ROP, retinopathy of prematurity.
In 2005, data from 17,400 blind children from 38 countries were reviewed (11) and provided supporting evidence that the third epidemic of blindness due to ROP principally affected the middle-income countries of Latin America and the former socialist economies (12). In these studies, the proportion of blindness attributed to ROP ranged from 0% in all the studies from Africa—apart from South Africa—to 60% in a study from one province in Argentina. Countries were characterized and grouped using United Nations Development Programme (UNDP) measures of development (the Human Development Index) (13) as highly developed (rank 1 to 30), moderately developed (rank 31 to 100), and poorly developed (ranked 101 and above). The findings showed that the proportion of children who were blind from ROP was higher in countries ranked as moderately developed (24% overall, range 0% to 60%) than from those that were highly developed (9% overall, range 3% to 13%) and from those that were poorly developed, where only Guatemala and South Africa recorded any blind ROP children (4% and 10.6%, respectively). Since then, data on 17,551 blind children have been reported, giving additional data on ROP as a cause of blindness in children. The findings are similar to those reported in 2005 (Table 35.2). There are two outlier countries, Hong Kong and Vietnam, which both have a higher proportion of blindness from ROP than would be expected. In the case of Vietnam, this appears related to the very rapid improvement in socioeconomic development the country has recently experienced.
TABLE 35.2
Proportion of blindness in children due to retinopathy of prematurity in countries ranked by the UNDP Human Development Index ranking (2009)
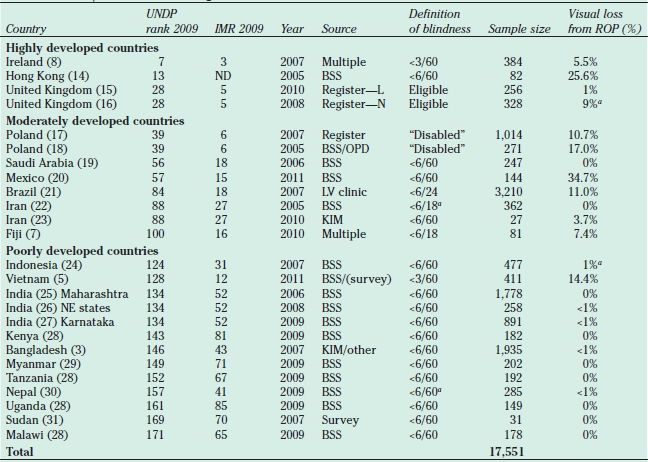
aIncludes other perinatal causes, unspecified.
BSS, blind school study; OPD, Out-patient Department; LV, low vision; KIM, key informant method; register—L, local register; register—N, national register; UNDP, United Nations Development Programme.
ROP, retinopathy of prematurity; IMR, infant mortality rate.
Under-5 mortality rates have been used as a proxy indicator to predict the prevalence of blindness in children (32), and it has been suggested that infant mortality rates (IMRs) could be used to predict whether blindness due to ROP is likely or not (12). The data suggest that countries with low IMRs (i.e., ≤9/1,000 live births) have a low risk of ROP blindness. This is because in these settings neonatal care services are well developed and of high quality, and efficient and effective programs to detect and treat ROP are in place. At the other end of the socioeconomic spectrum, countries with IMRs >60/1,000 live births are also not likely to have ROP as an important cause of blindness, but for totally different reasons. In these countries, neonatal intensive care is not well established, being confined to a few units in major cities, and so the majority of preterm babies do not survive. It is the middle-ranking countries with IMRs in the range 10 to 60/1,000 live births where ROP is, or is likely to be, an important cause of blindness in children. There are several reasons why ROP is a public health problem in these countries. First, rates of premature birth are higher on account of high rates of teenage pregnancy (33), poor attendance at antenatal care facilities, poorly regulated assisted fertilization with multiple births (34), and, in some regions, very high rates of elective cesarean section (35). Second, interventions known to reduce the risk of ROP are not always being implemented, for example, antenatal steroids and close monitoring of supplemental oxygen. Last, not all neonatal units have programs for examining and treating babies at risk of severe ROP. The more recent data in Table 35.2 confirm that IMR may be a good proxy indicator for the risk of blindness due to ROP. Few data are available on the causes of blindness in children from countries in the Middle East and North Africa, but given their health indices (e.g., IMRs in the range 10 to 60/1,000 live births), one would expect ROP to be responsible for a relatively high proportion of blindness in children.
