Generally, treatment is surgical, but defining and treating the cause of the conjunctival scarring must be done first or most cases will recur. Occurs in the upper or lower eyelid.
Epidemiology and Etiology
• Age: Any age
• Gender: Equal occurrence in males and females
• Etiology: Scar tissue on the conjunctival surfaces results in shortening of the posterior lamella, physically pulling the eyelid inward.
• Factors include:
 Surgery
Surgery
 Conjunctival scarring diseases (e.g., ocular cicatricial pemphigoid, Stevens-Johnson syndrome, trachoma)
Conjunctival scarring diseases (e.g., ocular cicatricial pemphigoid, Stevens-Johnson syndrome, trachoma)
 Trauma
Trauma
 Conjunctival burns (e.g., chemical)
Conjunctival burns (e.g., chemical)
 Antiglaucoma drops
Antiglaucoma drops
History
• Chronic low-grade inflammation over months to years results in the entropion that then causes more irritation.
• The other scenario is a history of trauma or surgery resulting in an entropion and associated irritation.
Examination
• Careful evaluation of the conjunctiva for signs of scarring causing inversion of the eyelid.
• This may include evaluation of the other eyelids to determine if the entropion is isolated or involving all four eyelids, which may help determine the etiology (Fig. 5-3).
Special Considerations
• Must determine the etiology of the conjunctival scarring before treating.
• Any progressive disease must be quieted before surgery can be done on the eyelids.
Differential Diagnosis
• Acute spastic entropion
• Involutional entropion
Laboratory Tests
• Conjunctival biopsy with immunofluorescence testing if ocular cicatricial pemphigoid is suspected.
Treatment
• Determine the etiology of the conjunctival scarring.
• Quiet any active disease.
• Surgical correction of the entropion with a marginal rotation or buccal mucosal graft is then the treatment of choice.
Prognosis
• Variable depending on the etiology
• Entropion secondary to trauma and surgery usually do very well.
• Progressive disease processes, such as ocular cicatricial pemphigoid, can make it much more difficult to prevent recurrence of the entropion.
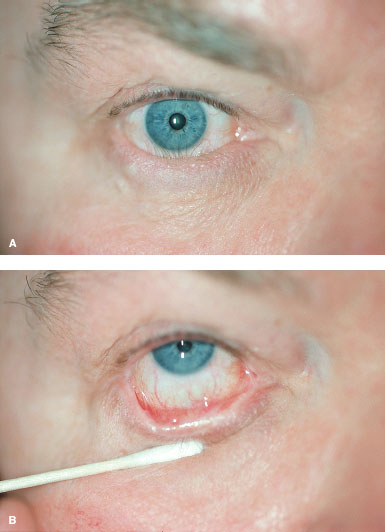
FIGURE 5-3. (Cicatricial entropion. Externally A), it is difficult to differentiate this cicatricial entropion from an involutional entropion until the eyelid is everted (B), and the cicatricial changes are noted pulling the eyelid inward.
ECTROPION
INVOLUTIONAL ECTROPION
Involutional ectropion has the same involutional factors as in an involutional entropion (e.g., horizontal laxity, vertical instability). These patients do not have hypertrophic, spastic orbicularis muscle to override, so the unstable eyelid sags outward instead of being driven inward. Symptoms are less acute and not as severe as in involutional entropion. Many patients will have mild involutional ectropions and may be asymptomatic.
Epidemiology and Etiology
• Age: Incidence increases as age increases.
• Gender: Equal occurrence in males and females
• Etiology: Eyelid tissue laxity, especially horizontal laxity
History
• Insidious onset of ocular irritation and/or tearing
• Patient may note redness and inflammation of the eyelid margin.
Examination
• Eyelid sagging inferiorly and away from the globe surface (Fig. 5-4)
• Must look for the amount of horizontal laxity, corneal exposure, and stenosis of the lacrimal puncta.
Special Considerations
• Tarsal ectropion is complete eversion of the eyelid and indicates detachment of the lower eyelid retractors.
• This condition must be recognized, as it requires both horizontal tightening and reattachment of the retractors.
