CHAPTER 4
Interaction with the Patient
THE INITIAL ENCOUNTER
The office is now prepared to receive allergy patients for diagnosis and treatment. The allergy area of the office has been set up, and the person who will be in charge of administering allergy tests and treatment, as well as rapidly becoming the allergy patient s sounding board, has been hired.
Certain changes in the office layout, subtle or otherwise, have been made to inform the patient that allergy care is now a part of the available treatment menu. Both the directing physician and the allergy caregiver have received appropriate training in allergy diagnosis and care. The patient now entering the office encounters a new aspect of care not previously available.
Some offices, reacting to the needs for increased efficiency in today’s medical market, have established a limited triage format in screening new patients. When a practice offers multiple aspects of care, this approach may facilitate saving time and avoiding delay for both patient and physician, although there may be shortcomings as a consequence. When an office uses this approach, the patient is initially seen by a physician’s assistant, a nurse, or other paramedical professional, who makes an initial evaluation of the nature of the problem and channels the patient along appropriate lines. This is especially effective when a group practice is involved in which not all members of the group are equally qualified and interested in all aspects of the field. This approach may become even more widespread in the future, but at present many practitioners feel that the physician is the best-qualified member of the group to make an initial decision regarding both the nature of the patient’s condition and the best approach to care, and therefore should serve as the first professional contact with the patient other than the office receptionist or the physician’s personal assistant. The directing physician, then, should be aware of the signs of allergy, and be prepared to factor this knowledge into diagnostic considerations and treatment plans. It is even more beneficial, to both the practice and the patients, if other members of the office staff are also alert to the indications of allergy. Some signs and symptoms of allergy may be observed even before the physician sees the patient.
Because many patients with allergy do not arrive at the office with this as their primary complaint, it is advantageous for most or all of the office staff to have some ability to recognize the allergic patient when first seen, even before a formal visit has been established. Because all the office personnel will eventually encounter and deal with the allergy patient, it is beneficial for all to recognize allergy, as this will aid them in understanding the various patient complaints that will appear over time. The allergy patient may be expected to have ongoing problems, and will usually be a frequent visitor. Identifying the allergic patient on first encounter, and frequently on first observation, adds to the staff’s recognition of the prevalence of allergy and often provides a feeling of personal knowledge and unique ability. In short, most staff members enjoy this silent exercise in diagnosis. When the presence of allergy has been recognized, and the treatment decision made, the patient is usually turned over to a special member of the staff with specific instructions on how to proceed.
RECOGNIZING THE ALLERGIC PATIENT
An overall look at findings that strongly suggest allergy should help alert the person making the initial contact with the patient, the member of the medical or paramedical staff observing the patient for the first time, and the person taking the initial history and performing the basic physical examination that there is a strong possibility of an allergic element being present. Because the ears, nose, and throat are the portals of entry for all allergens, and because four of the five senses are based predominantly in the ear, nose, and throat area, a major relationship would be expected and does in fact exist. Conditions that offend the senses drive the patient to the physician, often more rapidly than more dangerous conditions. This probably contributes to the frequency of physician visits for conditions caused by allergy.
PHYSICAL SIGNS OF ALLERGY
When the patient with allergy is first observed, certain physical signs are usually evident. This holds true especially for inhalant allergy, but also for food hypersensitivity. As noted, there is a considerable overlap between the two, and patients with inhalant allergy are more prone to food allergy than are basically nonallergic patients. At this point, it is not important that the cause of the allergy even be considered. The fact that the patient is allergic should be recognized, and in many cases this can even be seen or suspected when the patient is in the waiting room. The staff member first seeing the patient and those involved in performing the initial clinical evaluation should observe the patient for the following indications of allergy.
Facial Configuration
The look long known as adenoid fades may be equally as indicative of allergy (Fig. 4-1). The cheekbones tend to be less prominent, the nasal bridge is somewhat low, and the mouth tends to be slightly open. The mandible is frequently underdeveloped and the chin recessive. This is a developmental result of any condition that produces chronic nasal congestion and is not diagnostic of allergy, but it should raise an element of suspicion, especially if combined with other, more specific findings. This facial appearance alone is rather subtle and prone to be modified by genetic differences, but the person with this facial format, and a somewhat sad expression, may well be allergic.
