FIGURE 49.1 Contraction of proliferation intrinsic to the circumferential ridge (arrow), resulting in a radial fold.
2. Ridge to lens (Fig. 49.2). The most common and easily conceptualized traction vector, and the most important to interrupt surgically, often extends circumferentially from the ridge toward the midperipheral lens.
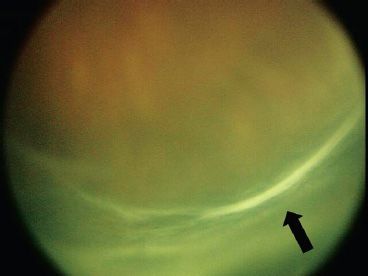
FIGURE 49.2 Proliferation extending anteriorly from the ridge toward the lens in an anteriorly open–posteriorly open funnel detachment. Traction originates at the ridge in a circumferential, purse-string pattern that draws the retina anteriorly and centrally (arrow).
3. Ridge to ridge (Fig. 49.3). This vector extends as a sheet across the “mouth” of the developing funnel-shaped retinal detachment.
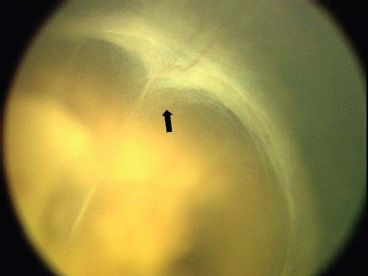
FIGURE 49.3 Sheet of proliferation originating from the ridge and extending across the “mouth” of the funnel-shaped retinal detachment toward the contralateral ridge (arrow).
4. Ridge to ciliary body (Fig. 49.4). This vector extends from the ridge anteriorly toward the ciliary body.
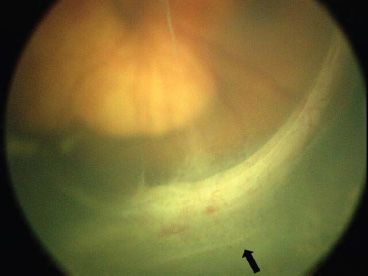
FIGURE 49.4 Sheet of proliferation originating from the ridge extends anteriorly toward the ciliary processes (black arrow).
5. Ridge to retina. This traction extends from the elevated ridge back toward the portion of the retina just anterior to the original location of the ridge.
6. Disc stalk. There are three variants of the proliferative tissue extending from the optic disc: (i) a typically very adherent epiretinal sheet extending along the retinal surface to the ridge often seen in eyes in which the ridge is located posterior to the equator, (ii) a transvitreal stalk extending to the ridge usually seen in eyes with an equatorial ridge, and (iii) a transvitreal sheet extending from ridge-to-ridge sheet usually seen in eyes with a ridge located anterior to the equator (Fig. 49.5).
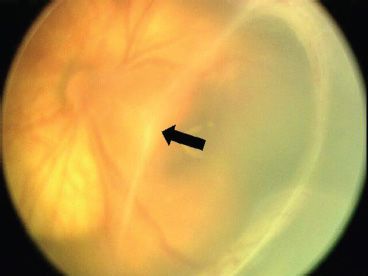
FIGURE 49.5 Central “T-shaped” stalk extending transvitreally from the optic disk (out of focus) anteriorly to join with the ridge-to-ridge sheet (arrow).
Some or all of these components are present in all ROP-related retinal detachments. The configuration of the detachment is determined by the overall tractional contribution of the multiple force vectors.
The surgical goal in eyes with macula-sparing ROP–related traction retina detachments (stage 4A ROP) is an undistorted or minimally distorted posterior pole, total retinal reattachment, and preservation of the lens and central fixation vision (Figs. 49.6 and 49.7). Surgery for tractional retinal detachments involving the macula (stage 4B ROP) is performed to minimize retinal distortion and prevent total retinal detachment (Figs. 49.8 and 49.9). The practical surgical goal is to reattach as much of the retina as is possible without causing a retinal break. Partial residual retinal detachment and retinal drag/distortion are common in such eyes. The functional goal for stage 4B eyes is ambulatory vision.

FIGURE 49.6 Nasal stage 4A ROP–related tractional retinal detachment located in zone I in a 38-week-old infant 1 month following laser.

