2 Otology Section Editor Contributors Week 6: Hillocks of His form from condensations of the first and second branchial arches. The first three hillocks are attributed to the first arch, and the second three hillocks are attributed to the second arch (Table 2.1). Week 20: Adult configuration is achieved. Week 8: Ectoderm of the first pharyngeal groove (cleft) invaginates. Epithelial cells then grow as a solid core toward the middle ear. The cord dissolves at 20 to 21 weeks, and is complete by week 28. Medial epithelium forms the lateral surface of the tympanic cavity; lateral epithelium forms the skin of the bony external auditory canal (EAC). The EAC might not reach final adult size and shape until the early teenage years. Week 3: Endoderm from the first pharyngeal pouch forms the tubotympanic recess. This will become the middle ear and eustachian tube. Pneumatization begins at 10 weeks. The tympanic membrane (TM) forms after the canalization of the EAC. The outer layer is first groove endoderm, the fibrous layer is first arch mesoderm, and the innermost mucosal layer is first pouch endoderm. Week 4: Mesenchyme from the first and second branchial arches fuses and begins to form the malleus and incus. The first arch is referred to as Meckel’s cartilage, and the second arch is referred to as Reichert’s cartilage. The cartilaginous ossicles form adult size and shape by week 16. They then ossify by endochondral bone formation (Table 2.2). Reichert’s cartilage also goes on to form the stapes blastema between weeks 4 and 5, which gives rise to the stapes suprastructure. The footplate is of otic capsule origin.
2.0 Embryology and Anatomy of the Ear
Embryology
Auricle
External Auditory Canal
Middle Ear
Hillock | Arch | Auricular Structure |
|---|---|---|
1 | 1 | Tragus |
2 | 1 | Crus of helix |
3 | 1 | Helix |
4 | 2 | Crus of antihelix |
5 | 2 | Antihelix |
6 | 2 | Antitragus and lobule |
Note. There remains some controversy regarding the final contributions of hillocks 4, 5, and 6.
Cartilage | Arch | Ossicular Structure |
|---|---|---|
Meckel | 1 | Head and neck of malleus, body and short process of incus |
Reichert | 2 | Manubrium of malleus, long process of incus, stapes suprastructure |
Note. The manubrium of malleus never completely ossifies.
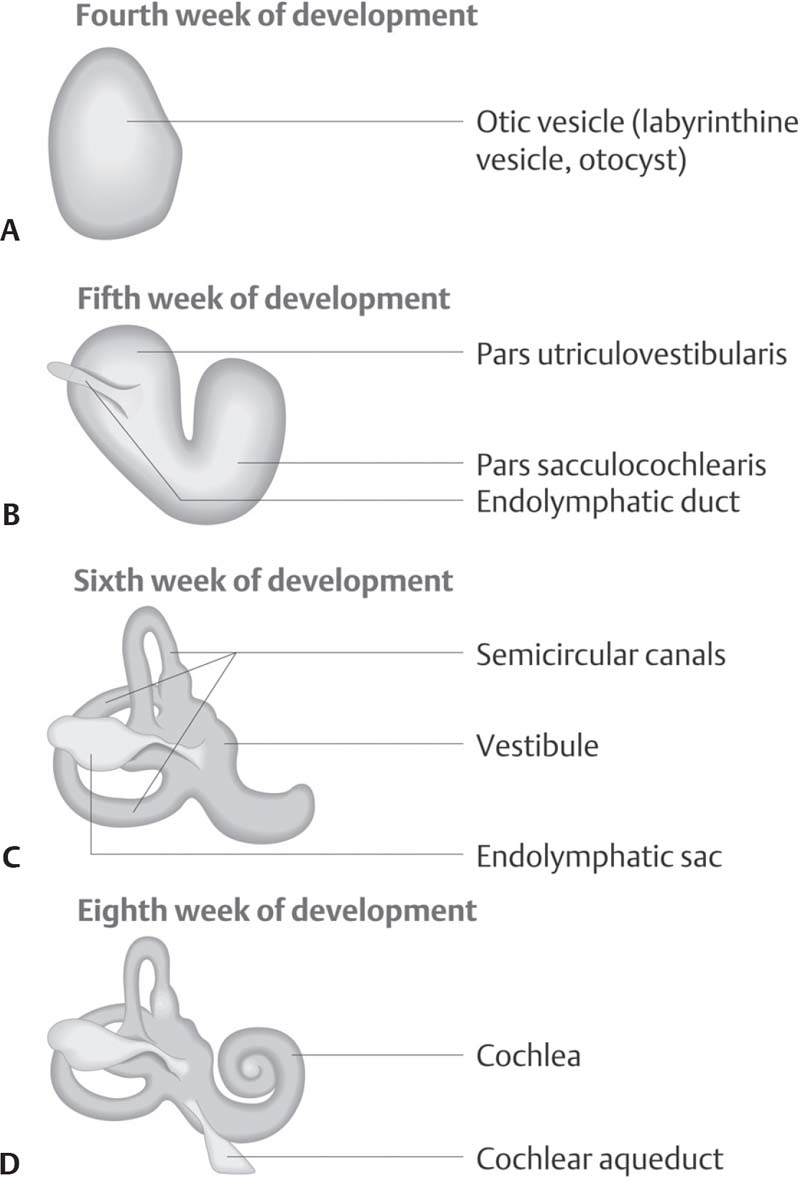