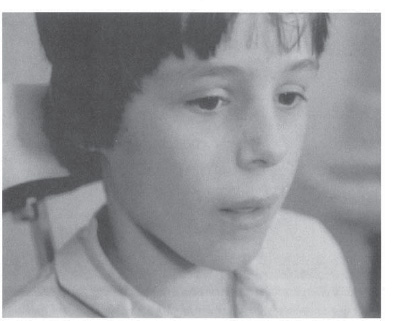
Figure 4-1 “Adenoid” faces: short chin, low malar peaks, open mouth, sad expression. (With permission from King HC. An Otolaryngologists Guide to Allergy. New York: Thieme Medical Publishers; 1990:61.)
Activity
The allergy patient is restless. In most cases, allergy of any type produces a constant annoyance. The allergic patient itches. In a child, the condition may be quite obvious, with the child squirming, twisting in the chair, and often moving about the room. This heightened activity is at odds with the rather sorrowful facial expression. In the adult, the condition may be less marked but is usually present in some form if watched for. This heightened activity is less obvious than the typical gestures of the allergic patient, but it may supplement other findings.
Gestures
Certain gestures are almost diagnostic of allergy. The most classic is the “allergic salute” (Fig. 4-2). This is most obvious in children. The allergic nose itches and is also congested. Placing the palm flat on the face and pushing upward lifts the flexible nasal tip off the congested turbinates, allowing a brief breath of air to enter the nasal cavity. At the same time, the itch is scratched to some degree. This gesture may be repeated several times in a period of a few minutes. If the allergic salute is kept up for two years or more, the supratip crease in the nose, a typical sign of allergy, develops. These findings are described later in this chapter (see Facial Stigmata), and when well established may be present throughout life.
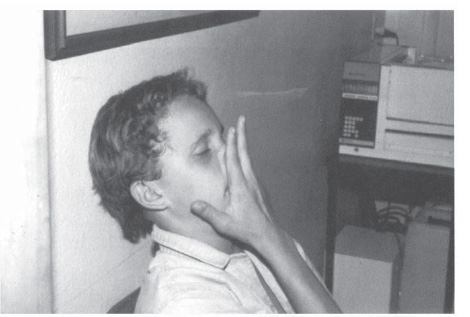
Figure 4-2 The allergic salute: the gesture both rubs the itching nose and lifts the nasal tip enough to allow a momentary breath of air to pass above the congested turbinates. (With permission from King HC. An Otolaryngologist’s Guide to Allergy. New York: Thieme Medical Publishers; 1990:58.)
As the child ages, social pressures make the allergic salute less acceptable. The physical sensations producing the salute continue, however. In most cases, the salute is replaced by grimacing: twisting the upper lip and midface to move the nasal tip (Fig. 4-3). This may also be unacceptable, inspiring the impression that the patient is “making faces,” but is almost unavoidable. It is interesting to quietly observe patients in a waiting room and note the number of adults surreptitiously grimacing to wiggle the nasal tip. This has been referred to as the “bunny rabbit” motion, and the term is singularly appropriate.
One final activity that may be noticed is “clucking.” Even in a moderately noisy room, this sound can sometimes be heard, and it becomes quite obvious in quiet surroundings. The allergic palate itches, and the patient soothes the itch by rubbing the tongue over the area. This action produces a pronounced “cluck,” which may vary in volume depending on the age of the patient. It is an action that is often especially annoying to a parent.
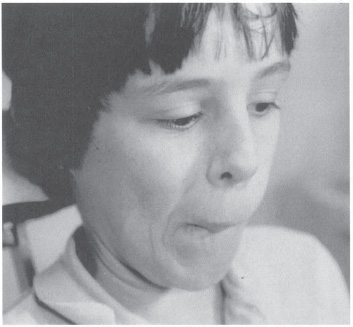
Figure 4-3 The allergic grimace: twisting the face replaces the allergic salute. (With permission from KingHC. An Otolaryngologists Guide to Allergy. New York: Thieme Medical Publishers; 1990:60.)
