CHAPTER 3
Preparation of the Office for Allergy
GETTING STARTED: PREPARING THE SETTING
It must be presumed at this point that the physician has made the decision that adding allergy care, in some form, to the already existing practice will benefit both the practice and the patients. The prevalence of allergy as a major factor in the overall medical milieu has already been established, as well as its importance in evaluating other medical problems. In short, the otolaryngologist (or the primary care physician) will practice allergy, whether by design or compulsion.
This chapter deals not with science but with logistics. Nothing presented here should be taken as a rigid requirement for a successful practice. All practices are different, and subject to various needs and conveniences. The information presented here is the accumulation of several decades of trials, failures, revisions, restructuring, and successes, not only on the part of the authors but also of many of their colleagues nationwide who have introduced allergy into their practices and survived the ensuing struggles. Today the physician instituting allergy care has a wide range of options in determining the degree to which such care will fit into the practice. Most of these options are practical to expand as needed, as the allergy aspect of the practice grows. It is hoped that this information will help the novice overcome some of the normal problems encountered in starting.
Preparation
As stated previously, nothing should be taken as a rigid requirement in practicing otolaryngic allergy. There is one exception: preparation of the practice. Right from the start, in selecting space, site, and equipment, the physician must know the basics of the element that is to be added to the practice. If the physician has not attended appropriate basic courses or read available material, selection of a successful format may fall short of an effective level, and become expensive and unrewarding. Unfortunately, this poorly prepared approach is not uncommon. It results in the clinician’s becoming disillusioned and abandoning allergy care without a reasonable trial. No competent physician would attempt to add laser surgery to the office without appropriate training. The same considerations apply to allergy care. Today, a wide range of programs is readily available and well attended. Any physician so motivated may contact the American Academy of Otolaryngic Allergy (AAOA) and be advised of written material and available courses that provide the necessary background for preparing the office. Such programs also assist greatly in acquiring proper ancillary personnel, and in selecting the most appropriate format and equipment for an initial approach.
It would be best for not only the physician but also the direct allergy caregiver (nurse, technician, or assistant) to read this preparatory material in advance of setting up the logistics of practice, but this is not always practical (see later). In any case, the physician adding allergy should be quite familiar with the basic format before initiating the plans for the office if the best results are to be achieved.
General Considerations
Before discussing the possible formats of providing allergy care, let’s consider the possible approaches on an overall basis, including benefits and limitations, as well as specific requirements, to better prepare the clinician adding allergy to the practice to decide on an initial approach. Members of the allergy team can consult specific sections of this chapter for answers to questions that may arise.
Because the physician in charge of the practice usually makes the necessary preparatory decisions, this chapter is of importance primarily to that person. This is not an ideal situation. It would be better if the person providing the actual day-to-day care were able to have considerable input on preparing the area in which allergy care is to be practiced, but often this member of the staff has not yet been employed, or if only newly hired, may not be familiar with the specific needs of the practice. This entails some carefully thought out projection of actual needs on the part of the directing physician, who unfortunately often has little experience. If the member of the staff who will be performing the allergy testing and treatment is already employed in another role in the practice, it is to the directing physicians advantage to involve him or her in advance in the preparation of the area set aside for allergy. Often, this person will be able to identify projected arrangements that would make the daily procedures cumbersome and require later revisions in the layout, or make recommendations that would improve efficiency in effecting the transition. Of course, no one can anticipate in advance all the changing needs of an expanding allergy practice. It is often wise to be as flexible as possible until this aspect of the practice is well under way, thereby reducing the need for later major physical revisions in the area in which allergy is to be practiced. Provide the minimum setup anticipated, leaving room for individualized expansion as the practice grows and experience is gained.
If the person providing the allergy care has yet to be employed, as is frequently the case, the directing physician must prepare the allergy unit with only theoretical information. This is not easy, and it is common either to overestimate or to underestimate the needs in advance. However, even a limited initial commitment may be sufficient to allow the practice to provide good care, and to expand fairly easily as the need arises.
Approach
After the treating physician, and if possible the allergy caregiver, have undergone the necessary preparation, the next stage in arranging to provide allergy care is to move from the theoretical to the practical. The first consideration is whether to include allergy care as a significant part of the primary practice or to refer much of it to another treatment facility. Although commercial laboratories have been available for outsourcing of in vitro testing (and sometimes of antigen preparation), only recently has their use become popular. Prior to the ascendance of the commercial laboratory, the commitment on the part of the practice was of necessity much greater. Now there is a spectrum of programs available for those who have not yet determined their desired degree of commitment. Different formats may be appropriate for different practices. In making appropriate plans, there are three basic approaches to adding allergy care from the point of view of physical and personnel requirements. Each will be considered separately.
IN VITRO TESTING AND VIAL PREPARATION BY OUTSIDE SOURCE
There are many reasons for selecting this form of testing. Perhaps the most common is patient preference: “I want to get help for my allergies, but I don’t want all those needles.” Skin testing, although not especially painful, is sometimes an uncomfortable procedure. More to the point, however, is the advantage in vitro testing provides to the patient in both time and indirect cost. Skin testing takes quite a bit of time. If the patient must take time off from work or arrange for a baby sitter, considerable expense may be incurred in addition to the cost of testing. But having blood drawn takes only a few minutes. However, after the results are available, the patient must then take the time to undergo procedures similar to those that are done when skin testing is performed.
The description provided here of the space and furniture required applies to the office that does not plan to perform in vitro allergy testing on site. Under present circumstances, this is the most practical arrangement. In-office laboratories for in vitro testing became very popular in the 1980s, when costs had dropped to a reasonable level and a certain prestige accrued to performing everything on an on-site basis. Unfortunately, during the early 1990s costs escalated, and third-party payers frequently balked at paying for in vitro testing, although studies confirmed its cost-effectiveness. But the final blow for in-office laboratories may have come in 1988, when they were placed under strict governmental regulation according to the Clinical Laboratory Improvement Act (CLIA). As a result of these factors, by the 1990s this type of testing became impractical in the small office. Times and conditions change, however. There has been some liberalization of the controls, but few small offices have felt a need to face the challenges again. For the present it is far more practical to have the patient’s blood sent out to a reference laboratory. Results are controlled, and the turnaround time is close to what could be achieved in the private office. The physician needs to understand the principles and mechanism of in vitro testing to assess and apply results, but it is more practical to leave the actual performance to the reference laboratory, which is better equipped to assume the necessary controls. The office must still check the results against the patient, by limited skin testing, but it need not cope with all the problems.
The approach of outsourcing both in vitro testing and vial preparation is the simplest and least demanding one, and today may be employed with an acceptable degree of success. The format is simple. A good history is taken and an appropriate physical examination is performed. Based on the findings, a decision is made that the problem is probably an inhalant allergy. (This approach does not work for food allergy; see Chapter 13.) When the decision is made to use this approach, blood is drawn from the patient and sent, properly prepared, to a reference laboratory for the appropriate radioallergosorbent test (RAST) or the enzyme-linked immunosorbent assay (ELISA). The specific tests to be performed are determined by the treating physician. A battery of tests, appropriate to the area, can be selected. A list of these tests is readily available from most major reference laboratories, or specific tests can be selected that are indicated by the patient’s history. At times, testing for a seasonal group of allergens maybe indicated; a list of these tests is also available. For a more detailed picture of the allergens usually necessary, see Selection of Allergens for Treatment. The previous approach usually provides a satisfactory list to begin with, which may be altered later as needed.
