FIGURE 46.1 Skin of the area of the target vein is held taut as the tip of the IV cannula enters the skin 1 to 2 mm away from the target vein.

FIGURE 46.2 Target vein is entered with a deliberate 1- to 2-mm thrust of the IV cannula into the vein.

FIGURE 46.3 Intravenous catheter is connected to the IV tubing with a Luer-Lok T piece.

FIGURE 46.4 Medications are administered directly at the site of the T piece.
Only preservative-free saline can be used as a flush solution for these neonates, because flush solutions containing benzyl alcohol can precipitate acidosis in small babies.
For short procedures that allow easy access to the neonate’s airway, the LMA is ideal (8). The LMA has been shown to provide a satisfactory airway in infants with BPD during minor surgical procedures and results in fewer respiratory problems compared to an endotracheal tube. Procedures such as extended eye examination under anesthesia and laser surgery allow for easy placement of an LMA and rapid reinsertion of the LMA, should it become dislodged. We do not recommend the use of the LMA for open-eye procedures where the patient’s entire head and neck are covered by surgical drapes and easy access to the LMA would not be available. We have had one extreme situation of a neonate with severe reactive airway disease accompanying BPD. In this situation, the bronchospasm was precipitated by intubation. An LMA was used successfully for an open-eye procedure, but great care was taken by the surgical and anesthesia teams to secure and not dislodge the LMA during the procedure. Use of the LMA for an open-eye procedure is the rare exception and is not recommended unless the infant does not tolerate intubation well.
When we are certain we have adequate ventilation via mask airway, have established IV access, and plan to proceed with oral endotracheal intubation, we administer IV rocuronium, 1 mg/kg for muscle relaxation.
Prior to commencing anesthetic induction, the three sizes of uncuffed endotracheal tubes (2.5-, 3.0-, and 3.5-mm internal diameter) used in neonates should be available, with stylets in place. For most neonates, a laryngoscope fitted with a Miller 0 laryngoscope blade is the instrument of choice for intubation. The anesthetist should hold the laryngoscope handle close to the laryngoscope blade to allow use of his or her fifth finger to apply external pressure over neonate’s cricoid cartilage. This pressure pushes the glottis into view when the tip of the laryngoscope blade is pulling up on the neonate’s epiglottis. During laryngoscopy, this maneuver will maximize the chances of good visualization of the glottis of the neonate for successful intubation (Figs. 46.5A and B and 46.6).
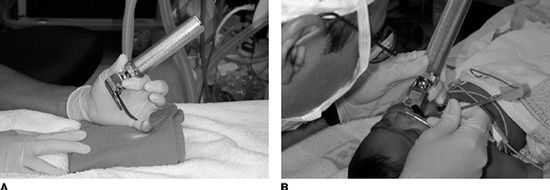
FIGURE 46.5 Laryngoscope is held close to the laryngoscope blade.

FIGURE 46.6 Fifth finger of the anesthetist’s hand holding the laryngoscope is used to place pressure over the infant’s cricoid cartilage.
For maintenance of general anesthesia, we generally change over from sevoflurane to isoflurane because isoflurane is less toxic when given for a long period of time. We rarely administer any narcotic to these neonates for ROP surgery because of their decreased ability to metabolize narcotics and our desire to establish a normal respiratory pattern as soon as possible after anesthesia to facilitate extubation. For neonates who will remain intubated for a long period after surgery with general anesthesia, we titrate small amounts of IV fentanyl.
We have encountered a few neonates who have severe reactive airway disease and do not tolerate more than moderate-to-low inspired concentrations of sevoflurane or isoflurane. In these cases, we have used low concentrations of sevoflurane or isoflurane augmented with propofol infusion. We begin the propofol infusion at 100 µg/kg/min and titrate up or down as the clinical situation requires. We use IV rocuronium for muscle relaxation as needed.
CRISIS AND TREATMENT OF BRONCHOSPASM
One of the most difficult anesthetic complications to deal with when anesthetizing the VLBW infant for ROP surgery is bronchospasm. Although rare, bronchospasm occurs in the VLBW infant with moderate-to-severe BPD, at about 1 to 3 months after birth. The bronchospasm, which probably is a combination of airway smooth muscle and arterial smooth muscle contraction, can be of sudden onset and lead to rapid oxygen desaturation. Bronchospasm can be very difficult to treat. If it does not abate with positive pressure via face mask or endotracheal tube, we administer IV epinephrine in 1-µg boluses until the bronchospasm improves or the heart rate is >215 beats/min. Sometimes, increasing the sevoflurane concentration helps relieve the bronchospasm; at other times, the sevoflurane must be discontinued to stop bronchospasm. It is important to emphasize that this type of sudden severe bronchospasm is rare.
Because of limited respiratory reserve, the VLBW infant with BPD should not receive elective general anesthesia when the infant has an upper respiratory infection (URI). Infants and children with a URI are more likely to have respiratory complications. These patients already have significant respiratory compromise and should not be placed at greater risk than necessary when receiving general anesthesia for ROP surgery. These infants may require a full 6 weeks to recover from a URI to be suitable for elective general anesthesia.
EXTUBATION IN OPERATING ROOM VERSUS TRANSPORT TO NEONATAL INTENSIVE CARE UNIT WITH SLOW EXTUBATION
Most VLBW infants aged 4 months or older with mild-to-moderate lung disease will tolerate extubation in the operating room after the ROP eye surgery is completed. Some of the VLBW infants in this age group with severe lung disease will require postoperative ventilatory support. Most of the VLBW infants will require postoperative apnea monitoring, and many of these infants will be on continuous apnea monitoring at home.
Anesthetic care of the VLBW infant for ROP surgery requires a trained pediatric anesthetist. These patients require extra time and consideration because of the fragility of their physical condition caused by the multiple medical problems of extreme prematurity.
Tables 46.1 to 46.8 list the guidelines for medications, endotracheal tubes, and LMAs we use at William Beaumont Hospital, Royal Oak, Michigan.
TABLE 46.1
William Beaumont Hospital basic pediatric anesthesia drugs
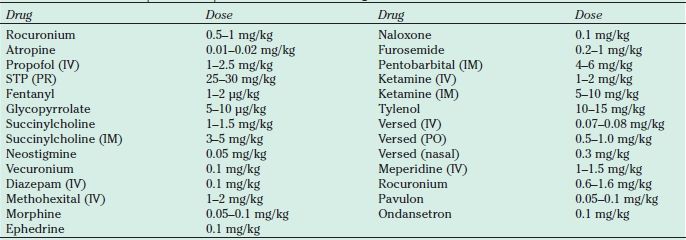
STP, sodium pentothal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