Facial Stigmata
Although the previous gestures may be easily seen by an alert observer who has a good view of the waiting room, in most cases the first view of the patient is obtained when the patient is in the examining room. At this point, the person making the initial clinical contact, be it the clinician, a nurse, physician’s assistant, or other, has the opportunity to see the patient at fairly close hand. Certain facial appearances typical of the allergic patient immediately stand out.
ALLERGIC SHINERS
Probably the most outstanding feature of the allergic patient’s face is the presence of dark staining below the lower eyelids (Fig. 4-4). This may appear in the very young patient, even in the toddler, and continue to be present throughout life. If the allergy is untreated, the discoloration may become permanent.
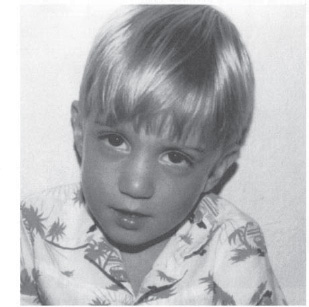
Figure 4-4 Allergic shiners: dark discoloration of the orbit resulting from venous stasis due to chronic nasal congestion. (With permission from King HC. An Otolaryngologists Guide to Allergy. New York: Thieme Medical Publishers; 1990:57.)
DENNIE-MORGAN LINES
Dennie-Morgan lines, or Dennies lines (Fig. 4-5), are crescentic creases in the skin of the lower eyelid. These, like the allergic shiners, appear very early in life, and the two are usually present together.
Both allergic shiners and Dennies lines are the result of stagnation of venous blood in the orbital region. Venous drainage from the orbit begins in the marginal venous arcades and progresses through the angular veins, medial palpebral veins, inferior ophthalmic veins, and on into the sphenopalatine veins and the pterygoid plexus (Fig. 4-6). Congestion in the nose and paranasal sinuses results in pressure on the anterior complex of this group of veins, which run beneath the nasal and sinus mucosa. This in turn causes venous blood to back up in the orbit, resulting in darkening of the overlying tissue and eventually permanent staining of the skin caused by leakage of hemosiderin. In addition, the stagnating blood and resultant local hypoxia produce spasm in the unstriated muscle of Muller in the lower eyelid. This muscle is attached to the skin, and the spasm results in the formation of creases in the skin that, like the discoloration, may well become permanent.
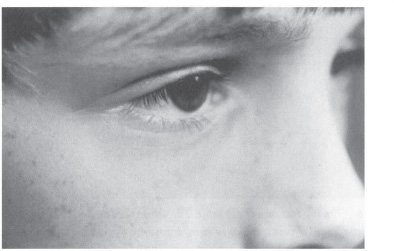
Figure 4-5 Dennie-Morgan lines: skin lines in the lower eyelid resulting from poor oxygenation of the unstriated muscle of Muller. This is the result of venous stasis in the orbit caused by chronic nasal congestion. Note also the long, irregular silky eyelashes typical of allergy. (With permission from King HC. An Otolaryngologists Guide to Allergy. New York: Thieme Medical Publishers; 1990:57.)
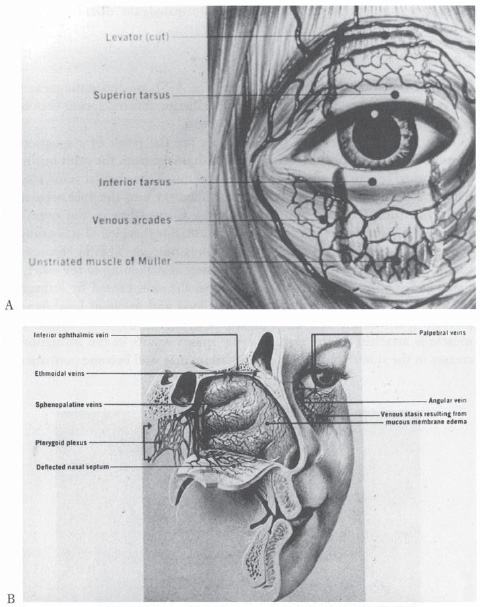
Figure 4-6 Venous drainage of the orbit. The orbit is drained via venous arcades into the palpebral and angular veins, which in turn drain into the sphenopalatine plexus. Congestion in the nasal mucosa produces venous stasis in the orbit, resulting in allergic “shiners” and prolonged spasm of the unstriated muscle ofMuller in the lower eyelid, producing Den-nie-Morgan lines in the lower eyelid. (Courtesy of Pfizer Inc., Kalamazoo, Michigan, Scopes Publications, “Stigmata of Inhalant Allergy.”)
