FIGURE 44.1 Effect of VEGF in normal vascular development.
FIGURE 44.2 ROP vascular phases and effusive retinal detachment phase biochemically.
In the fetus, wound healing responses and scar formation differ depending on the developmental time in utero. For example, fetal regenerative wounds heal without scar formation in the second and early third trimesters (12). Transforming growth factor-β1 (TGF-β1) has been widely studied regarding its effects on wound healing and in the eye. TGF-β1 leads to excessive scar formation in fetal wounds and contributes to hyaluronic acid synthesis (13). It differentially affects adult and fetal fibroblast migration and hyaluronan synthesis (14). In addition, it downregulates VEGF in cell culture (11). Although direct evidence is lacking, TGF-β is present in fetal development and conceivably could affect collagen structure, vascularity, and wound healing in the eye. These processes could participate in the development of retinal detachment seen in stage 4 and 5 ROP.
CLINICAL FEATURES OF RETINAL DETACHMENT IN RETINOPATHY OF PREMATURITY
The International Classification of Retinopathy of Prematurity describes retinal detachments as stage 4A, 4B, and 5 (15). Others have also used the term predominantly effusive and predominantly tractional to further classify these detachments.
The predominantly effusive retinal detachment has a characteristic shape. The retina is convex toward the examiner and smooth with fluid extending primarily posterior to the ridge detaching the ridge and macula. This detachment begins at the ridge. Some of the components of this subretinal fluid are blood products (16). Accordingly, subretinal fluid may vary from relatively clear to turbid or bright red in color. Effusive detachments are less common now that cryotherapy is used less frequently than laser (Figs. 44.2 to 44.4).
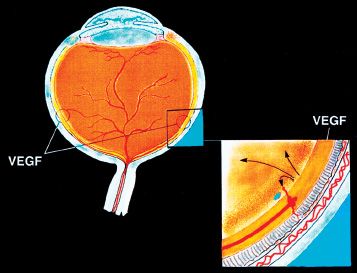
FIGURE 44.3 Schematic drawing showing the area of highest VEGF concentration anterior to the advancing retinal vascular ridge. The inset shows the relationship of developing intraretinal and extraretinal vascularization contributing to the formation of subretinal blood (effusive retinal detachment) and the areas of cellular elements (primary vitreous and tunica vasculosa lentis) contributing to predominantly tractional retinal detachment.
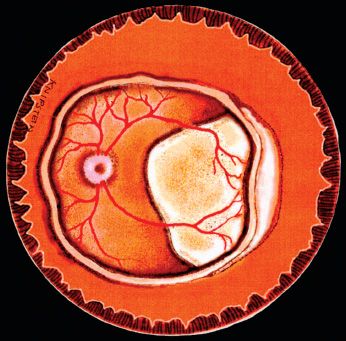
FIGURE 44.4 Artist’s drawing showing the predominantly effusive 4B retinal detachment of ROP extending from the ridge to include the center of the fovea. Subretinal fluid may be clear to turbid.
Predominantly tractional detachment (Fig. 44.5) is characterized by peaked retinal folds pulled toward the center of the eye. The retinal ridge may circumferentially contract and pull the retina toward the center of the eye. Frequently, prior to detachment, a central stalk and scaffolding of spokes extending to the retina become apparent. The network can be predominantly posterior when associated with regression of posterior hyaloid structures, predominantly anterior when associated with regressed structures of the tunica vasculosa lentis, or both. This tractional form of retinal detachment is common after laser treatment has reduced the vascularity, producing a “quiet” eye with less effusion into the subretinal space.
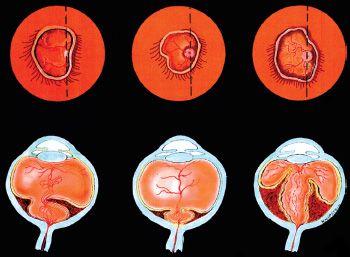
FIGURE 44.5 Artist’s drawing of a predominantly tractional 4B retinal detachment of ROP with asymmetrical traction by posterior cellular elements (hyaloid vasculature), the symmetrical traction by predominantly posterior cellular elements, and the configuration resulting by traction of predominantly anterior cellular elements (tunica vasculosa lentis). Upper row shows appearance with indirect ophthalmoscope. Lower row depicts cross-section of condition in upper row.
