FIGURE 40.1 Schematic representation of the SUNDROP hub-and-spoke RDFI screening program for ROP.
KIDROP RDFI Network in India
The Karnataka Internet Assisted Diagnosis of Retinopathy of Prematurity (KIDROP) program, initiated in the southern state of Karnataka in 2008, has expanded to provide ROP screening through an indigenously developed telemedicine platform that includes 54 neonatal care centers in 18 districts (3 zones of 6 districts each) utilizing 20 teams trained in RDFI ROP interpretation from throughout India. KIDROP uses a single RetCam Shuttle per zone. Dedicated teams of trained technicians transport the device between NICUs situated within rural and semiurban neonatal centers on a fixed schedule every week. Image capture, processing, storage, analysis, and reporting are performed on site by the technicians using a triage-based algorithm based on the principles of pattern recognition (Fig. 40.2). Images are also remotely viewed and reported on smartphones or personal computers by ROP experts from Bangalore, where KIDROP is headquartered, providing real-time diagnosis to the rural infants. The reports are transmitted to the rural technicians using the cellular network or the Internet via secure data server with a digital signature before the child can be handed over to the mother in most cases. Treatment is also provided at the rural center itself by the KIDROP team of experts or locally trained ophthalmologists.
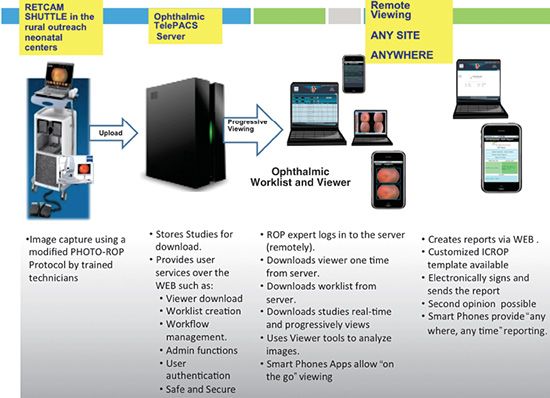
FIGURE 40.2 Schematic representation of the KIDROP program. Image capture, processing, storage, analysis, and reporting are performed on site by the technicians using a triage- based algorithm based on the principles of pattern recognition. ICROP—International Classification of Retinopathy of Prematurity.
KIDROP demonstrates the potential of coordinated public–private partnerships to expand access to care to prevent a worldwide leading cause of childhood blindness. The KIDROP screeners utilize an integrated RDFI platform employing automated binary compression, a patented technology to provide live, lossless image transfer and live reporting in conjunction with smartphone or tablets applications. Two unique features of the KIDROP program are the widespread implementation of nonphysician readers to grade and analyze the images as the first point of contact and the lack of any mandated BIO examination at any point to terminate screening. It remains to be seen if either of these innovations is effective (sensitivity and specificity) and generalizable to highly developed countries (United Nations Development Program Human Development Index) (82). Furthermore, particularly with respect to the US, use of nonphysician readers introduces medicolegal uncertainty (21,22). The challenges that face KIDROP are (i) barriers to adopt to new technology; (ii) lack of awareness of the disease even among the medical community; (iii) Internet speeds that are variable and often unreliable in the most backward areas, which hamper live image transfer; and (iv) relatively large capital costs of equipment during initiation of the program. Despite these issues, in the 5 years since inception, over 25,000 imaging sessions have been performed, over 6,500 unique infants have been enrolled, and the KIDROP program is now poised for a nationwide expansion in India.
IMPLEMENTATION OF AN RDFI SCREENING PROGRAM FOR ROP
Personnel
The RDFI team includes the RDFI reader/treater, the nurse photographers, the bedside nurse, the NICU team (physician, social work, nurse practitioners), the front desk schedulers, the legal consultants, the hospital administration, and the family members. Each group has a role to play to ensure a smooth transition from birth, identification of need for screening, screening, implementation of reader recommendations, discharge, hand-off and communication to outside screen, and completion of screening termination criteria. The easiest method for delineating roles is through the ROP screening contract. In addition to outlining each team member’s responsibilities, the contract can serve to head off disputes about what to do when a photographer is unavailable, when an infant needs treatment, when there is an equipment malfunction, and the like.