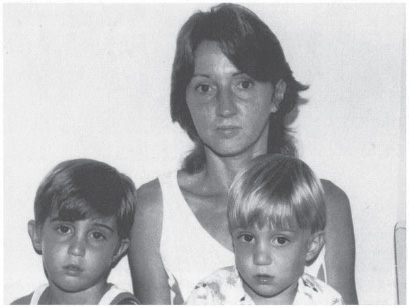
Figure 4-7 Familial allergy. A mother and two sons exhibiting similar allergic shiners and the typical facial signs of allergy. (With permission from King HC. An Otolaryngologists Guide to Allergy. New York: Thieme Medical Publishers; 1990:54.)
If the patient is a child and has been brought in by a parent, especially if a sibling is also present, it is interesting to observe the entire group. Allergy is a familial disease, and it is not unusual to see the same facial stigmata reflected in all members of the family (Fig. 4-7).
Supratip Crease
This finding requires a little closer observation than those previously mentioned, but it is seen about as frequently. It does not appear as early in life as do the allergic shiners and Dennie’s lines. It is represented by a clear crease in the skin of the nose between the mobile nasal tip and the more stable pyramid above (Fig. 4-8). The development of this crease requires about two years of repeated performance of the allergic salute at close intervals. When well established, the supratip crease may be extremely difficult to eradicate. Even during rhinoplasty, when access to the underside of the skin is available, extensive scoring of the skin may fail to eliminate the crease entirely. This crease is frequently quite annoying to teenagers, as it is often the nidus for unsightly pimples and blackheads.
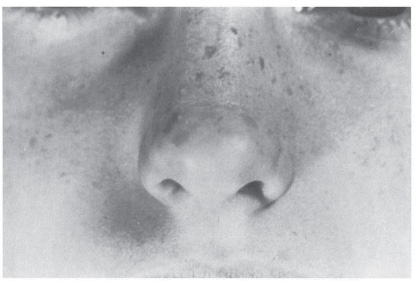
Figure 4-8 The supratip crease: repeated use of the allergic salute for 2 years or longer may result in permanent creasing of the skin above the nasal tip. This may persist throughout life. (Courtesy of Pfizer, Inc., Kalamazoo, Michigan, Scopes Publications, “Stigmata of Inhalant Allergy.”)
Crusting and Rawness in the Nostril Area
Excoriation in this area is primarily seen in children, and is by no means always present. When it does occur, however, it presents strong confirmation of an ongoing allergic condition. The allergic child has a chronically runny nose. This is a matter of degree. All children may be expected to have some degree of nasal drainage, more than is present in an adult. A normal adult nose produces between 1 and 3 L of mucus in a single day, and this amount may be increased by allergy. A child is born with all the mucous glands the nose will ever have, confined in a considerably smaller structure than the adult nose. More mucous drainage from the nose than will occur in adult life is quite normal, despite the mother’s concern, and few children are well enough motivated or trained to concern themselves with the social implications of a mucusladen nose. When the drainage is clear, it is not indicative of infection. However, when the drainage becomes markedly exaggerated and constant, as occurs in allergy, the area of the upper lip immediately below the nose and the nostril margins may become chronically irritated (Fig. 4-9). When present, this finding is strongly indicative of an ongoing allergic problem, even though allergic activity at the moment of examination may not be acute.