The turnaround time for such testing is usually brief. When the results are available, the physician must correlate them with the patient’s clinical picture, and if allergy is felt to be a significant contributor to the patient’s symptoms, the physician should discuss in detail with the patient the appropriate therapeutic modalities available (environmental control, pharmacotherapy, and immunotherapy). If the physician recommends immunotherapy, and the patient agrees to proceed with treatment, a prescription or order form indicating the antigens to be treated and the concentration (end point) for each is sent to the same reference laboratory doing the testing, and treatment vials are prepared (Fig. 3-1). The importance of using the same laboratory is that when using in vitro testing (as opposed to in vivo testing), the testing antigen is not always identical to the treating antigen. Using the same laboratory for testing and treatment preparation is the best way to maintain the highest degree of uniformity possible. When the vials are returned to the treating physician, careful vial testing is performed as described in Chapter 10. Treatment is instituted and escalated as described in the chapters on treatment. As would be expected, there are advantages and disadvantages to this approach. The major advantage is a minimal investment in space, equipment, and personnel. The major disadvantage is a lack of control over some elements that would allow a more individual approach to patient care.
Space
The amount of space necessary for this method of testing is somewhat less than that needed for complete skin or in vitro testing, and the space needed for vial preparation is greatly reduced. But not all space needs are eliminated (Fig. 3-2). Vials received from the commercial laboratory must still be tested against the patient’s skin response prior to use, and possibly adjusted (the format for vial testing is discussed in Chapter 10). Treatment space is necessary, as is a place for patients to wait, often for 30 minutes, after receiving an injection. These areas should be separated from the general practice as much as possible. The treatment space should be at least 8 by 10 feet, with room for a desk and refrigerator. Space is also needed for record keeping; allergy treatment records are best kept separate from the general office records.
Equipment
The necessary equipment includes syringes, vial racks for treatment vials, alcohol swabs, sharps containers, and, most essential, emergency equipment (see Chapter 11). Although emergencies are extremely rare in proper otolaryngic allergy care, preparation for them is essential. A moderate-size tray or drawer will usually hold all that is really needed in most offices.
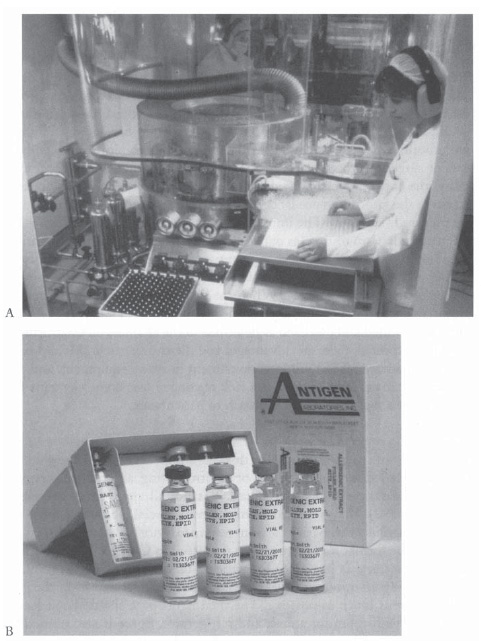
Figure 3-1 A: The use of a commercial laboratory for both a radioallergosorbent test (RAST) and treatment vial preparation has become moderately popular recently, partly due to economic pressures. The licensed commercial laboratory is well equipped to prepare treatment vials under properly controlled conditions. B: After testing the serum and preparing the extracts, the laboratory provides progressive treatment vials to the physicians office. (Courtesy ofALK-Abello, 1700 Royston Lane, Round Rock, Texas 78664 and Antigen Laboratories, Inc., P.O. Box 123, Liberty, Maryland 64068.)
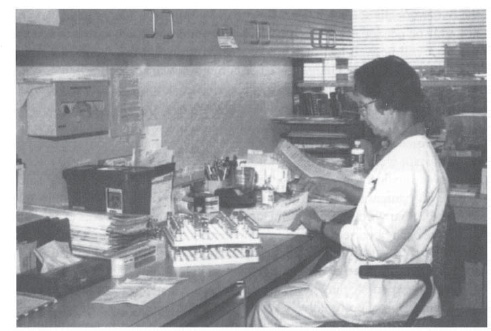
Figure 3-2 Finding adequate space may present a problem when allergy is added to an existing practice. With ingenuity and careful planning, however, a small space can be used if necessary.
Personnel
In addition to the treating physician, who ultimately makes all of the treatment decisions, at least one additional caregiver is needed. This person need not be a full-time employee (especially initially), although there is a definite advantage if this can be achieved. Treatment can easily be restricted to certain times of the workweek, but patients’ questions about allergy care will come at any time, and it is certainly much easier to handle them if the person administering the treatment is present full-time.
How this problem can be approached varies with the office. One possibility is to have a full-time member of the regular office staff be the person trained and delegated to administer allergy care at scheduled times. Then questions can be easily referred to this person. As the number of allergy patients increases, this referral for questions may become more difficult to handle, as this person may be involved in other aspects of care. Allergy questions rarely need an immediate response, however, so the clinician can return the patients’ calls at a later time. Eventually, a full-time allergy caregiver will probably be needed as the allergy practice expands, at which time hiring such a person will be well justified. Up to this point, however, we are discussing only a person directly charged with selecting, measuring, and administering allergy injections in a limited allergy practice, and doing vial testing and making necessary vial adjustments. Office preparation of vials for testing and treatment is not considered in this format.
What qualifications should this allergy caregiver have? A nurse or physician assistant would be an ideal choice, but this option is not always available in today’s medical climate. At a minimum, this person should have some nursing or comparable training, to cope with emergencies. He or she should also be familiar with blood drawing and injection procedures. This experience may have been obtained prior to employment in the allergy office. Otherwise, training may occur through attendance at courses, or may be administered by or under the guidance of the physician.
Previous experience in allergy care as such is not always a benefit, as there are several approaches to allergy treatment, and it is often beneficial to train the person in the specific method used in the practice. To this end, referring the person to one or more approved courses is by far the best approach to providing the best level of care and reducing the strain on the directing physician. This training may be supplemented by the use of published material. As noted previously, the AAOA is an excellent source for information on appropriate courses and supplements. In many cases, a visit to an established practice providing allergy care can be arranged, and will greatly aid the caregiver (such a visit can also be of great value to the physician).
Potential Drawbacks
One drawback to using this approach is that it reduces adaptability. It is more difficult to test one or more additional antigens after immunotherapy has begun, and to readjust the treatment vial to include them. Other adjustments to treatment vials cannot be conveniently made as needed. In short, the personal element has been transferred to an outside entity. Although this approach is safe, most patients prefer to have as much of their care as possible handled at one location by a physician who is familiar with all of their problems. This is especially true of allergy, which is an ongoing condition. Although the impact of managed care may have made it necessary for the physician to reduce the time spent with the patient, patients still want a personal relationship with the doctor and the staff. Having all studies performed off-premises, and (more importantly) treatment vials prepared elsewhere, may tend to erode the patient s confidence in the physician, which is highly important in effective allergy care. Another disadvantage is that, by law, there is a delay period mandated for the commercial laboratory before vials can be shipped, to confirm sterility. This in turn delays the institution of treatment, and often frustrates patients and caregivers alike.
