FIGURE 3-1. Keratoacanthoma. A. Lesion of the left upper eyelid that grew over 2 to 3 weeks. It was excised without recurrence. B. Large lesion of the left lower eyelid in a 40-year-old patient. The appearance could be that of a squamous cell carcinoma; however, the history of growth over 4 weeks and the patient’s younger age point to a keratoacanthoma. This lesion was excised without recurrence.
ACTINIC KERATOSIS
These lesions may be single or multiple on chronically sun-exposed skin. They appear as dry, rough, scaly lesions that are stable but can rarely disappear spontaneously.
Synonym: solar keratosis.
Epidemiology and Etiology
• Age: Older than age 40; rare younger than 30 years
• Gender: Higher incidence in males
• Etiology: Sun exposure over time in a fair-skinned white population results in actinic keratosis.
History
• Extensive sun exposure in youth
• Lesions present for months.
Examination
• Rough, slightly elevated, skin-colored or light brown lesions with hyperkeratotic scale (Fig. 3-2)
Special Considerations
• It is estimated that one squamous cell carcinoma will develop per 1000 actinic keratoses.
Differential Diagnosis
• Squamous cell carcinoma
• Discoid lupus
Laboratory Tests
• Pathologic evaluation if biopsied
Pathophysiology
• Repeated solar exposure results in damage to the keratinocytes by the cumulative effects of ultraviolet radiation.
Treatment
• Prevention through early and lifelong use of sunscreen
• Excise nodular lesions and submit for pathologic evaluation.
• Most flat lesions respond to liquid nitrogen or topical application of 5% 5-fluorouracil cream over a few days to weeks.
• Topical imiquimod cream has also been approved for treatment of actinic keratosis.
• These three treatments (liquid nitrogen, 5-fluorouracil, and imiquimod) must be used with caution around the eye and should be avoided in lesions at or near the lid margin.
Prognosis
• Some actinic keratoses may disappear spontaneously but others remain for years unless treated.
• Incidence of squamous cell carcinoma developing in these lesions is unknown but has been estimated to be one squamous cell carcinoma in every 1000 actinic keratoses.
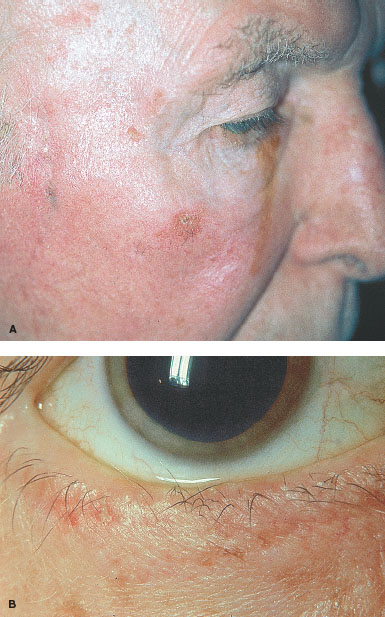
FIGURE 3-2. Actinic keratosis. A. Multiple actinic keratoses on the cheek and brow with signs of chronic sun damage. B. Lesion involving the lower eyelid. (Courtesy of Jurij Bilyk, MD.)
LENTIGO MALIGNA
Lentigo maligna is a flat intraepidermal neoplasm and the precursor lesion of lentigo maligna melanoma. The lesion has striking variations of brown and black (Fig. 3-3), often described as a “stain.”
Epidemiology and Etiology
• Age: Median age is 65 years
• Gender: Equal incidence in males and females
• Etiology: Sun exposure is a definite factor.
History
• History is usually not helpful, as exact onset of lesion is unclear.
Examination
• Flat, dark brown or black color, sharply defined edges
• Often appears like a dark “stain” on the skin
Special Considerations
• This is a premalignant lesion and should be excised because of the chance of development into a lentigo maligna melanoma.
Differential Diagnosis
• Seborrheic keratosis
• Actinic keratosis
• Malignant melanoma
Laboratory Tests
• Histopathologic evaluation
Treatment
• Excision with margins sent for pathologic evaluation
Prognosis
• Excellent if excised before developing into a melanoma

FIGURE 3-3. Lentigo maligna. A. A large macule with irregular borders and different shades of brown. (From Fitzpatrick TB et al. Color Atlas & Synopsis of Clinical Dermatology, 4th ed. New York, McGraw-Hill, 2001.) B. Recurrent lentigo maligna of left brow.
BASAL CELL CARCINOMA
Basal cell carcinoma is the most common type of skin cancer. It is locally invasive and aggressive but has very limited capacity to metastasize. If neglected, it can invade the orbit, especially if located in the medial canthal area. Most commonly, it occurs on the lower eyelid and is treated by complete surgical excision.
Epidemiology and Etiology
• Age: More than 40 years of age. Rare cases do occur in the 20s and 30s
• Gender: Males more than females
• Etiology: Sun exposure and fair skin with poor ability to tan are risk factors. Treatment with x-ray (for acne) increases the risk.
• Incidence: 500 to 1000 per 100,000 people
History
• Slowly enlarging lesions in sun-exposed areas
• The lesions may be associated with bleeding.
Examination
• Round or oval, firm lesions with depressed center
• The lesions are pink or red with fine thread-like telangiectasia.
• The center may be ulcerated. Basal cell carcinoma may also appear scar-like or be cystic (Fig. 3-4A–D).
Special Considerations
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