Fig. 2.1 Embryology of the inner ear. The otocyst forms from an epithelial thickening between the cutaneous ectoderm and neural groove in the third and fourth weeks of embryonic development. (A) This thickening invaginates and closes off to form a separate vesicle. (B) In the fifth week, the otocyst becomes infolded, forming the upper pars utriculovestibularis and the lower pars sacculocochlearis. (C) In the sixth week, the three semicircular canals form from the pars utriculovestibularis. (D) In the seventh to ninth weeks, the cochlear duct forms as a tubular extension of the pars sacculocochlearis and becomes coiled. (From Probst R, Grevers G, Iro H. Basic Otorhinolaryngology: A Step-by-Step Learning Guide. Stuttgart/New York: Thieme; 2006:158.)
Inner Ear
Week 3: The otic placode forms from ectoderm of the first pharyngeal groove. It invaginates and is completely encircled in mesoderm and termed the otocyst by week 4. The pars superior (semi canals and utricle) develops prior to the pars inferior (saccule and cochlea). The membranous labyrinth is complete by week 15 or 16. Ossification occurs between weeks 20 and 25 (Fig. 2.1).
Anatomy
Auricle
The auricle, with the external auditory canal known as the external ear, is made of elastic cartilage with perichondrium and skin tightly adherent anteriorly and loosely adherent posteriorly (Fig. 2.2). It is attached to the head by the extension of cartilage into the ear canal and an anterior, superior, and posterior ligament, and an anterior, superior, and posterior muscle.
External Auditory Canal
The EAC is one-third cartilaginous laterally and two-thirds osseus medially. The cartilage is fibrocartilage, not elastic cartilage. The skin over the lateral one-third is thick with hair follicles, sebaceous and ceruminous glands. The medial skin is thin without any adnexal structures or subcutaneous tissue. It is the only site in the body with skin directly onto periosteum, and is extremely pain sensitive. The canal is innervated by contributions by the trigeminal nerve (cranial nerve [CN] V, auriculotemporal branch), the cervical plexus (C3, great auricular nerve), the vagus nerve (CN X, Arnold’s nerve) and the facial nerve (CN VII). C2 and C3 also form the lesser occipital nerve, which helps innervate the anterior and posterior inferior surface of the auricle, but not the canal.
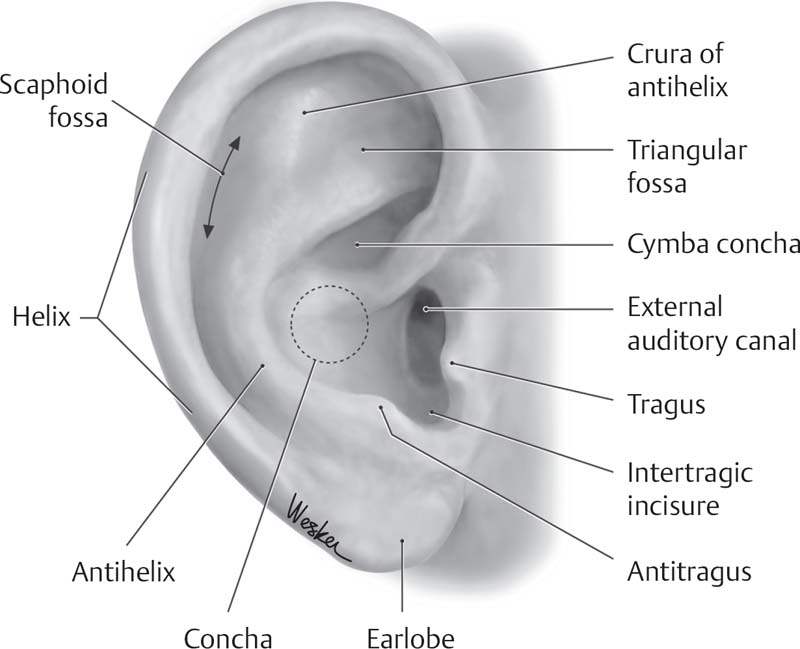
Fig. 2.2 Anatomy of the auricle. (From THIEME Atlas of Anatomy, Head and Neuroanatomy, © Thieme 2007, Illustration by Karl Wesker.)