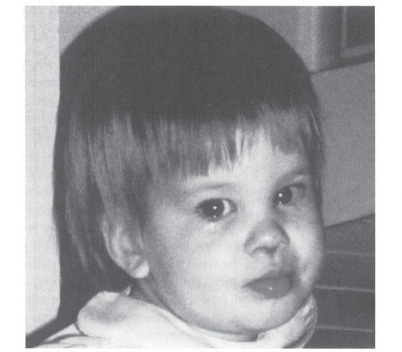
Figure 4-9 Allergic child with chronic nasal crusting from profuse rhinorrhea (in this case, caused by a food allergy to corn).
The previously mentioned features of facial appearance may be seen by an alert observer before a more complete physical examination is performed. When present, they should provide a strong indication of allergy and place this diagnosis under consideration. The directing physician may now elect to perform a more detailed history personally, or delegate this part of the procedure to the person designated as the regular allergy caregiver.
INITIAL ALLERGIC HISTORY
The single most important aspect in allergy diagnosis, and in ongoing allergy care, is the allergic history. The physical examination is of importance in further identifying the presence of allergy and in eliminating other conditions, such as structural defects, but it is the history that usually establishes the overall condition, indicates the nature of the exposure, and leads to a suspicion of specific offenders. The restrictions placed by third-party payers on avoiding the extensive use of laboratory testing has made the history an even more important part of the diagnostic approach. The clinician practicing allergy is expected to have a broad understanding of the condition, and to use this knowledge to direct the studies necessary and not test at random.
It is an axiom of allergy that the history is never taken as a single entity or at a single sitting. The patient’s memory is frequently undependable in regard to seasons and exposures, especially when an adequate amount of time has not been allowed to give these matters thought. Many patients have not considered allergy as a significant part of a presenting problem at the time of their initial visit, and they are too surprised by the proposed diagnosis to recall details reliably. Often, a better background picture is provided by family and associates than by the patient, as many patients who have been allergic for years consider this condition to be a normal state. Only when a complication occurs, or they are pressed by family or associates, do they seek medical care. A detailed background history cannot be expected at this point. The patient must be made aware of the type of symptoms and the pattern of onset and remission that will aid the physician in making a diagnosis, of both the basic nature of the disease and probable offenders. Because allergy is frequently not a dramatic condition, the events producing symptoms may not be at all obvious to patients until they have been made aware of the information necessary to provide a diagnosis, and have given considerable time and thought to the answers.
A large number of factors influence the allergic pattern demonstrated by a patient, including season, age, exposure, environment, and intercurrent disease. The more of these factors that can be identified, the better the results that may be expected from treatment. No matter how dedicated the person taking the history may be, it is impossible to obtain complete information covering all possibilities during a single session, especially with the time constraints necessary in the average practice. Time is not normally allotted for an extensive history when the condition has not been identified. Nonetheless, certain aspects of history must be obtained and evaluated as early as possible to determine the direction further study and care should take.
No routine format can be presented for this evaluation, but certain approaches may serve as a guide to both the physician performing the initial evaluation and the designated allergy caregiver, who will enlarge the history. The information obtained may also affect the steps to be followed in confirming the proposed diagnosis and instituting care. These two parts of the basic allergy history are not usually taken at the same time. This division in history taking allows different approaches on the part of the directing physician and the ongoing caregiver, which may be used to facilitate and streamline the overall evaluation.
History by the Physician
The first person to encounter the patient on a medical basis and to hear the patient’s history is usually the treating physician. On occasion, because of the pressures of managed care to streamline practices, the first person encountering the patient may be a nurse or physician’s assistant. When this is the case, however, the person selected for this important task should be highly competent and familiar with the technique of obtaining a history that will include consideration of allergy as a primary or contributory cause of the patient’s symptoms.