There is a risk in having treatment vials prepared elsewhere. There is always the possibility of human error, either in sending the vials back and forth, or in preparing them in the office using a different approach. Careful selection of the commercial laboratory should minimize this risk.
Another drawback concerns insurance coverage. Although allergy care is covered by insurance, many insurance companies have their own rules about what testing methods are compensated, and this inevitably impacts decisions as to how to provide the care necessary. Not only are the rules different for different companies and different states, they tend to change frequently. The AAOA generally provides practice management courses at its annual meeting, and assists its members on an individual basis as they deal with carriers, but each office must have one staff member develop expertise in insurance coverage issues.
IN VITRO OR SKIN TESTING AND OFFICE VIAL PREPARATION
Because the space and equipment needed, as well as the personnel, are practically identical when using either of these two approaches, many offices use a combination of the two. This combination gives the treating physician the most latitude in formulation of treatment vials, including limited skin testing for additional antigens, and in reformulation of vials (such as breaking down a vial into several components when skin reactions are noted). Although the novice may start by outsourcing both testing and treatment, many practices, especially those doing skin testing, eventually move to in-house vial preparation. The information presented here is more detailed, as this approach requires consideration of the needs for full allergy care. Space, furniture, and equipment must be carefully considered, and additional personnel may need to be employed. Hiring good personnel and providing appropriate training are especially important, but the first consideration is space.
Space
The space needed to perform allergy testing and treatment is not extensive. If necessary, a small space can be used, but the space should be large enough so that the patients and staff will feel comfortable. No heavy equipment is needed. If the room chosen already has a sink and an electrical outlet for a refrigerator, no new plumbing or electric wiring is necessary.
The space should be close to the clinical area of the office, so that assistance is readily available in the case of syncope or treatment reactions. Space is also needed for the preparation of the vials of extract used in testing and treatment. This may be a part of the testing and treatment section if space permits, and this is always convenient. It can be separated from the rest of the office simply by closing the door to bar interruptions while testing and treatment vials are prepared. This contiguous office space is frequently at a premium, however. It is quite acceptable to have testing and treatment vials prepared elsewhere within the office complex, where there is more space. Here, a large refrigerator to hold bulk extract and prepared vials and a table for vial preparation are needed. It can easily be seen that there is a benefit in combining this area with the main allergy section; the prepared vials are then immediately at hand, but the alternative is a possibility that has been used successfully in many locations.
The person preparing the vials should ideally be familiar with the patients, as should be the regular allergy caregiver. The same person may perform both tasks at different times, or another person, possibly a part-time employee, may prepare the vials. This affords the opportunity for another person to become familiar with allergy protocol and the treatment methods, in case the regular allergy caregiver is absent. It is not practical, however, for both persons to be occupying the main allergy section at the same time. This produces even more confusion than calling on the allergy caregiver for other needs.
The amount of space necessary to start is actually not great. A single room measuring 10 by 12 feet is adequate for basic testing and treatment (a smaller space might be adequate, but would tend to produce a feeling of claustrophobia). This testing area need not be within the treatment area, but it should be nearby so that the treating physician can easily reach the allergy testing and treatment area should a problem arise. There are benefits to having the allergy section, especially the allergy waiting room, physically somewhat separate from the rest of the office. Allergy patients are seen much more frequently than other patients, and they tend to attach closely to both the physician directing their treatment and the person directly administering it. This is an advantage from the point of view of improving and expanding the practice. However, it can seriously interrupt the work of physicians if every patient has the opportunity to intercept them with questions while they are attempting to move efficiently through the office to handle the daily nonallergy patient load. Separating the allergy testing area from the general office by a door that can be closed provides such a division for practical purposes while making the area quickly accessible if help is needed. The allergy area should be free from perfume, air fresheners, and other chemicals, as many allergy patients are sensitive to odors.
It is also advisable to arrange in some way to have allergy patients clearly separated from other patients throughout their visits. This may be accomplished by having a separate receptionist handle and route allergy patients. Alternatively, when the allergy portion of the practice is still small, the member of the team administering the testing and care may receive the patients in person. (As the practice grows, this will quickly become impractical.) Having allergy patients processed through the same receptionist as other patients quickly becomes prohibitively cumbersome. Allergy visits for immunotherapy are brief. The patients are in and out of the treatment area in minutes, although they should stay in the office for at least 30 minutes after receiving an injection, in the interest of safety. Ideally, they should stay in a separate waiting room. The more the allergy part of the practice can be separated from the rest of the practice, the better and more smoothly it can be run.
There are other reasons to separate the allergy portion of the practice from the general part. These reasons may not seem important initially, but if ignored they tend to produce increasing problems with time. Testing sessions may be scheduled at regular time intervals, but allergy testing and treatment require careful timing and measurements. Interruptions should be kept to a minimum. There is always the temptation on the part of the physician to call on the allergy treatment person when an additional hand is needed elsewhere in the office. The allergy section may appear to be quiet at the moment, but if skin testing procedures are under way, for example, the person providing the care must time and measure the responses accurately if good treatment results are to be obtained. An unexpected delay in timing may invalidate an entire test series.
Even more deleterious is interrupting the person involved in preparing the vials of allergenic extract used in both testing and treatment. Test vials must be remade every 6 weeks if potency is to be maintained. The same procedures used in making testing vials is used in making treatment vials, and in a small practice the same diluted series of vials may be used for both testing and treatment. If these become confused as a result of an interruption during the procedure, not only may test results be invalid but the treatment can be compromised. This is comparable with a pharmacist dispensing the wrong drug. Allergenic extracts for treatment, using this approach, are prepared in the office, and the same care as would be required in a laboratory is essential for reliability and safety.
The directing physician must be aware of the need for concentration by the person engaged in extract preparation. This problem may often best be solved by having the testing and treatment extracts prepared in a location not directly attached to the clinical part of the office, and therefore not readily visible. It is sometimes a good idea to have them prepared by another person, possibly someone more accustomed to laboratory procedure, leaving the person charged with testing and treatment free from these time constraints.
Furniture
The furniture needs are simple. A standard secretary’s desk and chair, without arms, are suitable for both testing and treatment. It is easier on both patient and allergy provider if the patient is positioned a little above the standard chair level, although this is not absolutely necessary. A bar stool provides a convenient elevation if the patient is to be present for an extended time, as in skin testing. A couple of chairs for family members should be provided. In addition to a sink, refrigerator, and sufficient counter space for work (Fig. 3-3), the only other item needed is specific allergy equipment (see later in this chapter), which can be obtained through various allergy supply houses.