Middle Ear
The tympanic membrane is made up of three layers. From lateral to medial: squamous epithelium, a radiating and circular fibrous layer, an inner mucosal layer. It is ~10 mm in height and 9 mm in width. Circumferentially, the fibrous annulus sits within the bony annulus, but is discontinuous superiorly at the notch of Rivinus. Inferiorly to the notch of Rivinus, the TM has a well-organized fibrous middle layer, and is known as the pars tensa. At the level of the notch of Rivinus and above, the middle fibrous layer is less well organized, and is known as the pars flaccida. Prussak’s space is at the level of the pars flaccida, bounded laterally by the TM and medially by the neck of the malleus. It is a frequent site of retraction and cholesteatoma formation.
The boundaries of the middle ear space are as follows:
• Lateral: tympanic membrane
• Superior: tegmen
• Inferior: jugular dome
• Anterior: carotid canal, eustachian tube
• Posterior: mastoid via facial recess or retro facial cells
• Medial: cochlear promontory and labyrinthine wall
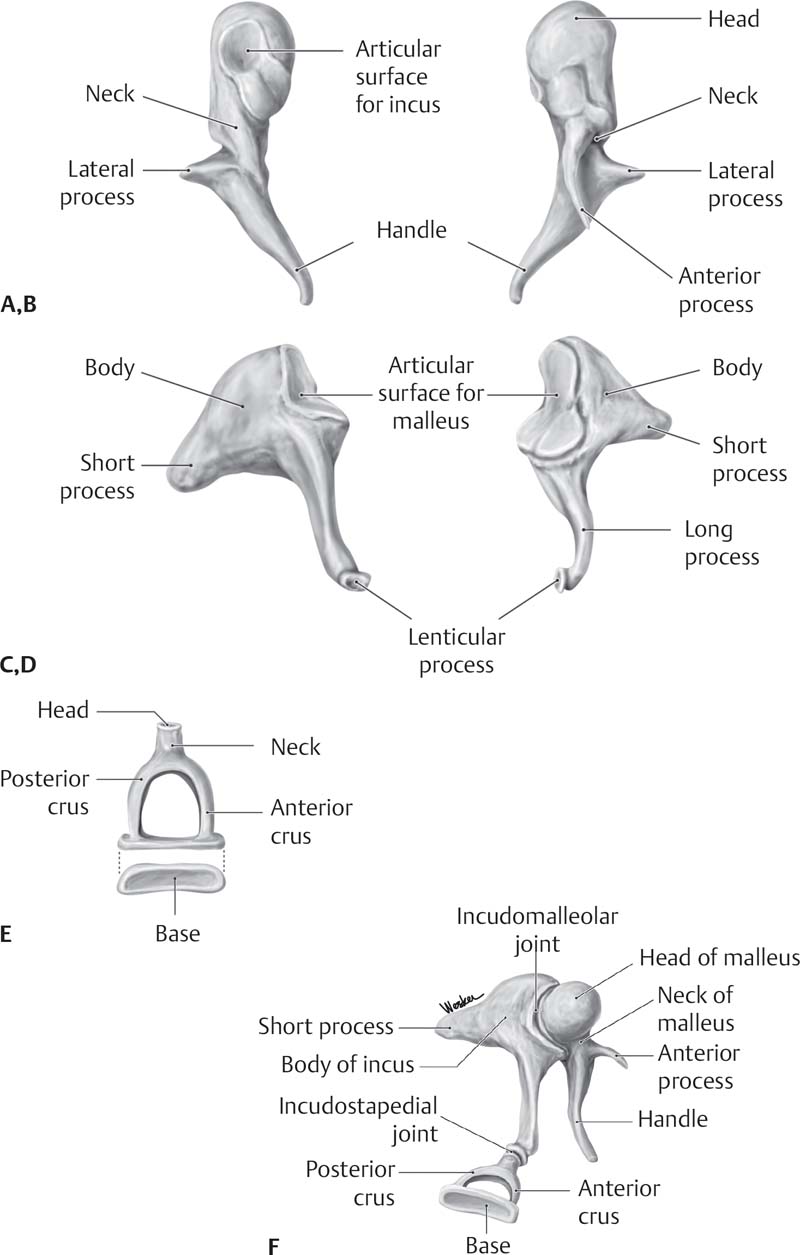
Ossicles (Fig. 2.3)
The malleus consists of a manubrium, anterior and lateral processes, neck and head. It is incorporated into the TM from the lateral process to the tip of the manubrium (umbo). The tensor tendon runs from the cochleariform process of the middle ear to the medial surface of the neck and manubrium of the malleus.