FIGURE 49.7 Resolved nasal stage 4A ROP–related tractional retinal detachment seen in Figure 49.6 following lens-sparing vitreous surgery. Straightening of the vessels inferonasal to the optic disc is the only residuum of the tractional detachment following vitrectomy.
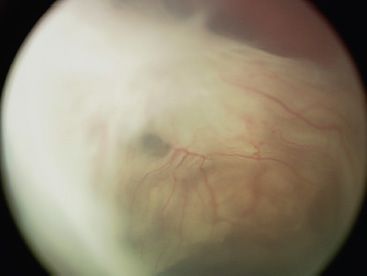
FIGURE 49.8 Stage 4B ROP–related tractional retinal detachment prior to surgery. The red reflex visible superiorly is an area of attached retina.
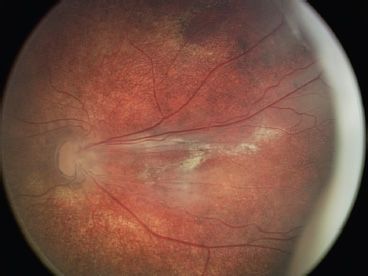
FIGURE 49.9 Attached posterior retina with residual subretinal lipid in the eye seen in Figure 49.8 following lensectomy and vitrectomy.
Vitreous surgery can interrupt progression of ROP from stage 4A to stages 4B or 5 by directly addressing transvitreal traction resulting from fibrous proliferation and may also reduce dragging of the macula. In experienced hands, lens-sparing vitrectomy allows primary retinal reattachment in 90% of eyes with stage 4A ROP (4–10). Early visual outcomes appear encouraging as well (14). In a cohort of 11 consecutive eyes of children able to cooperate with Teller visual acuity testing (mean age 2.5 years), Snellen equivalent was 20/80 or better in eight eyes (73%) (5). Similar results have been reported by others for stage 4A ROP (15), with positive outcomes also reported for eyes with stage 4B detachments (16).
The surgical goal for stage 5 ROP is to reattach as much of the retina as possible (Figs. 49.10 and 49.11). As with stage 4B detachments, partial residual retinal detachment is common. Form vision can be preserved following vitrectomy for stage 5 ROP (11,17). Lower levels of vision can be measured by detecting the perception of light in different fields of vision as determined in different levels of illumination (13). This measurement permits one to stratify low levels of vision and then follow low vision in infants treated for stage 5 ROP. Maximal recovery of vision following the insult of macula-off retinal detachment and interruption of visual development in infants may take years.

FIGURE 49.10 Stage 5 ROP–related tractional retinal detachment prior to surgery demonstrating retrolental fibroplasia. The red reflex visible superiorly is an area of attached retina.

FIGURE 49.11 Attached posterior retina with residual subretinal lipid in the eye seen in Figure 49.10 following lensectomy and vitrectomy.
ROP-related detachments may appear stable in the first few weeks or months after peripheral retinal ablation. Yet neither the stability of the partial detachment nor visual acuity is predictable from the retinal appearance in infants with ROP. This is particularly true for untreated eyes or those with incomplete peripheral retinal ablation. ROP-related retinal detachments can progress—often very gradually—for years. As the eye grows, the cicatricial proliferation does not, and retina tethered to the eye wall is vulnerable to stretching to the point of tractional detachment or development of a retinal break.
Visual outcome of eyes with even partial ROP-related retinal detachment is generally poor by age 4.5 years. In the cohort of 61 eyes from the Multicenter Trial of Cryotherapy for Retinopathy of Prematurity study with partial retinal detachment 3 months after threshold, only six eyes had vision of 20/200 or better at age 4.5 years (1,18). The difficulty exists in determining whether an eye with residual or recurrent features of threshold ROP will develop progressive stage 4 ROP or show regression after laser treatment. One retrospective study of retinal features in eyes treated with laser for threshold ROP determined that ≥6 clock hours of ridge elevation, ≥2 quadrants of plus disease, and vitreous haze were predictive of progressive stage 4 ROP and that these features should indicate to the ophthalmologist that this patient likely will require surgery to prevent stage 4B ROP (19). The study was retrospective and did account for the correlation between eyes in the same infant by using a generalized estimating equation model. Others have found the importance of even a clock hour of bleeding or fibrovascular proliferation associated with the ridge as causative harbinger of progressive retinal detachment and vision loss. More recently, investigators found that recurrent neovascularization in previously treated avascular retina was a cause of subsequent retinal detachment (20
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


