FIGURE 28.1 Flat-mount mouse retina (wild type) shows vascularization to the periphery. The retina of the mouse, which does not express TGF-β in the eye, shows an avascular peripheral retina similar to FEVR. If left alone, the eyes progress to develop retinal detachment.
Although genetic diagnostic tests only identify a portion of mutations associated with FEVR, referral of patients to a clinical geneticist for counseling is recommended. After obtaining a thorough family and medical history, the clinical geneticist may be able to provide information about research laboratories that would be helpful to the patient as well as make recommendations for family member testing and family planning.
The clinical diagnosis often is made by the examiner saying, “This looks like ROP, but the child was full term.” The features of FEVR include areas of avascular peripheral retina and findings of vascular buds at the junction of the avascular and vascularized retina, as well as dragged vessels (Fig. 28.2) in the posterior pole and retinal folds (Fig. 28.3), which can be in contact with the lens. Large amounts of subretinal exudate can be present, and total retinal detachment due to exudative and proliferative forces can be seen (Fig. 28.4). Histologically, inflammatory elements are found that may support the proliferative process (18). A positive family history also may be helpful in making a diagnosis. However, the lack of a diagnosis of FEVR in family members does not rule out a diagnosis of FEVR; for example, in one study no family history was found in 55% of cases (16). In addition, FEVR shows variable expression (e.g., mild avascular peripheral retina without significant exudate or detachment) and incomplete penetrance (mutation present but asymptomatic). Therefore, if the diagnosis of FEVR is suspected, a thorough peripheral retinal examination including fluorescein angiography should be recommended for family members.
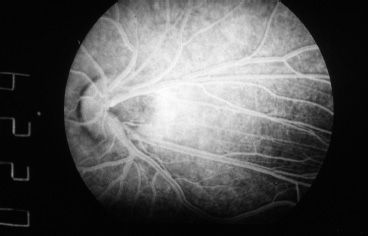
FIGURE 28.2 Fluorescein angiographic image showing the dragged vessels of the posterior pole. This is often seen in FEVR but also presents in other pediatric retinal diseases. Note the temporal dragging of the nasal vessels before they course nasally.
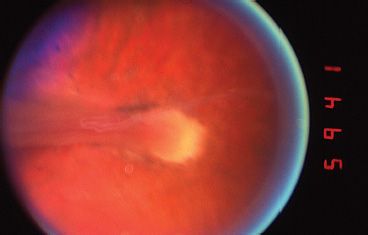
FIGURE 28.3 Now tightly dragged retina fold. Note that the retinal vessels are drawn into the fold, and there are large areas of attached avascular retina. What appears to be optic nerve tissue is actually the retina being dragged across the nerve.
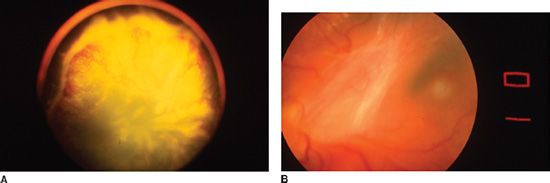
FIGURE 28.4 A: Wide-angle photograph of an eye affected by severe FEVR with avascular peripheral neovascular buds, subretinal exudate, and shallow total retinal detachment. This eye shows a predominantly exudative retinal detachment. B: Eye with organized Vitreous causing a predominantly tractional retinal detachment in this area, with a resultant retinal fold.
As mentioned earlier, the presentation of FEVR can be variable, and a classification system that somewhat parallels the International Classification of Retinopathy of Prematurity has been proposed. The FEVR classification system has five stages (Table 28.1). The classification system ranges from avascular periphery alone to total retinal detachment with and without active exudation.
TABLE 28.1
Clinical classification of familial exudative vitreoretinopathy
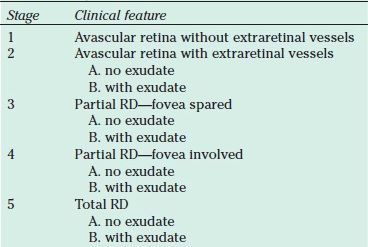
RD, retinal detachment.
The bilateral and unilateral features of FEVR have been used and can be helpful for diagnosis. In one series, 85% of eyes were bilaterally involved and 15% were unilaterally involved (16). Bilaterally involved patients need not be symmetrical (both eyes with the same stage). One eye can be severely involved with great exudation whereas the other eye can be at a more minor FEVR stage. The diagnosis often is made by examining the less involved eye, because the features for diagnosis may not be recognizable in the more involved end-stage eye. In addition, careful examination of newborns can be helpful in identifying involved eyes at earlier stages. As in most pediatric retinal diseases where severe retinal detachment can occur, if both eyes are involved, the more involved eye is often smaller than the less involved eye. Fluorescein angiography has been performed in FEVR but is not needed to make the diagnosis (19). Fluorescein angiography, however, will frequently reveal bilateral disease in a fellow eye that does not demonstrate abnormalities on exam.
The FEVR patient population is characterized by a spectrum of disease presentation, including range of age at presentation, gestational age, and birth weight. FEVR eyes that present in the first year of life have a much worse prognosis. Benson (3) noted that children who presented in the first 3 years of life had a worse prognosis. However, in our opinion, presentation in the 1st year of life is even worse. Children often present because of reduced visual attention, strabismus, or leukocoria. Retinal folds are seen in approximately one-third of FEVR eyes. The majority of retinal folds extended radially in the temporal quadrants, but radial folds were seen in almost all quadrants. Fellow eyes demonstrated a wide variation in symmetry (20
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