Differential Diagnosis
• Cicatricial ectropion
• Paralytic ectropion
Treatment
• Mild ectropion with only mild exposure symptoms can sometimes be treated with ocular lubrication.
• Definitive treatment involves horizontal eyelid shortening and possible punctoplasty.
Prognosis
• Excellent. Recurrence after surgery is estimated at 5% to 10%, but is higher the longer the follow-up is done and the more severe the ectropion was at the time of the repair.

FIGURE 5-4. Involutional ectropion. Bilateral ectropions with very lax eyelids. Note the red palpebral conjunctiva from chronic exposure.
PARALYTIC ECTROPION
Paralytic ectropion is the result of temporary or permanent seventh cranial nerve palsy. The lower eyelid sags away from the globe, resulting in loss of protection of the eye and inability of the lacrimal system to collect tears. Patients with less severe palsy and other eye protective mechanisms intact present with tearing. Patients with more severe palsies and poor eye protection mechanisms present with corneal breakdown.
Epidemiology and Etiology
• Age: Any age
• Gender: Equal occurrence in males and females
• Etiology: Facial palsy etiologies include:
 Bell’s palsy
Bell’s palsy
 Surgery: intracranial or facial
Surgery: intracranial or facial
 Stroke
Stroke
 Tumor
Tumor
History
• Previous onset of facial palsy
• Depending on the severity of the facial palsy, the ectropion may have onset at the same time or the eyelid may slowly sag with time.
• The severity of the condition depends on the severity of the paralysis, corneal sensation, and ocular lubrication.
Examination
• The lower eyelid is found to be sagging away from the globe (Fig. 5-5).
• Evaluate severity of facial palsy, degree of ectropion, amount of corneal exposure, amount of lagophthalmos, and presence of an intact Bell’s phenomenon.
Special Considerations
• Must check for corneal sensation as loss of corneal sensation will make all exposure symptoms much worse.
• Any unexplained facial palsy must be worked up.
Differential Diagnosis
• Bell’s palsy versus nonresolving facial palsy
Treatment
• Treatment depends on the anticipated duration of the paralysis.
• If spontaneous improvement is anticipated, then treatment with lubrication and a temporary tarsorrhaphy if severe corneal problems are present is indicated.
• If corneal exposure is still a problem with lubrication use and the paralysis is long term, then horizontal eyelid tightening is used to treat the paralytic ectropion.
• Placing a gold weight in the upper eyelid may also be required. Rarely, a permanent tarsorrhaphy may be needed.
Prognosis
• Variable. The ectropion tends to recur over time if the paralysis is permanent.

FIGURE 5-5. Paralytic ectropion. Right lower eyelid ectropion as the result of a facial palsy.
CICATRICIAL ECTROPION
Cicatricial ectropion is caused by mechanical shortening of the anterior lamellae of the eyelid pulling the eyelid down and outward. This results in tearing and corneal exposure. More common in the lower eyelid but can occur in the upper eyelid.
Epidemiology and Etiology
• Age: Any age
• Gender: More common in males because of higher incidence of traumatic events.
• Etiology: Scarring of the anterior lamellae of the eyelid pulls the eyelid outward. The etiologies include:
 Trauma
Trauma
 Surgery
Surgery
 Dermatitis
Dermatitis
 Skin carcinoma
Skin carcinoma
History
• May include a specific history such as trauma or surgery
• If a chronic dermatologic condition is the cause of the scarring, this may be a known or a previously unrecognized condition.
Examination
• External scarring or skin changes are noted on the upper or more commonly the lower eyelid.
• This scarring results in shortening of the eyelid skin and out-turning of the eyelid margin (Fig. 5-6A).
Special Considerations
• Must always consider a skin carcinoma as the possible cause of scarring of the skin. If the cause is unclear, a biopsy is needed.
Differential Diagnosis
• Important to differentiate involutional ectropion from those with cicatricial changes.
Treatment
• Treatment of any underlying dermatologic condition is important.
• In traumatic or postsurgical cases, the scarring should be left for 6 months or longer unless exposure or other problems necessitate earlier treatment.