The incus is the largest ossicle, and articulates with the malleus head in the epitympanum. It has a body and short, long, and lenticular processes. The short process is held in place by the posterior incudal ligament.
The stapes is the smallest ossicle, and articulates with the incus at the lenticular process. It has a capitulum, anterior and posterior crus, and a footplate. The stapedius tendon runs from the pyramidal eminence to the posterior surface of the capitulum, or the posterior crus. Both incudomalleolar and incudostapedial joints are synovial diarthrodial joints. The footplate is kept in position by the annular ligament.
Eustachian Tube
It measures ~18 mm at birth, and 35 mm in adulthood. It is one-third bony laterally at the anterior mesotympanum, and is lined with ciliated cuboidal epithelium. Two-thirds of the eustachian tube is cartilaginous as it travels medially to end at the torus tubarius of the nasopharynx, and this portion is lined with pseudostratified columnar epithelium. It functions to ventilate, clear secretions from, and protect the middle ear. At rest it is closed, and its primary dilator is the tensor veli palatini muscle (CN V).
Inner Ear
Bony Labyrinth
The vestibule is the central chamber. Its medial wall has two depressions. Posterosuperiorly is the elliptical recess for the macula of the utricle, and anteroinferiorly is the spherical recess for the macula of the saccule. The vestibular aqueduct contains the endolymphatic duct, and enters posteroinferiorly.
The cochlea lies anteriorly. It is a 32-mm canal that rotates 2½ turns around a bony modiolus. The cochlear aqueduct contains the periotic duct.
The semicircular canals lie posteriorly. They lie at a 90-degree angle to one another, and connect to the vestibule with an ampullated and a nonampullated end. They are the horizontal (or lateral), the superior (or anterior), and the posterior canal. All of the ampullated ends enter the vestibule separately, but the posterior and superior canals fuse at their nonampullated ends to join the vestibule together at the crus commune. Superior semicircular canal dehiscence syndrome is a well-recognized entity consisting of symptoms of disequilibrium with motion, exacerbated by loud sounds, and computed tomography (CT) evidence of a bony dehiscence.
Membranous Labyrinth
The membranous labyrinth is the fluid-filled chamber within the bony labyrinth; it is surrounded by perilymph, similar to extracellular fluid (high in sodium, low in potassium), and filled with endolymph, similar to intracellular fluid (high in potassium, low in sodium).
The vestibule is filled with perilymph and holds the saccule and the utricle. Both contain gelatinous membranes coated with otoconia. They sense linear acceleration and gravity.
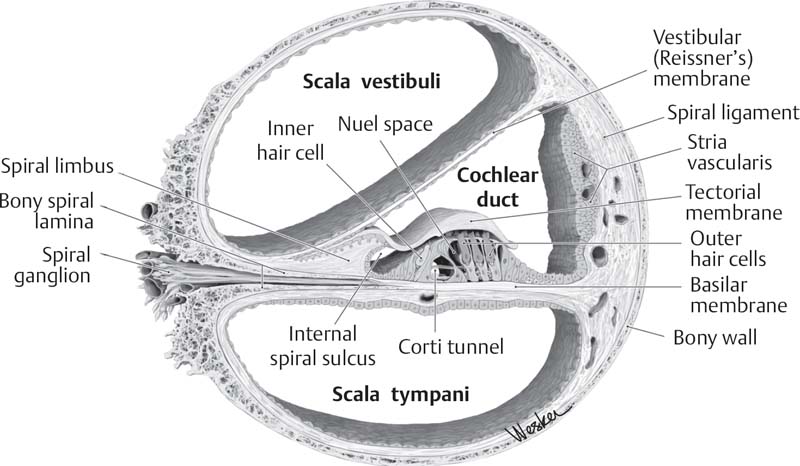
The cochlear duct mimics the bony cochlea in size and shape (Fig. 2.4). It is also known as the scala media, and is filled with endolymph and contains the organ of Corti. Superiorly is the scala vestibuli, and inferiorly is the scala tympani, both filled with perilymph and joined at the helicotrema of the cochlear apex.