Photographic Technique
The photographic screening protocol most widely employed is derived from the PHOTO-ROP study (Fig. 40.3) using a RetCam (Fig. 40.4). Images are taken by nonphysician nurses or other trained personnel who have received training and, ideally, certification in the use of the camera and imaging technique (www.focusrop.com). Clarity Medical Systems, the manufacturer of the RetCam, offers 1 day of training with a certified ophthalmic photographer, infant mannequins, and live babies following purchase. Additionally, Clarity has an online training program (http://www.claritymsi.com/us/retcamtraining.html). In the SUNDROP program, the nurse photographers utilized both and then have additional annual training with the RDFI reader. Dilation is key to good photographs, and this can be achieved with phenylephrine 2.5% and tropicamide 1% every 5 minutes for three applications to each eye. Cyclomydril repeated once is a good alternative. Feedings should be held for at least an hour around an imaging session to reduce the risk of apnea, bradycardia, and aspiration. We recommend that the bedside nurse be present throughout the photographic session. A speculum is an absolute requirement, and the Alphonso speculum appears well suited for the 130-degree lens of the RetCam. We do not advocate for routine usage of scleral depressors. With respect to imaging frequency, RDFI images are most useful when there is a longitudinal record, and therefore, a screening frequency of at least weekly is most likely to ensure continuity of care, instill in the team members the importance of the enterprise, as well as capture rapidly advancing disease.
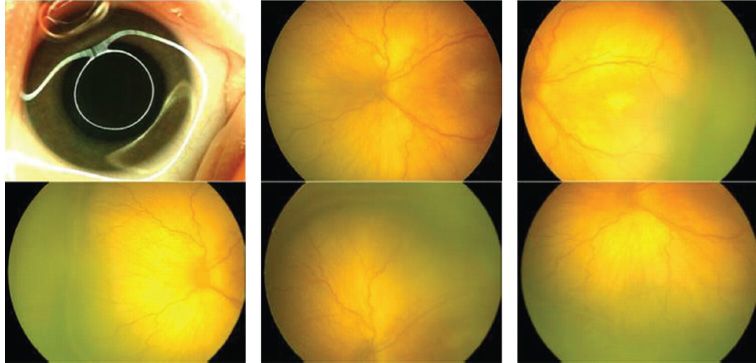
FIGURE 40.3 PHOTO-ROP standard image set for a left eye, consisting of an image of the iris, the optic disc, followed by images of the temporal, nasal, superior, and inferior retinal fields.

FIGURE 40.4 Image of the RetCam camera (Clarity Medical Systems, Inc. Pleasanton, CA).
Image Transfer and Storage
Once the six images for each eye have been obtained and assessed for quality and completeness, the images need to be transferred to the RDFI reader in an HIPAA-compliant fashion, using a file transfer protocol, automated synchronization with the server, or secure email.
To verify receipt, the RDFI reader should be notified independently via email, text, or phone message that images on X number of infants have been sent. With absent confirmation of receipt, the nurse photographer should contact the reader to verify and clarify. With the present camera, 12 images will occupy approximately 10 MB. These images need to be stored either with the reader on a secure server or locally with the camera or both. For larger networks, it will be economical to have redundant off-site storage, managed by the home institution’s information technology service or similar. Bear in mind that images may need to be stored until the infant reaches maturity (21 years of age), due to medicolegal concerns.
RDFI Report
The report of the images taken at each examination will become a permanent part of the medical record and require the following general documentation: name, medical record number, birth date, date of examination, date that images were received, date of interpretation, birth weight, gestational age at birth, postmenstrual age (PMA) at exam, weight at examination, number of images received, NICU, and the name of the interpreting physician. ROP characteristics that need to be documented on a per-eye basis are as follows: number of images, status of the iris/lens/pupil, vitreous clarity, zone, pre-plus or plus (number of quadrants), stage (number of hours), hemorrhages (by quadrant), and other abnormalities. The cornea, optic nerve, and foveal reflex can be documented. It is important to document the interval changes, if any. The report should include a summary of the interpretation, a recommendation as to future examinations or treatment, as well as an educational handout for the family members explaining to them the disease grading and recommendations (21). If the reader finds that the images are unacceptable for grading (poor quality, incomplete image set, artifact, mislabeling, etc.), then a request should be made to repeat the evaluation within 24 hours. Reports should be created and returned no later than 24 hours after receipt of images, unless other arrangements have been made in advance such as communicating the results in person or by phone. These reports serve many functions in addition to their medical support role, such as education of the NICU team, education of family members, creation of RDFI team solidarity, and use in Institutional Review Board (for human studies) approved studies.
RDFI Graders
While it is understood that every member of an RDFI team is interdependent upon each other and essential to its success, the RDFI grader holds a position akin to a quarterback on a football team. Even experienced ROP screeners may feel uncomfortable the first time they begin grading images. When SUNDROP was first deployed, the grader spent the first 6 months examining every patient with BIO prior to the photographs being obtained. Then he/she went home and interpreted each of the images, in essence mentoring him/himself. Presently, there are excellent mentoring opportunities in a live setting or through online certification courses (www.focusrop.com
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