• Treatment involves lysis of any deep scar tissue with horizontal tightening.
• If the skin shortening is severe, full-thickness skin grafts will be required.
• Skin grafts have the potential for scarring and a cosmetically noticeable area at the graft site (Fig. 5-6B).
Prognosis
• Trauma or surgically induced cases do well with repair.
• Chronic conditions of the skin tend to result in recurrences.
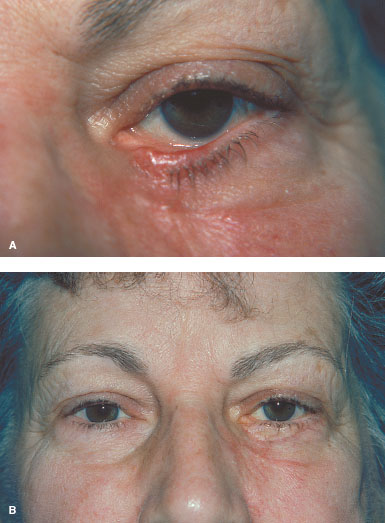
FIGURE 5-6. Cicatricial ectropion. A. Trauma to the left lower eyelid results in scarring of the skin with vertical shortening as well as scarring internally within the eyelid. B. After repair, using a skin graft.
MECHANICAL ECTROPION
Mechanical ectropion is a rare cause of ectropion in which a mass of some type pushes the eyelid outward. There are usually associated involutional changes that allow the eyelid to be pushed outward.
Epidemiology and Etiology
• Age: Older patients
• Gender: Equal occurrence in males and females
• Etiology: Gravity pulls the eyelid away from the eye or pushes the eyelid away from the eye secondary to a mass. Causes of the mass effect include:
 Dermatochalasis
Dermatochalasis
 Edema
Edema
 Chalazion
Chalazion
 Eyelid tumor (e.g., hemangioma, inclusion cyst)
Eyelid tumor (e.g., hemangioma, inclusion cyst)
History
• Patient may be asymptomatic, have symptoms of corneal irritation, or have redness and irritation of the eyelid.
Examination
• Must determine the degree of involutional changes of the eyelid as well as the etiology of the mass distorting the eyelid.
• The amount of corneal exposure and any corneal scarring should also be noted (Fig. 5-7).
Differential Diagnosis
• Involutional ectropion
• Cicatricial ectropion
• Paralytic ectropion
Treatment
• Excision of the mass and correction of the involutional factors of the eyelid
Prognosis
• Good if the mass can be eliminated
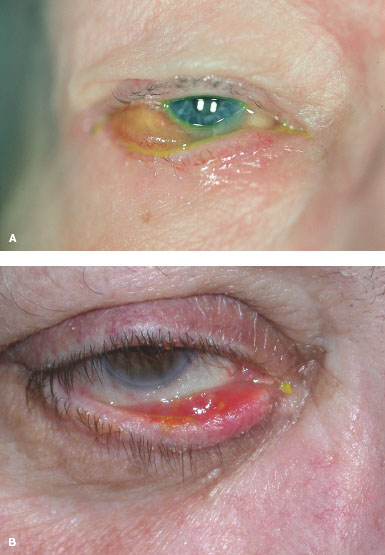
FIGURE 5-7. Mechanical ectropion. A. Chemosis from an inflammatory process mechanically pushes the lower eyelid outward. There are usually some involutional changes present to allow the eyelid to be pushed out. Resolution of the chemosis allowed the eyelid to return to a normal position. B. Mechanical ectropion from a chalazion. Even with chalazion resolution, the ectropion may remain.
SYMBLEPHARON
• Symblepharon is scarring between the bulbar and palpebral conjunctiva. This may be associated with active inflammation or there may be no inflammatory signs.