Allergy should be considered on the basis of the initial complaint and initial physical observations, and the possibility should be weighed that this condition may be a major contributor to the complaint. The major limitation for this examiner is time. When the patient s initial visit is scheduled, it is not known whether allergy will be the primary or at least a significant part of the complaint, and an insufficient amount of time may have been allotted for evaluation of the patient with so complex a problem. The patient must be accommodated if good care and a satisfactory ongoing relationship are going to be established, but at the same time an excessive amount of time cannot be spent with the allergy patient without delaying other patients unnecessarily. Adjusting to this dilemma is essential if the directing physician is to provide all aspects of care in an appropriate manner. As the physician (and other members of the allergy team) come to understand more about the disorder, less time is required to obtain essential information from patients with possible allergy.
It must be recognized when considering allergy that the history is the most essential aspect of the initial evaluation. A detailed history is not necessary, however, to determine the direction needed to pursue an appropriate course of diagnosis and treatment. The physician involved in initial contact with the patient must determine certain critical factors indicating the presence of allergy and, in an overall way, the nature of the probable offenders. There are many possible routes to clarify this diagnosis, but one pattern of questions usually provides the necessary information to direct the next step in diagnosis and treatment. Certain questions tend to go to the heart of the problem and allow the physician to feel relatively confident in the preliminary diagnosis. It should then be realistic to proceed with a more extensive diagnostic history and appropriate definitive tests.
SYMPTOMS
The classic opening question, “What brings you here?” is as good an initial approach as any. The patient then presents the primary complaint, which may have nothing to do with allergy, and, if so, may be treated on its own merits. If, however, the primary complaint suggests a good possibility of an underlying allergic condition, the physician may then explore this possibility with questions directed specifically to allergy. Taking this part of the history competently requires broad knowledge of the problems that allergy can cause. Most of the more common problems have been enumerated in the preceding pages. Unfortunately, the complete list is almost endless and is complicated by the fact that other conditions may mimic allergy in much the same way that allergy mimics other conditions. Certain factors, however, tend to suggest allergy.
ONSET
“When did the problem start?” Although the tendency to allergy is genetically determined, it is rare to see inhalant allergy appear in infancy. (Food hypersensitivity is a different situation, and is discussed independently.) It is also rare to see true allergy appear in the geriatric patient as a new condition. Provided the environmental situation is stable (i.e., the patient has not made a major geographic move or been exposed to new potential offenders), inhalant allergy may begin to appear around the age of 2 or 3 and increase from that time to about the age of 30, when it usually peaks. The condition then tends to remain stable or decrease gradually into the 60s, at which time there is sometimes a small peak followed by a decline in sensitivity. Although many patients feel that such a situation has occurred, it is rare to have an elderly patient experience the onset of allergy after the usual retirement age. This is not impossible if the patient has coupled retirement with a major environmental change, but the possibility should be considered with caution. This situation would be an appropriate one for a limited inhalant allergy screen, largely to clarify the situation and satisfy the patient.
FLUCTUATION
“Is the condition constant, or does it change from time to time?” This can be a key indicator. If the condition is unchanged from season to season and from one location to another, it suggests perennial allergy, mediated either by mites, molds, or epidermals to which the patient is constantly exposed, or by foods that the patient eats regularly. As discussed in the chapter on foods, most people are habit-driven eaters and consume the same foods day after day. The form may vary, but the basic food is the same. This may apply even during travel if the patient is able to select all the foods eaten. If the symptoms change radically during travel, however, an investigation of the inhalant allergens in the various areas needs to be undertaken, and if these are not different from those at home, the food pattern warrants evaluation.
If a definite symptom change is seen from one season to another, the indication is strong that the patient has an inhalant allergy. Pollens have definite blooming seasons, as described in the section on selection of antigen for therapy in Chapter 3. For the patient in whom inhalant allergies are developing, it is not unusual to see symptoms appear in the early stages in only one or two seasons and then escalate during succeeding years until eventually they become a perennial problem. This pattern typifies an allergic pattern that usually responds well to immunotherapy.