Semicircular Ducts
The semicircular ducts are within the semicircular canals. Each has an ampullated end with a crista that sends hair cells into a gelatinous cupula to sense angular acceleration. The horizontal canal lies 30 degrees from the true horizontal.
The endolymphatic duct lies medial to the crus commune and opens into the vestibule. It leads to the endolymphatic sac that lies within the dura of the posterior fossa adjacent to the temporal bone.
The cochlear aqueduct runs from the basal turn of the cochlea to the subarachnoid space.
Internal Auditory Canal
The internal auditory canal is the bony channel from the posterior fossa that houses the facial nerve, the cochlear nerve, and the vestibular nerves. It starts medially at the porous acusticus, and runs laterally to end at the fundus. At the fundus, it is split horizontally by the falciform or transverse crest. The superior portion of the canal above the falciform crest is then split again into an anterior and posterior compartment by the vertical crest or Bill’s bar.
Further Reading
Gulya AJ. Anatomy and embryology of the ear. In: Hughes GB, Pensak ML, eds. Clinical Otology. 3rd ed. Stuttgart/New York: Thieme; 2007:3–34
Schuenke M, Schulte E, Schumacher U. Thieme Atlas of Anatomy: Head and Neuro-anatomy. Stuttgart/New York: Thieme; 2007
Van de Water TR, Staecker H. Embryology of the outer, middle, and inner ear. In: Van de Water TR, Staecker H, eds. Otolaryngology: Basic Science and Clinical Review. Stuttgart/New York: Thieme; 2006:251–258
2.1 Otologic Emergencies
2.1.1 Sudden Hearing Loss
Key Features
• There is a rapid onset of hearing loss with no obvious explanation.
• Audiogram and tests to rule out identifiable causes are essential.
• Treatment (steroids) must be instituted as early as possible, preferably within 2 to 3 weeks.
Sudden sensorineural hearing loss (SNHL) represents a true otologic emergency. The probable underlying causes are thought to be viral infection or a microvascular occlusive, traumatic, autoimmune, or other event. The current standard of care is to institute high-dose systemic steroid therapy as soon as possible. Response rates to treatment appear to drop considerably if not administered within 2 to 3 weeks of onset.
Epidemiology
Incidence is often estimated to be 1 in 15,000. This is likely an underestimate, as many patients do not seek medical care or are misdiagnosed by primary care providers. Men and women are equally affected; mean onset is middle age.
Clinical
Signs and Symptoms
Patients may present with a complaint of severely decreased hearing of rapid onset in one, or more rarely both, ears. Occasionally, an illness or upper respiratory infection may precede onset. Some patients also experience dysequilibrium, aural fullness, or tinnitus.
Differential Diagnosis
Identifiable causes of hearing loss must be excluded to diagnose idiopathic sudden SNHL. These include vestibular schwannoma, autoimmune causes, and infectious causes such as syphilis. Occasionally, a patient with preexisting moderate SNHL will present with sudden more severe loss due to acute middle ear effusion, for example, following upper respiratory infection. Also, a history for recent exposure to ototoxic drugs (such as aminoglycosides or chemotherapeutic medications) must be sought; if present, dose schedules and possible serum levels should be obtained. A history of Ménière disease should be considered.
Evaluation
Physical Exam
The examination should include a full head and neck exam, paying special attention to cranial nerves. A neurologic assessment to rule out signs of central or systemic disorder is important. On otoscopy, it is important to not overlook possible acute middle ear disease as an underlying cause for hearing loss. Also, a fistula test should be performed.
Imaging
Magnetic resonance imaging (MRI) of the brain with and without gadolinium enhancement is obtained to rule out a vestibular schwannoma or other intracranial process.
Labs
A rapid plasma reagin (RPR) test or a fluorescent treponemal antibody absorbed (FTA-ABS) test to rule out syphilis, erythrocyte sedimentation rate (ESR), rheumatoid factor, antinuclear antibody, and Lyme serology if in an endemic area or risk factors are present. The 68-kD antibody is recommended by some authors, although many have not found this to be useful. Others recommend antineutrophil cytoplasmic antibody (c-ANCA; to test for Wegener disease), complete blood count (CBC), chemistries, and thyroid function tests.