Epidemiology and Etiology
• Age: Any age
• Gender: More frequent in women
• Etiology: The following can result in scarring of two conjunctival surfaces:
 Chronic blepharitis
Chronic blepharitis
 Previous trauma
Previous trauma
 Conjunctival scarring diseases (e.g., ocular cicatricial pemphigoid, Stevens-Johnson syndrome)
Conjunctival scarring diseases (e.g., ocular cicatricial pemphigoid, Stevens-Johnson syndrome)
 Atopic disease
Atopic disease
 Eyelid surgery
Eyelid surgery
 Conjunctival burns
Conjunctival burns
 Chronic glaucoma drops, especially miotics
Chronic glaucoma drops, especially miotics
History
• There may be no history, just asymptomatic symblepharon noted on examination.
• Patients with history of eye or eyelid trauma or inflammation may also have symblepharon.
Examination
• Scarring of the conjunctival surfaces may be very subtle with slight inferior fornix shortening or it may be very obvious with large conjunctival bands between the eye and eyelid (Fig. 5-8).
• Must be sure to examine under the upper lid for conjunctival scarring, as early signs are sometimes more obvious there.
Special Considerations
• It is important to determine the cause of the symblepharon.
• If asymptomatic, the symblepharon may require no treatment except looking for the cause of the scarring.
• Ruling out a progressive conjunctival scarring disease, such as ocular cicatricial pemphigoid, is important.
Differential Diagnosis
• The differential diagnosis involves determining the cause of the symblepharon, not whether the process is a symblepharon.
Laboratory Tests
• Conjunctival scarring of unknown etiology requires a conjunctival biopsy with immunofluorescence testing to rule out ocular cicatricial pemphigoid.
• In rare cases, squamous cell carcinoma may cause symblepharon; therefore, pathologic evaluation should be considered in select cases.
Treatment
• None for mild symblepharon
• Monitoring for progression is important.
• Significant symblepharon may cause trichiasis and cicatricial entropion that then may require treatment.
Prognosis
• Variable depending on the cause of the symblepharon
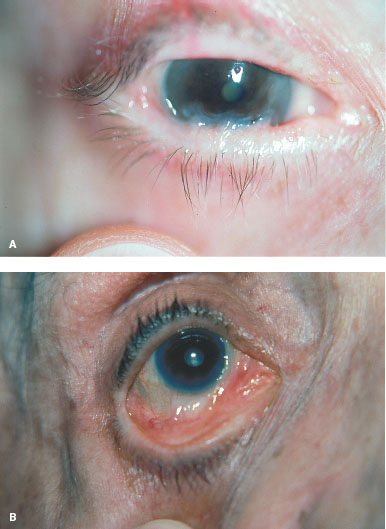
FIGURE 5-8. Symblepharon. A. Scarring is seen between the eyelid and the inferior cornea. B. Early symblepharon may be noted only as shortening of the fornix.
TRICHIASIS
Trichiasis is an acquired misdirection of eyelashes. Trichiasis may be focal, as is seen after eyelid trauma in the area of the laceration. The process may be diffuse with eyelid scarring and lashes along the entire eyelid margin.
Epidemiology and Etiology
• Age: Any age. Nontraumatic causes are rare in childhood. More common with increasing age.
• Gender: More common in females
• Etiology: Lash follicles are distorted and become misdirected with scarring of the eyelid. Chronic eyelid inflammation may result in growth of misdirected lashes. Chronic blepharitis, eyelid trauma, and conjunctival scarring diseases can all cause trichiasis.
History
• Patients will often have a history of chronic eye irritation and inflammation. They may also have a long history of eyelash problems. There may be a history of eyelid trauma or surgery.
Examination
• Eyelashes are seen rubbing on the eyelid surface (Fig. 5-9).
• The amount of corneal changes depends on the number of lashes and duration. There may be just SPK or there may be corneal scarring.
Special Considerations
• Important to differentiate trichiasis from abnormal eyelid positions, such as entropions, which secondarily result in eyelashes rubbing on the cornea.
Differential Diagnosis
• Spastic entropion
• Involutional entropion
• Cicatricial entropion
• Congenital distichiasis
Laboratory Tests
• Conjunctival scarring of unknown etiology requires a conjunctival biopsy with immunofluorescence testing to rule out ocular cicatricial pemphigoid.
Treatment
• Lashes can be epilated for temporary relief but they always grow back.
• Electrolysis or cryotherapy will ablate lashes on a more “permanent” basis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


