FIGURE 34.1 Mean distribution of ROP diagnoses by seven retinal fellows. A: Among the 28 eyes with a reference standard diagnosis of type 2 prethreshold ROP, the 7 fellows diagnosed type 2 prethreshold ROP in 5 (17%) eyes. B: Among the 15 eyes with a reference standard diagnosis of treatment-requiring ROP, the 7 fellows diagnosed treatment-requiring ROP in 14 (91%) eyes. (Reprinted from Chan RVP, Williams SL, Yonekawa Y, et al. Accuracy of retinopathy of prematurity diagnosis by retinal fellows. Retina 2010;30(6):958–965.)

FIGURE 34.2 Example of study images frequently misdiagnosed by fellows. A: Nasal, (B) posterior, and (C) temporal images diagnosed as type 2 ROP by the expert reference standard and no ROP by two of five fellows (40%), mild ROP by one of five fellows (20%), type 2 by one of five fellows (20%), and treatment-requiring by one of five fellows (20%). (Reprinted from Myung JS, Chan RVP, Espiritu MJ, et al. Accuracy of retinopathy of prematurity image-based diagnosis by pediatric ophthalmology fellows: implications for training. J AAPOS 2011;15(6):573–578.)
In an effort to further explore this issue, two web-based surveys of training programs in the United States have characterized trends in ROP education. In a survey of ophthalmology residents and residency program directors, Nagiel et al. (21) showed that two-thirds of responders estimated that residents performed <20 ROP examinations during their entire residency training. Also, despite over 80% of resident responders reporting they were not confident in their examination skills, about one-third of resident examinations lacked supervision by an attending at the bedside. A separate study of pediatric ophthalmology and retina fellowship training programs also showed concerning trends (22). Results demonstrated that from almost 30% of respondents up to two-thirds of ROP examinations performed by fellows were not followed up by an attending. Therefore, there were a significant number of infants who were examined exclusively by a trainee. Additionally, there was great variability in the number of ROP examinations performed by fellows across programs, and pediatric ophthalmology fellows performed significantly fewer laser photocoagulation procedures than retina fellows (Fig. 34.3). Lastly, only 7% of respondents reported the use of formal evaluations to assess fellow competency in ROP management. The survey data therefore showed the following: (i) a limited exposure to ROP in ophthalmology residency; (ii) lack of direct attending supervision during ophthalmology residency and fellowship ROP training; and (iii) extremely varied ROP curricula and experience across fellowship programs.
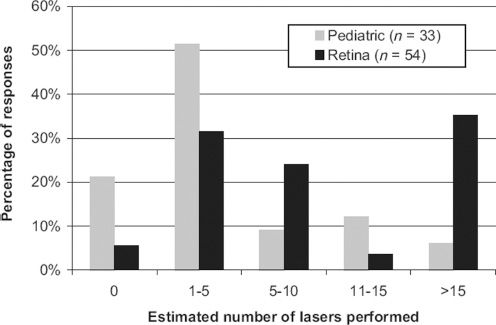
FIGURE 34.3 Attending and fellow responses to number of ROP laser photocoagulation procedures performed by fellows during the course of their training, stratified by specialty. (Reprinted from Wong RK, Ventura CV, Espiritu MJ, et al. Training fellows for retinopathy of prematurity care: a web-based survey. J AAPOS 2012;16(2):177–181.)
The study results revealed possible areas of refinement in ROP education: increasing ROP exposure during ophthalmology residency may be beneficial; having a more robust experience in residency may not only inspire more physicians to later consider incorporating ROP into their future practice, but it would also better prepare those that actually pursue subspecialty training in pediatric ophthalmology or retina; and a greater emphasis should be placed on attending supervision of trainee ROP examinations at the bedside. As the data demonstrated, currently many trainee ROP examinations occur without attending supervision. Having multiple, separate examinations may increase stress on already sick infants as well as present logistical challenges with respect to scheduling repeated dilated exams in the neonatal intensive care unit (NICU) (23). Incorporating supervised instruction may minimize these issues and also allow for direct and immediate comparison of examination techniques, clinical findings, and treatment recommendations between expert and novice. Moreover, supplementing supervision of indirect ophthalmoscopy with occasional live wide-angle digital imaging may prove to be a beneficial teaching approach. Several reports demonstrated that the use of digital imaging during laser treatment helps detect skip areas after panretinal laser photocoagulation (24). An even more recent study demonstrated the use of digital images to identify areas of missed laser by ophthalmologists in training, despite not being able to detect these regions by indirect ophthalmoscopy (25) (Fig. 34.4). With all concerns taken together, there is an increased need for ROP surveillance, but there is currently a lack of sufficiently trained ophthalmologists for examinations, and the need of trained ophthalmologists appears to be growing.