Other Tests
Audiologic assessment is mandatory. An accepted definition is at least a 30 dB sensorineural loss across three contiguous frequencies, commonly occurring within a 12-hour period. A poor word recognition score out of proportion to pure tone thresholds should raise suspicion for a retrocochlear lesion.
Treatment Options
Approximately 85% of cases are considered idiopathic. The current standard of care for treatment of idiopathic sudden SNHL is high-dose systemic steroids. Most authors recommend prednisone (1–2 mg/kg orally tapering over 2 weeks). Treatment should begin without delay. At the time of writing, there is an ongoing multicenter clinical trial to evaluate the efficacy of intratympanic steroids. Although data are lacking, many authors recommend concurrent antiviral treatment, such as acyclovir (800 mg orally five times daily for 1 week).
Outcome and Follow-Up
Follow-up audiograms to assess for recovery are obtained, usually at 2 to 3 weeks following initiation of treatment. The natural history of idiopathic sudden SNHL is that two-thirds of patients should experience some recovery without treatment, often within 2 weeks. Less-severe initial loss, shorter duration of loss, and early treatment are associated with better recovery. The presence of vertigo is associated with poorer prognosis. Auditory rehabilitation in patients who fail to recover is important, especially in children.
ICD-9 Code
388.2 | Sudden hearing loss, unspecified |
Further Reading
Gulya AJ. Sudden sensorineural hearing loss: an otologic emergency. Compr Ther 1996;22(4):217–221
2.1.2 Ear and Temporal Bone Trauma
Key Features
• Soft tissue or bony trauma
• Trauma may involve hearing, balance, and facial nerve function.
A wide range of acute injuries may involve the ear and temporal bone. These range from injury to the auricle, the external ear canal, the tympanic membrane, the ossicles, the inner ear, and the facial nerve. Fractures involving the petrous bone are associated with severe head injuries.
Epidemiology
Overall, between 14 and 22% of skull fractures involve the temporal bone. These are often associated with other serious injuries. Traumatic tympanic membrane perforations have been estimated to occur at an annual incidence of 1.4 per 100,000 persons. Lacerations, avulsions, hematomas, and thermal injuries to the auricle are common.
Clinical
Signs and Symptoms
Symptoms and signs depend on the type and extent of injury.
Auricular Injury
Blunt injury may result in local pain and swelling with auricular hematoma. Lacerations and avulsions will present with local findings. Burns to the auricle may appear mild or full thickness; underlying cartilage viability is the critical concern. The auricle is a common site of frostbite injury, which may present as a spectrum of symptoms over several weeks—from clear blistering, hemorrhagic blisters, a dry insensate wound, to blackened tissue demarcation.
Penetrating Trauma or Perforations
Foreign body, instrumentation, blunt injury, acoustic trauma, and barotrauma may all cause traumatic tympanic membrane rupture as well as middle or inner ear damage. Patients may present with pain, hearing loss, dizziness, or facial paresis.
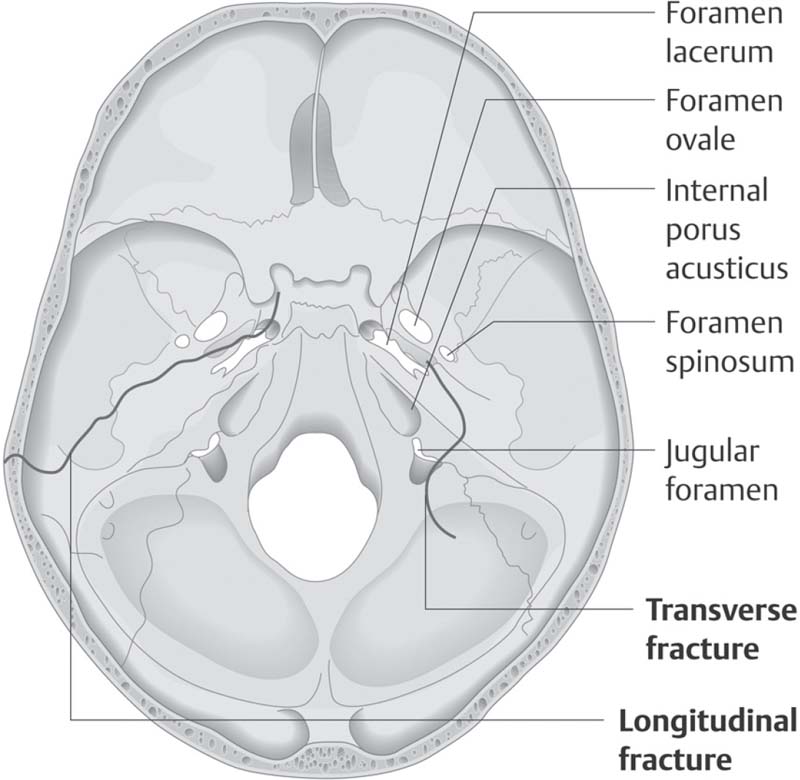
Temporal Bone Fracture
This is associated with severe traumatic head injury and the patient will present as such, requiring resuscitation, stabilization and multiteam care. Victims may present with Battle’s sign (mastoid bruise), raccoon eyes (periorbital bruising), otorrhea, hearing loss, nystagmus, and other cranial neuropathies. Fracture is classified by CT scan with respect to the long axis of the petrous pyramid: a transverse fracture crosses this axis (10–20% of fractures); a longitudinal fracture is oriented along this axis; fractures are most commonly mixed (Fig. 2.5).