Change in Blindness Due to ROP Over Time
Several papers have analyzed data on the causes of blindness in children by age group, to assess whether there is a trend in the major causes over time. Data from a large city in Mexico (20) and a national study undertaken in Vietnam (5) showed a far higher proportion of younger children to be blind from ROP compared with older children; for example, in Vietnam, 32.6% (42/129) of children aged <10 years were blind from ROP compared with only 6% (17/282) of older children. Comparable figures for Mexico were 43.3% (25/59) among children aged 0 to 15 years and 18.8% (6/32) among older children, suggesting that the problem may be increasing over time in these two countries. However, blind school studies are subject to selection bias, and for the age group comparison to be valid, several assumptions are needed, for example, that the majority of children become blind before the age of 5 years and that mortality rates among children who are blind are the same regardless of cause, the latter being unlikely. A study of children registered visually disabled in Poland has demonstrated the opposite trend that the proportion of children newly registered as blind due to ROP was slightly lower in those registered between 1999 and 2004 than those between 1974 and 1998, that is, 10.7% and 14.1%, respectively. This change may, in part, reflect the fact that Poland’s Human Development Index has improved from 0.73 in 1995 to 0.81 in 2011, and IMRs have fallen from 14/1,000 live births in 1994 to 5/1,000 live births in 2010 (36).
The United Nations Millennium Development Goals (36) have as one target the reduction in child mortality. Over the last few years, governments and agencies across the world have greatly increased programs and interventions to reduce child mortality and have had very positive results in virtually all regions. As preterm birth contributes significantly to neonatal mortality, and hence child mortality (37), many countries are increasing provision for preterm babies. This is particularly the case in China (38), India (39), and the other emerging economies in Asia, and it seems likely that ROP will become an increasing challenge in these countries as a consequence.
Rates of ROP Needing Treatment
Data on rates of ROP needing treatment are difficult to compare, as the case mix varies widely between and among studies (e.g., by BW and GA, by ethnicity, the proportion who are small for gestational age), and different indications for treatment have been used (e.g., at threshold according to cryotherapy for retinopathy of prematurity [CRYO-ROP] indications (40) or type 1 ROP according to the Early Treatment of ROP study) (41) (Table 35.3). The service providers also vary, as some data are reported from government units in the university or municipal or federal health system, and many different ophthalmologists are involved in examining the infants. Nonetheless, the data do seem to suggest that rates of ROP needing treatment are often high, particularly considering the wide screening criteria used in many of these studies. Aggressive posterior ROP (42) was also a frequent indication for treatment (43–45).
TABLE 35.3
Rates of ROP, by country
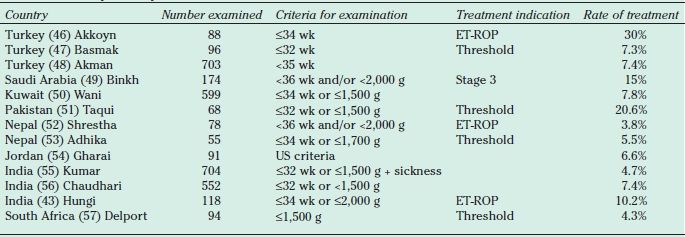
ROP, retinopathy of prematurity; ET-ROP, early treatment for retinopathy of prematurity.
POPULATION AT RISK OF ROP NEEDING TREATMENT
Since the first reports of blindness due to ROP in middle-income countries (10,11), many papers have since been published on the BW and GA of babies who developed severe ROP (i.e., that warranted treatment using either CRYO-ROP or early treatment for retinopathy of prematurity [ET-ROP] indications) from Argentina (58), Turkey (47,48), Jordan (54), India (59–62), Saudi Arabia (49), Vietnam (63,64), Romania (65), China (66–70), and Latin American countries (44,71,72). Compared to industrialized countries, in these settings, bigger, more mature babies were found to develop severe ROP. This is shown schematically in Figure 35.1. However, this is not the case in all reports, suggesting that high-quality neonatal care can be achieved and that severe ROP in larger, more mature babies can be prevented (73).
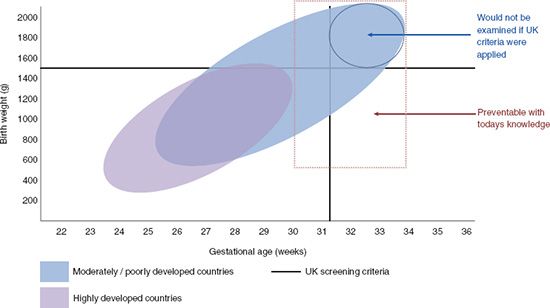
FIGURE 35.1 Diagram of characteristics of babies with severe ROP in highly developed countries and in moderate and poorly developed countries.
