FIGURE 48.1 Image of scleral buckle in place. Position of the encircling element, a 2.5-mm solid silicone band, is shown. Sponge elements are often used to create a large indentation to overcome lesser amounts of PVR.
It often is difficult to ascertain symptoms in the younger, especially preverbal, child. Therefore, the child often already has some PVR on the presenting examination. We believe larger buckles can be helpful in overcoming the tractional forces caused by the PVR. Customarily, the child is evaluated approximately 3 months after scleral buckling to determine if division of the buckle is possible. We usually do not remove the buckling element in toto but leave the large buckling element in place and divide the encircling band in an area where the retina is fat without any clinical evidence of traction. In children, capsular tissue can form rapidly around the scleral buckle, even after a relatively short period of time. This is noted on attempted division of the encircling band. The band can be located by tapping gently in the area where it is suspected with a closed pair of forceps. Once the band’s location is determined, a hockey stick–like blade can be used to make a 2- to 3-mm incision through the capsule in the direction along the length of the band. The band then can often be lifted from the sclera and divided with scissors. After longer periods of time, even 6 to 12 months, the band might rarely erode into or through the sclera. In that situation, it is important to avoid any deep tissue dissection. Sometimes division of the band over the larger buckling element can be performed. In the author’s experience, it is extremely rare that redetachment results after division of the encircling elements, particularly in eyes where buckling has been performed for a predominantly nonrhegmatogenous retinal detachment.
Drainage of subretinal fluid is always an important consideration. Drainage should be considered in all eyes in which all traction is relieved and the areas of the retina and retinal pigment epithelium (RPE) are similar. If the retina is stretched and all traction is not removed, drainage of subretinal fluid can be dangerous and lead to retinal breaks. Therefore, drainage is rarely performed in ROP and familial exudative vitreoretinopathy (FEVR). Drainage might be considered in these cases if there is a total retinal detachment with extensive amounts of subretinal fluid; then, often only partial drainage is performed to reduce the risk of iatrogenic retinal tears. In addition, unless there is an existing retinal break, which makes intraretinal drainage possible in vitreous surgery, external drainage is more desirable. This is true because it is unlikely that the posterior hyaloid can be mechanically removed in a child during standard vitreous surgery.
Vitreous surgery over the last 15 years has become increasingly useful in pediatric retinal diseases. As better understanding of the pathophysiology of these retinal diseases evolves, the role of vitreous surgery in altering the mechanical scaffolding of the vitreous or the biochemical interactions present in the vitreous cavity expands. From an instrumentation standpoint, three-port and two-port vitrectomy, and open-sky vitrectomy, can be used for pediatric indications. The authors most commonly use two-port vitrectomy with a variety of instruments that allow two-hand dissection (Table 48.1). These are the wide-angle high-flow light pipe, the infusion spatula, the infusion forceps, and the retractable-lighted pick or an irrigating illuminated pick (Fig. 48.2). These, in addition to the vitreous cutter and membrane peeler cutter (MPC) scissors, make up the instrumentation customarily used by the authors for vitreous surgery in infants and children. The viewing system used is an operating microscope with adjustable horizontal and vertical movement (X–Y) and the BIOM wide-angle viewing system. At this time, there does not appear to be a significant advantage to using smaller than 20-gauge instruments. In fact, some stiffer proliferative tissue may be difficult to deform and draw into the smaller port. Smaller instruments may become useful with the future development of enzymatic manipulation of vitreous collagen. They may have the advantage of being more safely and freely moved behind the lens and across the phakic eye. Currently, 23-gauge pediatric instruments are being developed to allow manipulation of more dense tissue.
TABLE 48.1
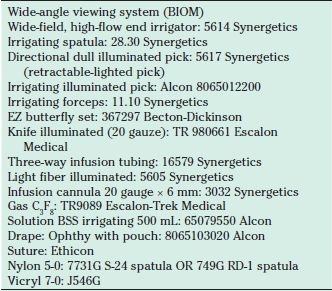
C3F8, perfluorooctane; BSS, balanced salt solution.
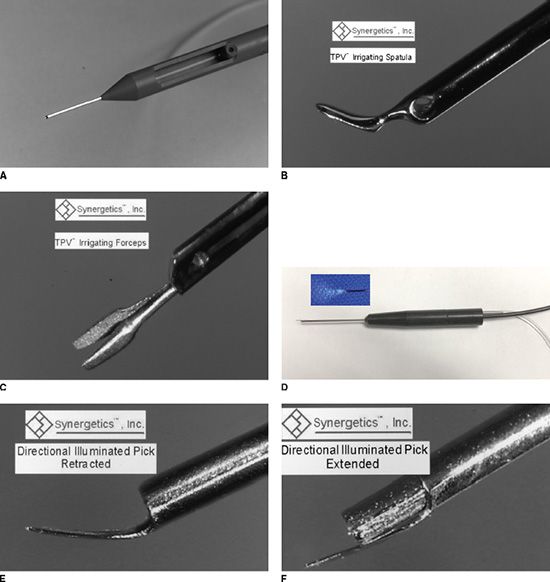
FIGURE 48.2 A: Wide-angle high-flow light pipe. B: Infusion spatula. C: Irrigating forceps. D: Irrigating illuminated pick (tip shown in inset). E: Tip of the retractable lighted pick–retracted. F: Tip of the retractable lighted pick–extended.
The location of the sclerotomies often is determined by the anatomy of the pathology and the age of the child. The premature eye does not have a pars plana; therefore, entry into the vitreous cavity should be performed through the pars plicata approximately 0.5 mm posterior to the limbus. A developed pars plana is not present until 8 to 9 months postterm (3). In retinal detachments, with vitreoretinal membranes that contact the posterior lens capsule, a lensectomy–vitrectomy often is required to relieve the vitreous traction and permit the retina to reattach. We often use a 23-gauge butterfly needle (Fig. 48.3), bent so as to allow infusion into the anterior chamber without contacting the corneal endothelium, while the vitreous cutter is used to remove the lens within the capsule. Alternatively, anterior segment infusion is effected via an anterior chamber infusion cannula (Lewicky anterior chamber maintainer or right-angled 20-gauge infusion cannula). The entry for the lensectomy–vitrectomy in the premature eye is located immediately posterior to the limbus through the iris root directed into the lens anterior to the equator of the lens. This avoids the possibility of injuring the retina pulled anteriorly into the posterior chamber. When the lens is aspirated, the capsule is removed using a broad fat Sutherland forceps. The Sutherland forceps grasps the capsule approximately one-third of the distance from the equator to the posterior pole of the lens; in that fashion, frequently all of the capsule can be removed at once. Complete removal of the capsule is essential to remove all of the cells that can lead to subsequent retinal iridal adhesions postoperatively—a common mode of failure of vitreous surgery in children. When lensectomy is performed in the absence of a fibrous proliferative sheet immediately behind the lens, the capsule is removed with the vitrector.
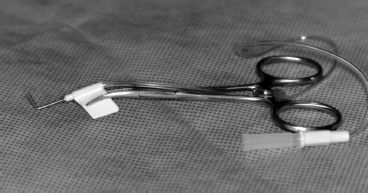
FIGURE 48.3 A 23-gauge butterfly needle mounted on a hemostat to be used as infusion with a sharp tip.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