Allergy Equipment
The special equipment needed for allergy testing and treatment and for the actual allergenic extracts are discussed separately, although both may be obtained from the same source, for convenience. The basic equipment needs are simple: glass vials, racks to hold the vials, syringes, and bottles of diluent to be used in preparing the vials. Intradermal dilutional testing (IDT), which is used by most otolaryngologists as well as many nonotolaryngologists, is the one presented here, although other formats are available. It would be impossible to present all possible testing and treatment formats, and IDT has a proven safety and convenience record extending over 35 years, although from time to time the name has been changed. Skin end-point titration (SET) is the prototypical method on which IDT is based. Other variants are also in use, but the basic equipment required remains the same.
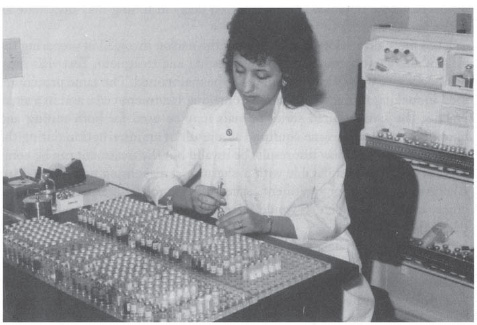
Figure 3-3 Sufficient counter space to allow mixing and access to vials is necessary in the plan of the allergy office.
GLASS VIALS For IDT, 5-mL testing vials with aluminum-protected rubber stoppers are used, containing 4 mL of buffered saline diluent. This saves on-site measuring and time. In the early stages of practice, or if the number of allergy patients is small, these vials, when properly prepared, may be used for both the testing board and preparation of individual patient treatment vials. The details of preparation are presented in Chapters 5 and 8, which discuss inhalant testing and immunotherapy. The number of vials required initially can be computed when the number of allergens that will be on the testing board is known (see Selection of Antigen for Therapy). Six of these vials containing diluent are needed for each antigen. These have to be remade every 6 weeks. Simple multiplication and a cost evaluation based on quantity purchase should provide the necessary information. These vials provide the initial testing board, and can be used to make the patient treatment vials in the initial stages of practice. The preparation of a separate treatment board can be considered when the practice grows beyond this format.
Empty glass vials are needed for the preparation of extracts for patient treatment. Most of these vials are also of the 5-mL size, but when a large number of antigens are needed a 10-mL vial may be required, so a few vials of this size should always be on hand. In the early stages of treatment, during buildup immunotherapy, the patient should receive all injections in the office whenever possible, as is discussed in more detail in Chapter 8. In the early phases of treatment, this approach allows for better safety and a better picture of the patient’s progress. Later on, when maintenance dose levels are reached (and under special circumstances), the patient will probably take injections at home, or in another physician’s office. When this time arrives, it is advisable to make unit doses for the patient using 1-mL vials and at least partly filling them with diluent. At that time, 1-mL vials will be needed, but from the start of allergy practice to this point will usually be a matter of several weeks or a few months. It may be advisable to purchase some 1-mL vials immediately, but the quantity need not be large.
RACKS FOR VIALS Containers for the vials containing the diluted antigens are an immediate necessity. With an IDT format, vial racks will contain six progressive dilutions, so the racks must be at least six rows deep and have sufficient numbers of columns to accommodate each antigen to be tested (and extras for future use). Five-milliliter vials are supplied in most cases in a thin plastic rack, which may be used in an emergency but will not prove adequate during any long-term use for the testing board. The racks may, however, be used to store treatment vials (Fig. 3-4).
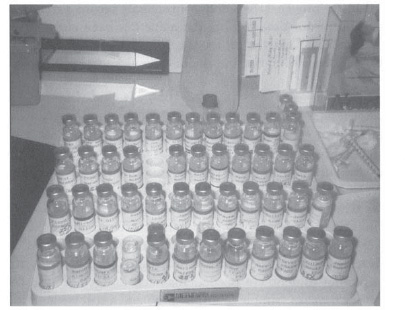
Figure 3-4 The plastic trays used to ship empty or diluent-filled vials can also be used to store patient treatment vials if necessary. However, they are not sturdy enough to hold stock antigen dilutions for testing and for making treatment sets.
Many physicians have Formica racks made for the office when the allergy section is designed. This arrangement is very attractive, and blends in with the space. The disadvantage is that these racks cannot reasonably be refrigerated, which limits the duration of potency. Refrigeration may almost double the life of vials that are in constant use, but their frequent use makes transferring racks of testing vials to and from the refrigerator between patients an inefficient maneuver. Nevertheless, in the early stages, when few patients are involved, refrigerating everything is of appreciable value. Probably the best vial racks are made of acrylic, 10 holes wide and at least 6 holes deep (Fig. 3-5). These may easily be transferred to a refrigerator, and when the practices volume increases, they may be used to hold patient treatment vials, which always require refrigeration. Most allergy supply houses are able to provide such racks or direct the physician to a reputable source. Whenever injections are not being given or vials prepared, all vials and antigenic material should be refrigerated.
NURSE’S NOTE
Only the dilutions #1 through #6 of each antigen should be on the testing board. Concentrates are generally purchased in vials larger than can be accommodated on the board. Even if small bottles of concentrate are being used, however, these are never kept on the board, in order to avoid inadvertent administration of an injection or test from a bottle of concentrate.
Only the material being used should be removed from the refrigerator. If testing is being done, only the testing board is removed. If injections are being given, only the patient vials are removed. This not only prevents inadvertently picking up the wrong vial, but also preserves the potency of the antigenic material. When made without added glycerine, antigen mixes and dilutions lose significant potency after 6 weeks, and earlier if they are not kept refrigerated when not in use.
SYRINGES Two types of syringe with attached needles (labeled allergy syringes) are available for use in the allergy office: testing syringes and injecting syringes. Both are available in 0.5- and 1.0-mL sizes. Although the two are interchangeable in practice, there are differences, and the person ordering the syringes will be faced with the decision of which, and how many of each, to order. The difference is in the bevel of the needle. A testing syringe has a shallow bevel, allowing the test injection to be made easily in the upper layers of the skin with minimal insertion. The injection syringe has a long bevel, which causes less pain during injection. Each has its benefits, but either may be used for the other purpose when necessary. A good compromise in the early stages is to order an equal number of each (by the case) and, when supplies run low, to use whichever is left in greater quantity until new supplies arrive. After the first few orders, a reasonable proportion should be evident.
Figure 3-5 An acrylic rack serves well to hold the various dilutions of the antigens needed for skin testing and for making treatment sets.
Do not try to substitute tuberculin syringes for allergy syringes unless absolutely necessary. These syringes do not have needles as an integral part, and as a result roughly 0.05 mL of the injection material is left in the hub and barrel of the syringe. This makes testing difficult and treatment wasteful (see Chapter 8).
DILUENTS Through the years, a variety of diluents for allergenic extracts have been utilized, but the current standard is phenolated buffered saline solution. Largely for informational purposes, a brief mention will be made of other diluents. Some are still in use, and the novice allergist should be aware of them, but will not necessarily employ them.
Normal Saline Solution This is a diluent of the same consistency as normal body fluid. It is safe and predictable. It lacks any preservative, limiting its potency span. Extracts made with normal saline diluent should be used completely or replaced every 6 weeks. Because it does not contain a bacteriostatic agent, normal saline solution has been largely replaced by phenolated, buffered saline solution (described later).