Differential Diagnosis
The differential diagnosis may include soft tissue injury, an auricular hematoma, a cartilage injury, a tympanic membrane perforation, an ossicular disruption, a perilymph fistula, an inner ear injury, a temporal bone fracture, and a facial nerve injury.
Evaluation
Physical Exam
The examination should include a full head and neck exam, paying special attention to cranial nerves. In a trauma patient with severe head injury or multisystem injury, standard trauma protocol and resuscitation are performed. Life-threatening injuries (cervical spine trauma, intracranial injury, etc.) must be stabilized prior to evaluation of a temporal bone injury. With severe injuries requiring intubation and other treatment, an initial assessment of facial nerve function is important. Cleaning and examination of the ear promotes the assessment of the injuries. Initially, hearing can be assessed with 512-Hz tuning fork. Presence and type of nystagmus should be noted. When stable, temporal bone CT scanning is performed.
In the patient with more limited injury, a more focused exam is feasible. Foreign body or penetrating injuries must be evaluated under the otomicroscope. In uncooperative children, there should be a low threshold for exam under anesthesia. Ear canal injuries can be cleaned and stented if circumferential. Traumatic perforations may require surgical exploration if located in the posterosuperior quadrant and associated with severe vertigo. However, most perforations are anteroinferior and can be observed. Avoid pneumatic otoscopy.
Soft tissue injuries isolated to the auricle are treated with focused exam and emergency care. Exposed cartilage and hematoma must be recognized and treated promptly.
Imaging
High-resolution CT scanning of the temporal bone is the most useful imaging study for temporal bone trauma. Angiography is indicated with gunshot wounds to rule out vascular injury.
Other Tests
Perform an audiologic assessment as soon as feasible. Electrophysiologic testing of the facial nerve in the setting of traumatic paralysis may be helpful in terms of predicting recovery and guiding treatment decisions.
Treatment Options
Soft Tissue Injuries
Auricular lacerations must be cleaned thoroughly. Cartilage may be reap-proximated. When possible, soft tissue should be closed over exposed cartilage. If tissue is devitalized, wet-to-dry dressing coverage can be provided and surgical reconstruction planned in a delayed fashion. Antibiotics are prescribed, and Pseudomonas coverage is required.
Auricular hematomas must be drained to prevent a cauliflower deformity. To prevent reaccumulation, a pressure bolster is applied. Dental roles or rolled Xeroform (Kendall Company, Mansfield, MA) are placed on the anterior and posterior surface of the auricle and secured with 2–0 nylon in a through-and-through mattress stitch for 5 days. Antibiotics are prescribed.
Auricular burns are treated with mafenide topically. This may penetrate eschar and help to prevent cartilage loss. Infected cartilage is débrided. With a frostbite injury, avoidance of thawing and refreezing is critical. Injured areas are rapidly rewarmed and patients may benefit from ibuprofen. Ongoing local wound care is required as the injury demarcates.
Attempt at surgical reattachment of avulsions should be performed. There is a high failure rate, requiring delayed débridement and discussion of reconstructive options. Most animal bites are thoroughly irrigated, closed, and treated with oral antibiotics. Management of human bites remains controversial. Débridement, irrigation, intravenous (IV) antibiotics for 48 hours and delayed repair is advocated by some; others treat human auricular bite wounds with irrigation, immediate closure, and oral antibiotics.
