FIGURE 33.1 Vitamin A deficiency of public health significance in preschool-aged children, assessed using serum retinol levels. Regression-based estimates from available survey data. (From World Health Organization. Global prevalence of vitamin A deficiency in populations at risk 1995–2005. WHO Global Database on Vitamin A Deficiency. Geneva: World Health Organization, 2009.)
Vitamin A is found as retinol in animal food sources, for example, breast milk, cheese, fish, liver, and eggs, and as carotenes and carotenoids (provitamin A compounds) in plant sources, for example, yellow and red fruits (mango, papaya), dark green leafy vegetables, and red palm oil (35). Vitamin A is necessary for epithelial cell differentiation and growth, gene expression, immune responses, hemopoiesis, and organogenesis and is an essential component of rhodopsin. Approximately 95% of total body vitamin A is stored in the liver as retinal palmitate, and stores are usually sufficient for 6 months. Vitamin A is released from the liver bound to retinol-binding protein, which is transported to tissues bound to prealbumin.
VADD results from a combination of poor dietary intake, malabsorption (usually secondary to diarrhea and malnutrition), and increased tissue demand (caused by any illness particularly if there is fever). It is useful to think of the underlying causes of VADD as those that are distal (i.e., the macroenvironment) and those that are more proximal (i.e., household and individual factors). Distal causes include all those interrelated factors that lead to poverty, including inadequate education and health care systems, political instability, poor roads and communication systems, unfavorable climate and soil, lack of private landownership, and low prices for products in the international arena. Under these circumstances, the essential elements of primary health care are either not available or not accessible on account of distance, cost, or lack of awareness, and income generation is challenging. All these factors predispose communities toward poverty and the adverse health consequences. More proximal causes of VADD at the household level include low levels of maternal education, inadequate water supplies and sanitation, overcrowding and large family sizes, and lack of land ownership. The main factors that can cause a child who is borderline vitamin A deficient to become acutely deficient, with keratomalacia or corneal ulceration, include malnutrition, measles infection, and diarrhea.
Low dietary intake of vitamin A–rich foods does not necessarily mean that affordable vitamin A–rich foods are not available; inadequate breast-feeding, traditional weaning and child-feeding practices and taboos, and overcooking or sun-drying foods (which reduces the provitamin A content) are also important factors. Children born in communities where women of childbearing age also have low vitamin A status (characterized by high rates of night blindness) are also more likely to be deficient. Babies born to women with adequate vitamin A status will have adequate liver stores, but children born to deficient women will have deficit stores at birth, and the deficiency will not be rectified because breast milk levels of retinol will also be low (36).
In VADD, dedifferentiation of conjunctival and corneal epithelia leads to loss of goblet cells, squamous metaplasia, and xerosis of the conjunctiva and cornea (xerophthalmia). Bacterial action on deposits of keratin in the conjunctiva leads to accumulation of material, which has a white, foamy, cottage cheese–like appearance. These accumulations, Bitot spots, are usually located at the temporal limbus and are pathognomonic of VADD (Fig. 33.2). Reduced photoreceptor rhodopsin causes night blindness and, occasionally in adults, fundus changes. Acute VADD can lead to corneal ulceration and necrosis (keratomalacia) (Fig. 33.3). Conjunctival xerosis and Bitot spots are signs of long-standing VADD, found principally in children aged 3 to 8 years. Children most at risk of keratomalacia are those aged 6 months to 4 years, who may not have exhibited other features of xerophthalmia before the onset of corneal ulceration but who frequently also have protein energy malnutrition. Because not all children who are vitamin A deficient develop eye signs, it is important to be able to identify communities at risk, as children with xerophthalmia represent only the “tip of the iceberg” of those who are deficient in vitamin A in the community. Table 33.1 shows the WHO minimum prevalence criteria for the different ocular signs of VADD, which indicate that the condition is frequent enough to be a public health problem.
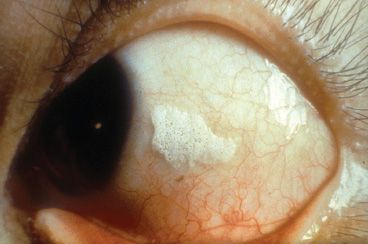
FIGURE 33.2 Bitot spot in a child with long-standing VADD. (Courtesy of Clare Gilbert.)

FIGURE 33.3 Keratomalacia in a child with severe, acute VADD. (Courtesy of Allen Foster.)
TABLE 33.1
WHO classification and minimum prevalence criteria for pediatric xerophthalmiaa and maternal vitamin A deficiency as a public health problem
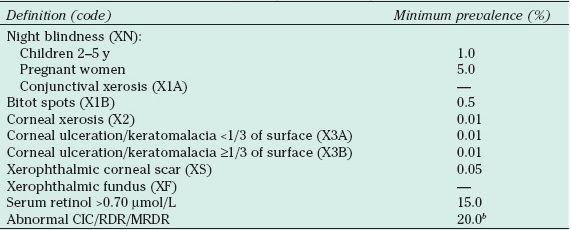
aAll stages refer to preschool children except where noted.
bProvisional cutoffs above which community interventions may be warranted.