Human Serum Albumin For a time, there was much concern over the significance of the “walling” of antigen when serial dilutions were mixed. This condition occurs when normal buffered saline solution is used as a diluent. Antigen tends to adhere to the glass of the vials, making successive dilutions less potent. In actuality, it was found in subsequent studies that the degree of walling was minimal, and that concerns about its effect were truly unfounded. In addition, the public became seriously concerned about the possibility of transmitting AIDS or the hepatitis B virus through the use of human serum. Again, in actuality the concern was unfounded; both viruses are highly heat-sensitive, and all human serum albumin products were heated far above virus survival level before being placed on the market. The product was more expensive than buffered saline solution, however, and this coupled with public concerns limited its use, especially because the benefits were found to be insignificant.
Buffered Saline Solution After years of experimentation, this product is considered the standard. Buffered saline solution is normal saline solution to which two important additions have been made: phenol, in a concentration of 0.04%, is bactericidal and virucidal, and sodium bicarbonate or a similar compound is added for pH adjustment. Buffered, phenolated saline solution is inexpensive and practical. It may be bought in bulk and kept for a long period, as designated by the expiration date on the bottles supplied.
Glycerine Glycerine is not a diluent per se, but it is a preservative. A moderate supply (a few hundred milliliters of 50% glycerine) should be purchased. This is used in the preparation of treatment vials in the format described in Chapter 8.
Additional Materials In addition to the already mentioned materials, the allergy office will also require a large supply of cotton balls, alcohol, and alcohol wipes. An occasional patient will require a spot bandage to prevent bleeding from an injection site from staining clothing. Sharps containers are necessary, and arrangements must be made to dispose of these and other biologic wastes in accordance with appropriate regulations. With these supplies, and antigens selected and purchased appropriately, the physician has made the necessary physical preparations to begin adding allergy to the practice.
SELECTION OF PERSONNEL
Clinicians vary in their approach to allergy testing and care. Most otolaryngic allergists delegate much of the actual testing and treatment of allergy to ancillary personnel. This is a perfectly acceptable approach if the person involved in the testing and treatment is well trained and concerned. Decisions regarding rapid dose escalation and terminating therapy remain the province of the clinician directing the treatment. However, making day-today changes in therapy, communicating with patients, and answering their questions may often be better handled by the appropriately trained person doing the testing and actively administering the treatment. This person is in closer contact with the patient, observes the patient’s attitude, hears the patient’s comments, which often are not voiced to the doctor, and provides an invaluable liaison for adjusting therapy to achieve better results. Despite the changes in the public’s view of medicine, in most cases the doctor still is viewed with a certain degree of awe, and the patient adjusts the history to whatever will provide the best personal image. This image may not be totally accurate, a situation that may affect effective diagnosis and treatment. The allergy nurse or assistant, who performs testing and provides regular treatment, has more personal contact with the patient and is usually viewed more as a confidant than as a provider. Thus this key team member is able to obtain an ongoing history, identify weaknesses in the treatment program, detect new exposures, and provide the treating physician with the material necessary to direct the treatment program accurately. The selection of this person or persons may be the most important single decision in preparing to provide good clinical allergy care.
Personal Characteristics
Not every person with a medical background is ideal for the position of allergy care provider. Although nurses may make excellent members of the allergy team, some are not temperamentally suited for this type of practice, and conversely, a hospital-type nursing background is not necessarily a prerequisite for becoming an excellent allergy assistant. Regardless of background and experience, such persons must have certain traits and interests if they are to provide good care and if they, the patient, and the treating physician are all to be pleased with the result. First, the person must desire ongoing patient contact, which not everyone wants. Many prefer to do a good job during their assigned time, and then go home and not be concerned with the job until the following day. These people are much better suited to hospital environments in which ongoing, long-term patient care is not an issue because of constant patient turnover. Good allergy caregivers like to follow their cases throughout the treatment and to observe the outcome. In an allergy practice they will have ample opportunity to do this.
Second, the ideal person for this job wants a degree of autonomy. Although this person will not make overall treatment decisions, which are the province of the treating physician, the allergy care provider should always be able to turn to the treating physician for advice and instruction. It is to be decried that even today, some physicians with allergy practices send their care providers to educational courses and then rely on them for critical decisions. The physician directing treatment should always be better educated than the ancillary personnel, as the physician must be held responsible for errors in treatment direction. The person providing the day-to-day care, however, should be prepared to plan testing, adjust treatment, and work with the patient on a plan to achieve the best results. This provider should take pride in making strides in improving the patient’s condition; in return, the majority of patients will credit their improvement primarily to the provider. If the directing physician is both secure and competent, the work of the care provider will be both acknowledged and appreciated. The treating physician will always be available for consultation and help and will check the patient at regular intervals so as not to lose control at any point, but will credit the provider with results obtained. This mutual recognition and respect facilitate optimal patient care.
The best allergy care provider is endlessly curious, which impacts the provider at two levels. First, the provider is the ongoing source of the individual patient history. The uncommunicative allergy provider will miss most, if not all, of the patient s changing problems. Chatting with the patient while giving therapy and observing the result, as well as discussing additional testing, provides an opportunity to identify new allergenic exposures and to perceive unrelated conditions easily confused with allergy. When the patient is receiving allergy care, there is a strong tendency to identify any new problems as directly allergy related. The physician does not see the patient on every visit, and may not be as able to spot an unrelated situation as is the regular provider. Second, the curious allergy care provider will read the paramedical and lay press and will bring pertinent articles to the attention of the treating physician for discussion. Many of the articles in the lay press will be of no importance, but some will stimulate the physician to further investigation, and it is not unusual to have such information lead to a breakthrough in a difficult situation. In addition, this provision of advance notice of information in the lay press will prepare physicians to field questions from allergy patients who have also read the articles.
Training
The allergy care provider should be well trained and knowledgeable in the field of practical clinical allergy care. A significant degree of autonomy in daily performance requires this knowledge. It is not always reasonable to expect this training and knowledge as a prerequisite to employment; it can be provided after the person is hired. There are situations in which previous experience with allergy care may be a benefit, but it is not necessary. The range of specialties involved in treating allergy, and the years during which allergy has been treated with a variety of methodologies, have led to a diversity of approaches to the field. Although today there is little disagreement regarding the principles involved, ancillary personnel trained in one approach or another without an extensive immunologic background may often have difficulty adjusting from one approach to another. It is usually to the benefit of the primary physician to arrange to have the allergy provider educated in the specific approach to testing and therapy that is to be employed in this particular practice. The treating physician has the ultimate responsibility in directing care, and therefore should be even more familiar with current knowledge and approaches to practical allergy care than the employee. Fortunately, this familiarity is not difficult to acquire. A variety of courses in basic approaches to allergy care are offered by schools and organizations, most notably the AAOA. These courses should be attended by both the treating physician and the employed allergy care provider. Ideally, both should attend together, so that the physician has the opportunity to clarify any material presented that may be too technical for the allergy care provider to understand. This interchange between employer and employee can prove of inestimable value in future treatment considerations. The approach described has been proved effective repeatedly by the authors during decades of practice. Not only does it provide an opportunity for cooperation between employer and employee, but it also affords a familiarity with the same material, allowing appropriate evaluation and application of such material by both members of the team.