Risk Factors for ROP
In middle- and low-income countries, risk factor studies show that prolonged exposure to oxygen (53,68,70,74), respiratory distress syndrome (46,51,55), and sepsis (67) can be independent risk factors for ROP in addition to measures of prematurity. However, very few papers report the proportion of infants whose mothers were given antenatal steroids within 48 hours of birth, a treatment reported to protect against ROP (75). Recent renewed interest in optimum oxygen saturation levels to prevent ROP (76,77) has led to several observational studies as well as clinical trials (78–80). The SUPPORT trial, the first clinical trial to report outcomes to compare lower versus higher target oxygen saturation levels, showed that lower target saturations were associated with a reduced risk of ROP and bronchopulmonary dysplasia, but concern has been raised as lower target saturations were also associated with increased mortality (81). A recent meta-analysis of the results of recent trials and observational studies concludes: “Until more data become available, oxygen saturation (SpO2) in immature babies should not be targeted at low levels, between 85% and 89%. The optimal SpO2 is presently not known” (82). A further meta-analysis is planned when the results of ongoing clinical trials become available (83), which is hoped to provide clear guidance as to what constitutes safe oxygen saturations, which may need to vary by gestational age and postnatal age.
The finding that more mature babies are developing severe ROP than is generally the case in industrialized countries suggests that much can be done with the present knowledge to prevent ROP in these settings. A recent important study by Chen indicates that control should not focus on individual risk factors (84), because his study demonstrates that risk factors for ROP interact with each other; that is, oxygen exposure was a more important risk factor in extremely preterm infants, whereas sepsis was more important in more mature infants. The implications of this study are that all aspects of neonatal care need to be of high quality to prevent severe ROP. In terms of control of specific risk factors, a recent observational study from Argentina has reported lower rates of ROP needing treatment following use of lower target oxygen saturations (85), and a preliminary study from Peru suggests that severe ROP has declined since workshops were held for neonatal staff focusing on how to improve delivery and monitoring of oxygen (72).
In public health terms, it is important to go beyond the specific risk factors individual babies are exposed to (e.g., sepsis) and to try and understand the underlying causes. What is clear is that neonatal units in middle-income countries are often overcrowded and underresourced. In Latin American countries, much of the nursing is provided by auxiliary nurses who have usually had minimal initial training or continuing professional development, and one nurse may be responsible for the care of many more high-risk infants than would be acceptable in industrialized countries. Studies in Brazil (44), South Africa (86), Mexico (87), and Colombia (88) show that there is also often inadequate equipment for safe delivery and monitoring of oxygen. Recent studies in India (89) and Pakistan (90) have also shown that levels of knowledge about ROP among medical and nursing staff are often low. It is important to recognize that the variability of resources, training, and the ability to regulate oxygen and deliver care in different regions throughout the world make it necessary to only compare treatments and outcomes from infants within a certain region and under similar conditions and not between regions, such as between Latin America and the United States.
IMPLICATIONS FOR PROGRAMS IN MIDDLE- AND LOW-INCOME COUNTRIES
Many industrialized countries have clear guidelines indicating which preterm babies should be examined for ROP in order to detect those needing treatment (91,92). However, these guidelines cannot be applied universally—if they were, many infants at risk of severe ROP would not be included (Fig. 35.1). Authors of many of the studies quoted above, and others, have suggested that wider criteria are required, with one author suggesting criteria of ≤34 weeks or ≤2,000 g (65). However, given the wide variability in the quality of neonatal care in middle- and low-income settings, other parameters may play a role in refining criteria, to avoid unnecessary examinations. For example, a study in seven units in Rio de Janeiro, Brazil, showed that mortality rates in babies with BWs <1,500 g may assist in distinguishing which units require wider criteria (i.e., those with higher mortality rates) (93).
Widening the criteria will, however, dramatically increase the number of babies needing to be examined and increase the workload of ophthalmologists and staff in the neonatal unit. However, the workload implications may not be as high as anticipated, because a high proportion of more mature babies will only need one examination, usually while they are still in the neonatal unit (44).
Another implication of wider criteria is that the more mature babies are likely to have been discharged from the neonatal unit before the treatable stages develop (85). This has important implications for those managing programs as well as for families, particularly for those who are poor. In situations where neonatal care is limited to major cities, families may live very far away, and the cost of travel and accommodation for follow-up examinations may be prohibitive. Indeed, in a study in India of babies who presented to a tertiary referral unit with stage 5 disease, failure to attend for follow-up examinations was reported as a cause of disease progression. If wider criteria are used, more intensive counseling of parents will be needed, systems for recall put in place (e.g., using mobile phones), and, if necessary, costs for travel reimbursed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