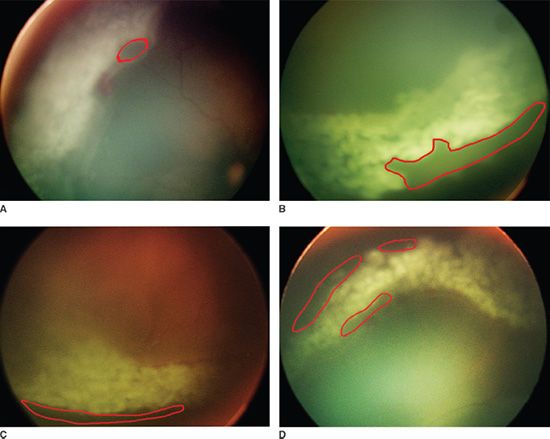
FIGURE 34.4 A: Digital retinal image (RetCam II, Clarity Medical Systems, Pleasanton, CA) of skip area (demarcated in red) adjacent to the ridge found in the 9:00 to 11:00 clock-hour region. B: Digital retinal image of skip area adjacent to the ora serrata found in the 3:00 to 5:00 clock-hour region. C: Digital retinal image of skip area adjacent to the ridge found in the 5:00 to 7:00 clock-hour region. D: Digital retinal image of several skip areas found in the 11:00 to 1:00 clock-hour region
Potential Solutions
Standardization of ophthalmology fellowship curricula may also help improve training in ROP management. Currently, the Association of University Professors of Ophthalmology’s (AUPO) Fellowship Compliance Committee is attempting to establish uniform training standards. For example, there are suggestions to retina fellowship programs regarding minimum operative numbers for vitrectomies and scleral buckles. However, fellowship programs are not required to follow these AUPO guidelines, and in fact, many reputable fellowships are not in compliance. Moreover, even among fellowship programs adhering to AUPO standards, there are no recommendations for pediatric ophthalmology and retina fellows regarding ROP examinations, ROP laser procedures, or assessment of competency in ROP management (26,27). Perhaps there is a need to establish a minimum number of ROP examinations and laser procedures, as well as incorporate other tools such as ophthalmic clinical exercises, 360 degrees assessments (evaluations based on multiple sources, such as supervising faculty, peers, residents, nurses, technicians, students, and patients), and global faculty performance ratings for ROP fellow training (28–31). These devices have proven useful in ophthalmology residency training and may be helpful in fellowship training as well.
Lastly, an area of needed research and commentary is the current American board certification process for ophthalmologists. Board certification and recredentialing every 10 years by the American Board of Ophthalmology is required for practice, but no credentialing is needed to offer subspecialty care, such as advanced surgeries in cornea, glaucoma, or retinal disease. The clinical significance of this regarding ROP involves results from Kemper et al. (32), which found that a large number of ophthalmologists without subspecialty training are performing ROP screening and treatment. It is unclear if formal training in pediatric ophthalmology or retina makes a difference in competency of ROP management, but a credentialing process to ensure certain standards of training would likely help with public accountability (33). Though an unproven correlate, studies in intensive care medicine, made up of a wide range of specialists, including critical care medicine, pulmonology, surgery, anesthesiology, and neurology, have shown that care led by intensivists with certification in critical care medicine is strongly associated with improved patient survival (34).
BURDEN OF ROP AND ROP EDUCATION: WORLDWIDE
Identifying the Problems
Despite major advances in management, ROP continues to be a devastating problem worldwide, causing blindness in more than 50,000 children (35). As expected, high-income and developed countries do not constitute the largest share of this staggering number, mainly due to high-quality neonatal services, excellent equipment, evidence-based screening protocols, and a sufficient access to ophthalmologists trained in ROP management. Perhaps surprisingly, low-income countries, on the opposite end of the socioeconomic spectrum, also are not responsible for the majority of these cases. In these countries, poor survival of preterm infants from a lack of neonatal resources reduces the number of infants at risk for developing ROP. Rather, the largest portion of blind children from ROP comes from middle-income countries and has been called the “third epidemic” of ROP (12).
Though most of the morbidity and blindness are potentially preventable in middle-income countries, these health care systems may not have the resources to deliver the high-level care necessary to effectively manage children with ROP. In these countries, rising numbers of blindness from ROP are multifactorial (36). First, when compared to higher income nations, teenage pregnancy tends to occur more often and utilization of prenatal care is less common (37). Second, though neonatal care is advancing and allowing survival of smaller and less mature babies, inadequate equipment and insufficient nursing staff do not allow for continuous supplemental oxygen monitoring and regulation. Lastly, screening programs tend to vary and the risk profile of babies at risk for developing ROP is different than that in high-income countries (35). Studies have shown that ROP occurs in larger, more mature babies in middle- than in high-income countries. Therefore, if protocols recommending screening of younger gestational age and smaller birth weight infants such as in high-income countries like the United States or United Kingdom are used in middle-income countries, cases of ROP may be missed (38,39).
Many middle-income countries have an inadequate number of ophthalmologists experienced in ROP management or lack facilities and infrastructure to deliver conventional laser therapy. Gilbert et al. (35) reported that in Lima, Peru, a single ophthalmologist provided ROP care for the entire city of 8 million people. Anecdotally, although there may be ROP coverage, some cities in Latin America lack neonatal units equipped with lasers or the necessary anesthesia services available for sedation or general anesthesia. Therefore, laser photocoagulation often cannot be offered in these countries.
Potential Solutions
Telemedicine and Tele-Education
Increasing awareness of ROP as a preventable disease and helping to establish local research in disease trends will help address the rising global epidemic of ROP. Experts from developed nations are conducting international workshops and conferences to help educate local clinicians and improve ROP programs in middle- and low-income countries. Educational initiatives and aid to these countries also already occur with organizations, such as ORBIS International (40,41) and Unite for Sight (42). However, many initiatives may only provide immediate but unsustainable help, for example, a one-time symposium or a surgical mission to help a finite number of patients. However, the goal should be to offer a more sustainable solution, such as training local clinicians to be competent in screening and treating ROP.
With this initiative in mind, a potential solution to managing the global burden of ROP is telemedicine, which is the use of information technology to support health care between entities separated from each other (43
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