The AAOA is the national organization most directly involved with supporting otolaryngologists in the clinical practice of allergy. It is the oldest allergy organization in the United States. The AAOA is separate from, but works in close cooperation with, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) and other related specialty societies, such as the American Rhinologic Society. The AAOA offers regular courses, both basic and advanced, and advertises them through mailings to all otolaryngologists, as well as to other physicians who have expressed an interest. Membership in the AAOA is available to physicians and allied health providers, and the status of Fellow may be attained by completing specified training, submitting case reports, and passing a written and oral examination. The AAOA also has available other teaching aids to supplement the scheduled courses. Full details may be obtained from the AAOA headquarters (1990 M Street NW, Suite 680, Washington, DC 20036; www.aaoaf.org).
Traditionally, because of the diversity of approaches to allergy care, it was often said that any intelligent and interested person, properly motivated, could be taught to be a highly successful allergy care provider. The allergy care provider is expected to be able not only to draw blood, inject the patient with immunotherapy vaccine, and verify the appropriateness of the injection, but also to identify and cope with any emergencies that might arise, among other things. In addition, the autonomous nature of the caregiver-patient relationship make it beneficial for the caregiver to have enough basic medical knowledge to at least suspect unrelated problems and bring them to the directing physician’s attention. Although this still leaves a wide range of background possibilities present, it does limit the pool from which assistants can be drawn with a degree of confidence. It remains the responsibility of the treating physician to assess the capabilities of the potential members of the allergy team, and assist them in securing any additional training needed before they enter into patient care. Today, society has become far more litigious than in the past, so the selection of allergy team members becomes especially important.
A medical or paramedical background is not necessary for the person whose job is making testing and treatment vials. A laboratory background may be preferable, and this might be a part-time job. There are benefits, however, in having the person who prepares vials also be able to provide treatment, as this allows a greater degree of flexibility in the practice. This decision will vary with the office.
Reference books, monographs, and comprehensive sources of practical information are unfortunately in somewhat short supply for the beginning clinical allergist. Indeed, this was the impetus for the present text. Books and monographs may serve as excellent supplementary sources of information, but they cannot substitute for experience. Thus, they should be supplemented with individualized teaching, such as at an approved course or at the hands of a mentor. The field of allergy is far too large to lend itself to “cookbook” approaches. The size of the field should not overwhelm the novice, however, or frighten the new allergy care provider. It is quite possible to diagnose allergy safely and effectively and care for a large percentage of allergic patients, so long as practitioners recognize and respect the limits of their capabilities. As in any field of medicine, more extensive knowledge comes with time, and some early failures may later be converted to successes. And, as in all of medicine, care and caution are necessary, especially in the early stages of the allergy practice. When both physician and allergy care provider are well established and secure with basic material, consideration may be given to undertaking more advanced aspects of care.
After the basic training has been completed through courses and reading material, a final step will greatly benefit the addition of allergy to the practice. Both the allergy care provider and (preferably) the physician should communicate with a practitioner who has an established practice and arrange to visit the office. Most such practitioners, and especially those involved with teaching, are quite amenable to having visitors. This visit gives the physician and care provider the opportunity to see allergy care in action. Office patients usually range from new patients just referred for care after an initial evaluation, to patients in later stages of care and those being evaluated for discontinuation of care. This spectrum cannot be adequately presented at a teaching course, as the necessary didactic material simply takes up too much of the course time. Most courses, whether in allergy or any other facet of medicine, compress weeks or months of learning into a few days. The students feel overwhelmed by the volume of material presented. Thus, it is helpful to be able to immediately apply the material they have been exposed to, while it is still fresh in their minds. Visiting a working allergy practice greatly facilitates this immediate application process and allows the neophyte practitioner to see the course material put into practice and adapted to the needs of the practice.
Every practice is different. The types of patients in the practice are determined in part by geographic population. A large geriatric population will not have the same needs as a large pediatric population. Climate, local occupations, industry in the area, and an urban versus an agricultural setting are some of the factors that determine what allergy care equipment and procedures are needed. Courses and reference books of necessity include information appropriate to all practitioners in all areas. Only a fraction of this information will be pertinent to one specific practice. Analyzing specific needs in advance will provide major savings in equipment and supply costs, and usually will make both physician and care provider more comfortable with starting the new aspect of the practice.
Job Description
The need for the allergy care provider to concentrate on one job only may present a problem in the early stages of the allergy practice, when there are not enough allergy patients to keep the care provider fully occupied. This can be circumvented by limiting the time set aside for both allergy care and vial preparation. Allergy testing or care in an office practice is rarely of an emergency nature. An office informational handout or sign can tell patients at what times allergy testing and treatment will be provided. This serves the dual purpose of controlling the allergy schedule and advertising to the patient population that allergy care is available. When the allergy schedule is established and strictly adhered to, the allergy care provider may be free at other times to share in the general duties of the rest of the staff.
When the allergy portion of the practice becomes active, another consideration becomes necessary. As noted, providing allergy care is a specialized job, requiring advance training and on-the-job continued experience. It is to be hoped that the physician in charge will be significantly more knowledgeable about the field than the specific care provider, but the physician already has major demands on his or her time. If the allergy care provider becomes ill or leaves the practice, the physician will be faced with a serious problem. A scheduled vacation of a couple of weeks allows for injections to be prepared in advance, but an unexpected or prolonged loss of this specially trained person may seriously impact the practice.
There is only one solution to this problem: fully train a second allergy care provider. This may be either another full-time member of the staff or a part-time employee. The expense of formal training must be borne by the physician, but the on-the-job portion may be provided by the primary allergy care provider. In most practices, it will not be long before this second person is active a good deal of the time, assisting the primary person in vial making and giving treatment injections and filling in during absences. This is the flexibility benefit alluded to previously. Both allergy care providers could be part-time employees, but having someone in the office full-time, to answer questions on the phone and provide the continuity of care the allergy patient has come to expect, is highly desirable. One of the benefits of an allergy practice is continuity of patient flow, as opposed to the fluctuations of a primarily surgically based practice. This benefit should be protected.
PAPER GOODS
Informational Literature
Time is an essential ingredient of allergy care. The condition is an ongoing one, and if good results are to be obtained, the patient must interact with both the directing physician and the allergy caregiver. Questions come up repeatedly and must be answered. To accomplish this in a manner consistent with the demands of an otherwise busy practice, as much use as possible must be made of informational material that the patient may study at leisure. Several pamphlets are available from the AAO-HNS and the AAOA. These are inexpensive and provide the patient with something to take home, which is also a good advertisement for the practice. Many books and monographs on allergy are available to the lay public. Most are good sources of information. The Internet is also replete with information, some good, some obviously self-promoting. A caveat must be expressed here, however. There are today a variety of approaches to allergy care, all of which are effective to varying degrees. Despite efforts to maintain an objective approach to the different formats, many publications tend to denigrate any approach except that practiced by the originator of the publication. This often results in a patient questioning the expertise of the practitioner. Many patients do not realize that this diversity of opinion is common in the field of medicine. If a patient asks about a specific publication or information on an Internet site, it is a wise precaution for the practitioner to check the source personally and to be prepared to counteract any adverse comments therein. Of course, this requires that the practitioner be knowledgeable and practicing well within reasonable, self-imposed limitations. It is regrettable, however, that the field of medicine should ever become involved in the type of vindictive attack frequently seen in print, or the self-promotion (at the expense of others) of some Web sites.