CIC, conjunctival impression cytology; RDR, relative dose response; MRDR, modified RDR. Adapted from Sommer A, Davidson FR. Assessment and control of vitamin A deficiency: the Annecy Accords. J Nutr 2002;132(Suppl 9):2845S–2850S.
PRIMARY PREVENTION FOR THE CONTROL OF BLINDNESS DUE TO VADD :
• Poverty alleviation and development
• Improved water supply and sanitation to prevent diarrhea
• Education of women
• Child spacing and family planning programs
• Dietary diversification with health and nutrition education to improve the intake of vitamin A in children and women of childbearing age, that is, promotion of breast-feeding, appropriate complementary and weaning foods, home gardening, and instruction on the preparation and storage of vitamin A–rich foods. Biodiversity, through crossbreeding of foods to increase their provitamin A content, is also being recognized as another food-based strategy.
• Fortification of commonly consumed foods and bioengineering of commonly consumed foods to increase their pro-retinol content. This approach has been very successful in the Philippines, where monosodium glutamate has been fortified, for example (37).
• Measles immunization programs
• Vitamin A prophylaxis of individual children at risk, that is, those with measles and severe diarrhea from communities at risk
• Distribution of vitamin A to communities at risk (i.e., 50,000 IU every month for 3 months for infants aged 0 to 5 months; 100,000 IU every 4 to 6 months for infants aged 6 to 11 months; 200,000 IU every 4 to 6 months for children aged 12 months and older; for women, two doses of 200,000 at least 1 day apart postpartum) (16). Distribution can be through existing health care facilities, in conjunction with immunization programs or as a vertical program.
SECONDARY PREVENTION:
• Vitamin A treatment for all children with signs of xerophthalmia, that is, three doses given over 2 weeks
The mainstay of control is to give infants and children aged 6 to 72 months a high-dose vitamin A supplement every 6 to 12 months. Another component of the strategy is to supplement women of childbearing age. However, retinol is teratogenic and should only be given during the immediate postpartum period. Despite conclusive evidence that supplementation reduces mortality and prevents blindness, coverage is not as good as it might be in some countries, such as India (38,39), but reaches the target of at least 80% coverage in other countries (40).
TERTIARY PREVENTION:
• Optical iridectomy
Corneal grafting in children, particularly penetrating keratoplasty, is always challenging, but in low-income settings, there are additional obstacles. Children with corneal scarring usually come from the most disadvantaged families in the poorest communities, and they cannot afford the surgical, medical, and optical treatments and regular follow-up visits, which are essential for a good outcome; the child is likely to present late and will be densely amblyopic; good-quality corneal material is rarely available, and the majority of surgeons are not trained in the surgical techniques and postoperative care; and surgery is complex, as there are often adherent leucomas and secondary cataract. Finally, most corneal scarring in children is associated with vascularization, leading to very high rates of rejection. For all these reasons, corneal grafting is not recommended for the control of corneal blindness in children in developing countries (41). However, optical iridectomy can be very successful for children with dense, central corneal scarring, restoring sufficient sight for independent mobility and sometimes for more detailed tasks.
Measles
The measles virus is highly contagious, and measles infection can be associated with very high case fatality rates (42). The Expanded Programme on Immunization, which includes measles immunization, has had a dramatic impact on child deaths: in 1999, there were estimated to be 850,000 measles-related deaths globally (10% of all childhood deaths), which had declined to 139,300 by 2010 (43). More than 95% of these deaths occurred in low-income countries where measles immunization rates remain below the target of 80% coverage. The reduction in the number of cases of measles is leading to redesignation of “measles wards” in hospitals across Africa. Overcrowding, which leads to a higher infecting dose of the virus, is thought to be a major factor contributing to the severity of the condition, particularly in African children, where the case fatality rate can be as high as 34% (42). Studies in Africa show that approximately 1% to 3% of children develop corneal ulceration following measles; approximately a third of children with corneal ulceration give a history of recent measles, and up to 80% of children with corneal scarring give a history of measles.
The pathogenesis of measles-related corneal scarring is complex and multifactorial, and the following mechanisms have been implicated (44,45): (i) measles keratitis, which reduces corneal epithelium barrier function; (ii) secondary herpes simplex keratitis due to reduced cell-mediated immunity; (iii) secondary bacterial infection; (iv) exposure keratitis; (v) harmful traditional eye medicines, particularly in regions where measles infection is severe, that is, in sub-Saharan Africa; and (vi) acute VADD leading to corneal ulceration and keratomalacia. As retinol is required for epithelial differentiation, measles imposes a huge demand, as all epithelial tissues can be affected. Fever also increases the metabolic rate and demand for retinol, at a time when the child is ill and anorexic. Stromal herpes ulceration can make eating painful, and in many communities, there are customs and taboos concerning which food should and should not be given to sick children. Sick children are often given watery “soup” made of the local carbohydrate only, without oil, vegetables, protein, or vitamins. Measles infection of the gastrointestinal tract leads to malabsorption and protein-losing enteropathy with loss of retinol-binding protein (together with retinol) in the feces. Retinol is also found in the urine of children with measles. So, at the time when the child most needs high levels of retinol, the intake is low, absorption is reduced, and there is increased loss in the feces and urine. A child who had borderline liver stores, and normal serum retinol levels before measles, can be precipitated into severe, acute deficiency, leading to corneal ulceration, keratomalacia and blindness, and death. Clinical trials of repeated high doses of vitamin A have shown reduced mortality in children with measles (46). Vitamin A should be given to all children with measles, particularly those who live in areas where VADD is prevalent.