EXPOSURE
“Has anything changed in your environment?” This general question must usually be expanded on. By this point, however, time is growing short for an initial evaluation, so the patient must usually be prompted to bring forth significant changes without enumerating every possibility. Has the patient moved to this geographic area relatively recently? The move does not have to precede immediately the appearance of symptoms. It usually takes months or years for allergic symptoms to develop after the initial contact and continued exposure occur. Has there been a change of job or of workplace? Has the home been changed or redecorated? Have any new pets been brought into the home? Has the patient started any new medications or radical changes of diet? These last factors are often neglected, as both physician and patient are now thinking about environmental exposures.
FAMILY HISTORY
“Does anyone in your family have allergies?” Allergy is a familial disease. It has already been noted that superficial allergic stigmata often appear in many family members. When inquiring about a family history of allergy, the physician should be sure to investigate the common euphemisms for allergy, such as hay fever, catarrh, sinus, and bronchial conditions.
PREVIOUS ALLERGY TESTS
“Have you ever been tested for allergy?” This question is the least likely to produce a positive answer, but if the patient has been tested and the form of testing is known to be reliable, much may be learned. If the testing has been performed in the same geographic area in which the patient now resides and performed during adulthood, a totally negative or a strongly positive result of testing supports or makes less likely the presumptive diagnosis of allergy Confirmatory tests are indicated, but the pattern of testing may be based to some degree on previous results with a considerable saving in time and procedure. It is well to realize that a “negative” prick test for inhalant allergens may be seen in patients with only mild degrees of hypersensitivity, yet such patients may exhibit significant allergic symptoms and benefit from appropriate therapy. These situations require intradermal dilutional testing (IDT) or quantitative in vitro testing for diagnosis.
These questions and their answers usually fill the time available during the initial visit and direct the ensuing history taking along the most productive lines. A more detailed history is necessary, as is discussed later in this chapter, but this is usually taken after the complete physical examination for allergy has been accomplished, and it may not always be taken by the directing physician.
FINDINGS ON PHYSICAL EXAMINATION
The previously noted items of facial appearance may be seen by any observer before a complete physical examination is performed. Such findings should alert the observer to the presence of allergy and indicate the potential benefit to be expected with appropriate treatment. Because of the constraints of modern medical practice, with cost control a major concern, a good history and physical examination must replace or reduce the use of random, and at times excessive, laboratory testing. The main thrust of this section is the physical examination, after which a more complete history is needed to establish the relevance of the physical findings, avoid misinterpretation, and set the stage for appropriate treatment planning. At this stage, however, a step-by-step progression through a complete ear, nose, and throat examination is required, with emphasis on findings that potentially indicate allergy.
Eyes
The eyes may show signs of allergy (e.g., edema of the conjunctivae, increased tearing, and vascularity) without nasal symptoms beyond the usual “hay fever” season. The presence of Dennie-Morgan lines and allergic shiners have already been described. A typical finding on the allergic eye is long silky eyelashes of uneven length (for reasons which are unknown). This produces a very attractive eye appearance; however, the possible indication of allergy should not be ignored (Fig. 4-10).
In addition to these findings, the eye itself frequently shows typical allergic stigmata. The conjunctivitis seen with hay fever is easily recognized. Tearing and itching are profuse, and the patient feels miserable. Less easily identified is the edema that may affect the cornea, making wearing contact lenses difficult. Questioning at this point often elicits a history of excess ocular itching that was not originally mentioned.
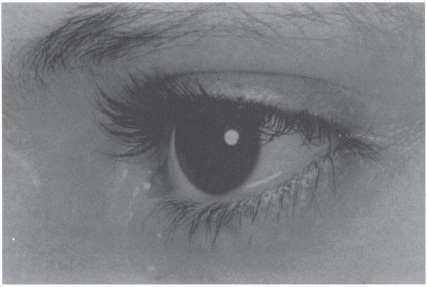
Figure 4-10 Allergic child, demonstrating frequent finding of long, silky eyelashes. (Courtesy of Pfizer, Inc., Kalamazoo, Michigan, Scopes Publications. Marks M. Stigmata of Respiratory Allergies. With permission from Marks M. Stigmata of Respiratory Tract Allergy. Kalamazoo, Michigan: Upjohn; 1977.)