One additional printed source of information should be made available to the patient: a booklet describing exactly how allergy care is delivered in this allergy practice, including what the patient may expect in the way of tests and treatment, how payment is to be handled, and answers to commonly asked questions. As the patient load increases, new editions of the booklet can address new issues and questions that arise. This material will prove invaluable as a teaching tool for the patients and as a time saver for the staff, as it saves the staff from having to answer the same questions repeatedly and it serves as a reference for patients to help them remember what they have been told. It is helpful to deliver the initial printed information within a folder that has pockets into which future material may be placed, so that the patient can easily find and refer to it.
Allergy Records
In allergy care, as in all areas of medicine, detailed record keeping is necessary. Because allergy care involves multiple brief visits, both for testing and for treatment, multiple notations must be made on the patient’s record. Fortunately, most (though not all) of these will be brief. Because allergy care is ongoing, often for years if immunotherapy is elected, it is important that allergy records be easily understood by any trained physician providing care, in case the patient changes allergists (because of moving out of the area or because of managed care issues). It has been an unfortunate experience that many records prove to be incomprehensible to other physicians. Abbreviations commonly used in one practice may be meaningless to another. (This situation may also occur within a practice if the allergy care provider uses chart notations that other staff members do not understand.)
With ever-increasing risks of litigation associated with medical care, it has been impressed repeatedly on physicians that all records should be easily comprehensible to anyone in need of reviewing them. This holds equally true for allergy records. Here, however, some specific problems may arise.
It has long been recognized that there are several schools of allergy with different beliefs and methodologies of achieving results from immunotherapy General allergists are trained based on the format of the American Academy of Allergy, Asthma, and Immunology, a conjoint board of internal medicine and pediatrics. Otolaryngic allergists are trained based on the format of the AAOA. The latter organization is a subspecialty group recognized by the American Medical Association, with representation in its House of Delegates, and has long been the driving force in otolaryngic allergy activities. The differences between the two schools are not in beliefs but rather in the logistics of the therapeutic approach to testing and treatment (see Chapters 5 and 8). Therefore, the documentation of testing and treatment differs.
Because the authors of this book include four otolaryngic allergists and an otolaryngic allergy nurse, the approaches described here are primarily those of the otolaryngologist. This specialty has dedicated itself to providing the training and material necessary for physicians of any background who are planning a limited allergy practice to perform this service in a competent manner. The concept of the regional specialist has long been espoused by practitioners of otolaryngology, and the inclusion of allergy care in the physicians armamentarium is no exception. The American Board of Otolaryngology requires that allergy be a part of the training program for residents in the specialty. Although “turf battles” between the two groups continue, unless radical restrictions are placed on allergy care by managed care programs, there will continue to be an ample number of patients to keep competent practitioners in both specialties well occupied.
Allergy records, both for testing and treatment, should be easily understood by any other practitioner using the same format. Fortunately, basic skin testing forms and treatment record forms are available from allergy supply houses, and the AAOA encourages all those receiving training under its auspices to use the same forms. Appendix 3 includes an example of a typical allergy history and an IDT form that can be modified or individualized on a computer to meet the needs of the practice. It is necessary to insert the individual allergens to be tested in the appropriate locations. Each region of North America (and elsewhere) will have different allergens.
It is especially important to document the exact contents of each treatment vial. This documentation may determine whether another physician taking over the care of the patient will be willing to accept the stage of treatment the patient has reached and continue previously successful therapy, or will demand a complete retest and new escalation of treatment. If the physician insists on this second approach, there will be a considerable delay in bringing the patient to maintenance levels. Of course, if the patient is not doing well, new testing may be indicated, regardless of who is providing the care.
Most testing forms include a section indicating the makeup of the initial treatment vial. As the dose is escalated to progressively stronger levels, the contents of each treatment vial must be fully documented. The source of the antigen (i.e., the laboratory supplying the extract) should also be documented; this is extremely important when records are transferred. The expiration date of the treatment vial should always be recorded. Recording all this information may save the patient extensive repetitions of previously successful immunotherapy, with no guarantee of an equally good result. When a transferred patient is doing well, it is wise to make as few changes in therapy as possible. This is considered in more detail in Chapter 8, along with appropriate sources of antigen for a patient who is transferred and appropriate safety checks and controls.
SELECTION OF ANTIGEN FOR THERAPY
After the physical necessities for providing allergy care and the personnel who will be utilizing them have been acquired, it is necessary to consider the specific antigens needed for treatment. Today, the number of antigens available from reputable supply houses is almost unlimited. The physician looking at a catalog of antigens and supplies for the first time may experience a moment of panic: How is it possible to select appropriate antigens for the practice from so large a list? How many will actually be needed? This can be a daunting experience.
As an aside, it is precisely the great number of available antigens that resulted in the reluctance of third-party payers to provide coverage for allergy care for a large number of patients, especially in the early days of in vitro testing. In the past, some programs were developed in which any physician, regardless of training, could send blood to a reference laboratory for specific testing, and have an antigenic vaccine returned with instructions for administering immunotherapy. This “remote practice of allergy” approach, in which a distant authority makes clinical decisions, has been decried by both otolaryngic and general allergists, and is discussed later in this chapter. There was a strong possibility in this system to perform tests for an immense number of allergens, thus running up a huge bill that third-party payers would in turn reject. The package produced a generation of untrained physicians dubbed “venipuncture allergists,” a group not accepted by any school of physicians dedicated to providing good allergy diagnosis and care. This approach seriously damaged the acceptance of in vitro testing as a cost-effective approach to allergy diagnosis, and left a damaged image for the basic procedure that still exists today to some degree, despite evidence that in vitro testing, properly performed, is in fact quite cost-effective.1
The venipuncture allergists received the greatest publicity for allergy care abuse, and because of this they have largely disappeared. It has been common for other allergists employing skin testing of some variety, however, to augment significantly the number of tests actually indicated for allergens needing to be investigated. The mere availability of an immense number of allergens does not indicate that such a number should be in the armamentarium of the clinician. All, or even a large percentage, are not needed to provide good diagnosis and care. A geographic, seasonal, and personal analysis by history will provide a good list of allergens that should be available to the practitioner, and determine how many should be used in the initial testing of any one patient.
Regional Allergens
Not all allergens are present in all locations in North America. It is rare to have more than 30 to 40 inhalant allergens of any significance in any one locality. The new practitioner may not find it necessary to have even this large a number immediately available, as more can easily be added when necessary. What is needed is a determination of the major allergens so that initial testing can be performed, allowing the physician to be prepared to offer treatment for the significant offenders in a timely manner. Acquiring this information requires a critical look at the area, specific exposures, and the individual patient. Initial testing should involve a screening evaluation of up to 14 antigens, and from this information it can be determined whether additional testing is likely to be fruitful.