PRIMARY PREVENTION FOR THE CONTROL OF MEASLES-RELATED BLINDNESS:
• Measles immunization
• Health education regarding the use of harmful traditional eye medicines
SECONDARY PREVENTION:
• Diagnosis and appropriate treatment of corneal ulceration, that is, repeated high-dose vitamin A, antibiotics, and antiviral agents
TERTIARY PREVENTION:
• Optical iridectomy
Harmful Traditional Eye Remedies
In animist societies, disease is thought to have several origins, that is, they may be supernatural (caused by spirits or by angering ancestors or be due to breaking taboos); they may arise as a result of conflict, tension, jealousy, or immoral behavior; they may be the result of the “evil eye” or witchcraft; or they may be passed down within the family (through the mother). Other conditions are due to weakness, eating unclean food, or lack of respect toward parents or elders. Remedies are based on these understandings. The WHO has defined traditional healing in the following terms: “the sum total of all the knowledge and practices, used in diagnosis, prevention and elimination of physical, mental or social imbalance and relying exclusively on practical experience and observation handed down from generation to generation, whether verbally or in writing” (47). Traditional medicine might also be considered as “the solid amalgamation of dynamic medicine know-how and ancestral experience. Traditional African medicine might also be considered to be the sum total of practices, measures, ingredients and procedures of all kinds, whether material or not, which from time immemorial has enabled the African to guard against disease, to alleviate his suffering and to cure himself.”
The use of harmful traditional remedies, initiated or used as part of cultural practices within the family or community or administered on the advice of traditional healers, is an important cause of corneal blindness in children in developing countries, particularly in the poorer countries of sub-Saharan Africa (45,48,49). However, one has to bear in mind that traditional practices are widespread, and although some may be harmful, many are benign (e.g., ritual bathing, dances) or may even be of benefit (e.g., direct application of breast milk into the eye, steam baths and inhalations).
There are several mechanisms whereby traditional remedies can lead to ocular damage and blindness. First, injury to the adnexa (e.g., from chemical or thermal burns) can lead to exposure keratitis and secondary infection (Fig. 33.4). Exposure keratitis can also occur through parents keeping the eyes of the children held open, a practice believed to prevent blindness in children with measles in parts of West Africa. Secondly, objects and material inserted into the eye can cause mechanical damage. Examples include insertion of twigs and leaves, ground-up cowrie shells, and liquids or sap from plants, which are either acidic or alkaline. Thirdly, mechanical damage predisposes toward infection, particularly from fungi if plant material is inserted. Fourthly, infected fluids can lead to severe infection (e.g., urine from someone infected with gonorrhea, breast milk that has been expressed into a contaminated container) (Fig. 33.5). Lastly, harmless traditional remedies can lead to corneal blindness indirectly, as a consequence of delay in seeking more appropriate treatment.

FIGURE 33.4 Lid burn in a Tanzanian child with measles as a result of hot oil being administered. (Courtesy of Allen Foster.)
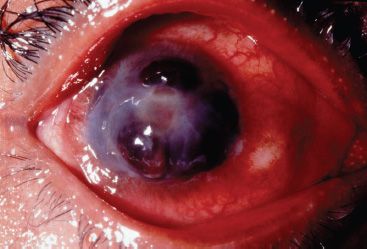
FIGURE 33.5 Gonococcal keratoconjunctivitis in a girl who had urine instilled as a treatment for seasonal epidemic conjunctivitis in West Africa. (Courtesy of Allen Foster.)
The practice of traditional healing varies enormously from locality to locality, even within the same country, and the tradition and remedies are often passed down within the family. Some healers develop specific areas of expertise, in the area of mental health, for example. Even in settings where eye care services are available, members of the community will often consult the traditional healer first or will want to discuss decisions having already seen an eye care worker, as they are respected members of the community who share local beliefs about the causation of disease.
PRIMARY PREVENTION FOR CONTROL OF BLINDNESS DUE TO HARMFUL TRADITIONAL EYE REMEDIES:
• Good primary health care and primary eye care services that are accessible and affordable
• Health education concerning potentially harmful practices
• Training programs for traditional healers, so that they avoid harmful practices and become part of the primary eye care system (50)
SECONDARY PREVENTION:
• Early diagnosis and appropriate treatment of corneal ulcers
TERTIARY PREVENTION:
• Optical iridectomy
Ophthalmia Neonatorum
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