MECHANISM OF PREDOMINANTLY EFFUSIVE RETINAL DETACHMENT
Predominantly effusive 4B retinal detachment is believed to occur as a consequence of vascular leakage into the subretinal space. Sang et al. (17) observed vessels in the subretinal space of humans in a histologic study; however, the pathogenesis of the subretinal neovascularization is enigmatic. Okamoto et al. (18) developed a transgenic mouse model in which VEGF expression was linked to the rhodopsin promoter and observed intraretinal and subretinal neovascularization as a result of increased expression of VEGF in the outer retina. Although direct clinical evidence is lacking, this model supports the notion that VEGF expressed in the retina can lead to subretinal neovascularization, leakage of fluid into the subretinal space, and thus retinal detachment, characteristics clinically noted in the predominantly effusive form of stage 4B retinal detachment (Fig. 44.4).
MECHANISM OF PREDOMINANTLY TRACTIONAL RETINAL DETACHMENT
The predominantly tractional retinal detachment of ROP involves one of the most interesting features of retinal detachment evolution in the premature child’s eye. The involuting hyaloid system and tunica vasculosa lentis play an important role. Eyes with predominantly tractional retinal detachments generally develop sharply peaked retinal folds. These folds are attached to spokes connecting to the central stalk, best appreciated with endoillumination during vitreous surgery. The stalk always extends to the disc and can have other direct isolated strands connecting to the retina at or posterior to the ROP ridge. The anterior aspect of the stalk often connects to the posterior lens surface. In eyes with profoundly immature vascular architecture, as seen in some eyes with aggressive posterior retinopathy of prematurity, the retina may detach fatly as a consequence of diffuse hyaloidal contraction (19).
The traction generally has a dominant direction first toward the center of eye and then posterior toward the optic nerve or anteriorly toward the lens (Fig. 44.5). With progression from preterm through birth and thereafter, the vitreous organizes and the circumferential folds are often drawn centrally. Clear to turbid subretinal fluid can be present.
A possible scenario is outlined. An infant is examined a few weeks after premature birth during the period of slowed retinal vascular development and active apoptosis of the hyaloid system and tunica vasculosa lentis. At that time, only the hyaloid vessel or a few persistent vessels at the lens may be visible. The continued retinal ischemia from avascular retina drives an increase in angiogenic activity through increased VEGF action, with a reduction in apoptosis of the hyaloid endothelium resulting in clinically visible hyaloid vasculature and rubeosis iridis. In addition, an increase in proteolytic enzymes might release or activate growth factors within extracellular matrix that result in fibrosis. One possible candidate is TGF-β1, which aggravates the scarring process in fetal tissue and allows formation of hyaluronic acid. Increased concentration of hyaluronic acid in the secondary vitreous then would promote liquefied vitreous noted in eyes with late stages of ROP. This liquefied vitreous would provide less internal tamponade and allow the retina to be pushed forward from subretinal exudate or blood (effusive) or pulled (tractional) as RPE tries to resorb fluid. The increased scar tissue may account for the cicatricial phase seen in the classic “retrolental fibroplasia ” of late stage 5 ROP (Figs. 44.6 and 44.7). Surgical specimens of infant eyes operated on for ROP provide evidence for regressing vascular elements within the stalk likely from the hyaloid vasculature (Figs. 44.8 to 44.10).
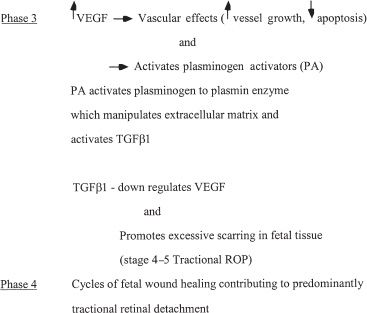
FIGURE 44.6 ROP tractional retinal detachment phases. Shown is the biochemical cycle leading to the cicatricial stage of ROP (4–5) predominantly tractional retinal detachment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