For practical purposes in selecting appropriate allergens and evaluating the patient’s history, allergens are divided into seasonal and perennial groups. Both need to be considered in selecting a supply of allergens for care, and in deciding which to test for in any one patient.
Seasonal Allergens
Seasonal allergens are those that produce the symptoms usually recognized by the lay public as “hay fever.” These are represented primarily by pollens. Actually, pollens often do not constitute as serious a problem as other allergens, not because of any lack of severity of symptoms but because of the short duration of their presence in the air. The patient sensitive to only a specific group of pollens present during a single season may often be treated with a less definitive approach than immunotherapy with good results, if the patient so desires. The tendency of allergy, however, is to become worse when untreated. The usual pattern seen in a patient becoming allergic is an initial complaint of symptoms during a specific season, such as fall, and an expansion of symptoms as the years progress to occur also in the spring, then the summer, and finally all year round. Thus, seasonal symptoms warrant investigation if the patient is interested in a definitive approach to care.
Although it might seem more likely that a patient would elect a simple medical approach to allergic symptoms when time is limited, the fact is that most patients presenting in the physician’s office for care are interested in immunotherapy. With the wide range of antiallergic drugs available over the counter today, most allergy sufferers have already tried several of these; they have either been satisfied, in which case they will not have made a doctor’s appointment, or have been dissatisfied, in which case they are interested in a more definitive approach, specifically immunotherapy. The treating physician, therefore, must become acquainted with the pollen allergens in the area and the degree of importance of each. This is not as daunting as it sounds.
Some allergy supply houses have available regional maps indicating the major allergenic offenders in each specific area of the country (see Appendix 2). These are of great value and should be available to the novice allergist from the start. Such maps have been developed from pollen counts in each specific area, either provided by a botanist employed by the allergy supply house or obtained from studies performed by local botanical gardens, universities, the U.S. Department of Agriculture, or private organizations. The best are those that deal with a small local area, as the overall region covered by some guides may be excessively large and subject to more variation.
The American Academy of Allergy, Asthma, and Immunology (AAAAI) makes available pollen and mold spore data from numerous counting stations. For further information, consult the AAAAI Web site: www.aaaai.org.
The veritable “bible” of regional allergens is the text by Walter Lewis, which should be consulted by those interested in the most detailed picture of each region.2 This book is a valuable addition to the allergists library. Some of the allergenic pollens Lewis recorded are not available commercially, however, and therefore cannot be used in treatment. It is for this reason that the allergy supply houses’ regional lists are a more practical source.
The best lists of regional allergens include a category noted as index allergens. These are the allergens whose extracts are in greatest demand, indicating a high degree of allergenic significance in the area. A list of such regional allergens appears in Appendix 2. The physician just starting an allergy practice might do well to begin by simply including the index pollen extracts in the treatment supply set, adding others as the need arises. If the index allergens are supplemented by allergens appearing repeatedly in local pollen counts, a good treatment base for pollens will have been established.
BLOOMING SEASONS
In North America, certain categories of plants bloom in certain seasons. The actual start and termination of the season may be affected by the latitude, prevailing winds, rainfall, and a variety of other factors of local significance, but the overall sequence of pollination remains very similar in all locations. This sequence of blooming, both over the entire country and in the local area, represents one of the things the person taking the initial and ongoing history from the patient must keep constantly in mind, as opposed to other factors that may be researched when needed. The patient s response to the blooming seasons of various categories of plant indicates whether the problem is a seasonal or a perennial one, which will affect both the testing to be performed and the treatment plan; if the problem appears to be seasonal, the response also indicates which category of plant should be tested. Testing plants that bloom in a season in which the patient is symptom free is likely to result in confusion.
The overall pattern of the blooming season in North America is simple and clear. Trees bloom in the spring. The starting date may be affected by the local environmental factors mentioned previously, but spring is the season for most trees. The blooming season for trees may last from 6 to 12 weeks, depending on the area of the country. Rarely do trees continue to bloom into the summer months. There are exceptions to this rule, and the allergy team must be aware of them as they apply in the specific area. Elm trees may start to pollinate in selected areas while snow is still on the ground, and they may pollinate again in the fall. Mountain cedars typically bloom during winter.
Grass is the summer offender. As with trees, the start of the blooming season varies, and in some subtropical areas grass blooms all year, but even there the blooming season is concentrated in the summer. Grass is an offender of major importance, as it is a highly potent allergen easily capable of inducing anaphylaxis. Our knowledge of grass pollen as an allergen goes back to the earliest investigations into the nature of allergy. Charles Blackley3 in 1873 used grass pollen to demonstrate the parallel between skin reactivity and hay fever symptoms, and Leonard Noon4 in 1911 used grass pollen, an extract of timothy (known at the time as Ph/eum), to establish the original Noon unit of allergy, the first quantification procedure for allergic sensitivity.
The grass-blooming season, like the tree-blooming season, usually lasts about 6 to 12 weeks in most temperate regions. The later stages of blooming may well overlap the start of the weed season.
Fall is the weed-blooming season. This may start as early as July in some warm areas of the United States, but usually occurs from mid-August to the first frost. Weeds are widely known for their allergenic effects. In much of the United States, especially the northeastern part, ragweed is the key offender, so much so that ragweed is used as the index plant in the majority of allergy studies. Ragweed is far from the only offender, however. The range of weeds of allergenic significance is discussed later in more detail, and still more information can be obtained from examining regional and seasonal charts as presented in Appendix 2 and provided by allergy supply houses.
Winter in most of North America shows little in bloom. Most people spend most of their time indoors, with the heat on. The primary winter offender, therefore, is likely to be dust. Dust is a mixture of many items, and cannot realistically be considered a seasonal allergen. Details of perennial allergens, including dust, are discussed later in this chapter.
Seasonal allergens are members of the group that has been the subject of the most extensive study. Pollens lend themselves to more objective examination than many other allergens. All inhalant allergy appears to be immunoglobulin E (IgE) mediated, and as such the specific allergens in each pollen extract may be identified. The details of this procedure are not relevant to a clinical discussion, however. The clinician faces a large enough problem in selecting allergenic extracts pertinent to the practice. A brief presentation of the method used to determine IgE-mediated cross-reactivity appears at the end of the section on cross-reactivity (see later in this chapter), but this is for information only and is not essential to the clinical part of a practice.
THOMMEN’S POSTULATES
Not all pollens present a significant allergenic problem. It is probable that the majority of pollens are not significantly allergenic. Aware of the difficulty in evaluating all pollens as possible offenders, Thommen, in conjunction with Coca and Walzer, in 1931 described a group of requirements to be satisfied for a pollen to be considered an allergenic offender. These requirements (known as Thommen’s postulates) are as follows:
1. The pollen must be wind-borne.
2. The pollen must be produced in large quantities.
3. The pollen must be buoyant enough to be carried by the wind for considerable distances, with a diameter between 15 and 58 μm.
4. The plant must be abundantly distributed, or habitually grown close to human habitation.
5. The pollen must be allergenic.