Penetrating Trauma/Perforations
Ear canal lacerations should be suctioned and cleaned under the microscope. If circumferential, stenting with Oto-Wick (Medtronic Xomed, Inc., Jacksonville, FL) or Gelfoam (Pfizer Pharmaceuticals, New York, NY) for 10 days may be required to prevent stenosis. Antibiotic and steroid drops are prescribed.
Traumatic perforations in the posterosuperior quadrant with symptomatic vertigo should undergo exploratory tympanotomy due to possible stapes dislocation. At surgery, unstable bone fragments are removed and the oval window is grafted; prosthesis placement is controversial.
Traumatic perforation in other locations can be treated conservatively. Antibiotic steroid drops are prescribed, dry ear precautions observed, nose-blowing avoided, and follow-up exams planned. Vestibular symptoms are treated with antiemetics and rest. Approximately 90% of small perforations heal spontaneously. Large perforations or an accompanying infection may complicate healing and eventually require surgical repair.
Temporal Bone Fracture
If there is no facial nerve injury, from an otologic standpoint the fracture may be handled conservatively. Local wound care and follow-up audiograms are necessary. However, patients often require neurosurgical intervention for other injuries. If there is complete facial nerve paralysis, this may require surgical exploration, depending on the nature of the injury. Gunshot wounds may involve widespread injury, carrying a high incidence of severe vascular injury and high mortality rate. Cerebrospinal fluid (CSF) otorrhea or rhinor-rhea may require surgical repair via a neurosurgical or mastoid approach. Injuries with CSF otorrhea not requiring neurosurgical repair may be observed with conservative measures; a high percentage spontaneously stop. Antibiotic prophylaxis is controversial. Audiometry at 3 months should be performed to follow conductive hearing loss. Persistent conductive loss may require exploratory tympanotomy. Vestibular dysfunction is treated with rest and antiemetics; follow-up vestibular testing is performed.
Outcome and Follow-Up
For temporal bone injuries involving hearing loss, follow-up audiograms are required, as discussed above. Most traumatic perforations heal spontaneously but should be reassessed at 3 months. Benign paroxysmal peripheral vertigo is common following temporal bone injuries, and is managed with canalith repositioning exercises. For patients without hearing recovery, auditory rehabilitation options should be offered, ranging from a conventional hearing aid, a bone-anchored hearing aid, to possible cochlear implantation.
ICD-9 Code
801 | Fracture of base of skull |
Further Reading
Chang CYJ. Auricular trauma. In: Stewart MG. Head, Face, and Neck Trauma: Comprehensive Management. Stuttgart/New York: Thieme; 2005:164–168
Dinces EA, Kim HH, Wiet RJ. Evaluating blunt temporal bone trauma. In: Wiet RJ, ed. Ear and Temporal Bone Surgery: Minimizing Risks and Complications. Stuttgart/New York: Thieme; 2006:71–80
Huang MY, Lambert PR. Temporal bone trauma. In: Hughes GB, Pensak ML, eds. Clinical Otology. 3rd ed. Stuttgart/New York: Thieme; 2007:273–288
Oghalai JS. Temporal bone trauma. In: Stewart MG. Head, Face, and Neck Trauma: Comprehensive Management. Stuttgart/New York: Thieme; 2005:169–179
Swartz JD, Loevner LA. Imaging of the Temporal Bone. 4th ed. Stuttgart/New York: Thieme; 2009
Wang TD. Auricular reconstruction. In: Papel ID, ed. Facial Plastic and Reconstructive Surgery. 3rd ed. Stuttgart/New York: Thieme; 2009:821–840
2.1.3 Acute Facial Paresis and Paralysis
Key Features
• The onset of Bell palsy is rapid, within 24 to 48 hours.
• Treatment consists of high-dose prednisone plus an antiviral.
• Eye care is essential and must not be overlooked.
• Spontaneous recovery to normal or near-normal function is almost 85%.
Bell palsy, or acute idiopathic facial nerve palsy, accounts for 60 to 75% of all acute facial palsies. It is characterized by a rapid onset (24 to 48 hours), and may or may not progress to total paralysis. A facial weakness that progresses slowly over weeks to months is suspicious for a neoplasm. Treatment for Bell palsy consists of a prednisone taper (starting at 1 mg/kg) plus an antiviral for at least one week. Surgical therapy is controversial for patients meeting very specific criteria. Eye care is mandatory if eye closure is compromised (see also Chapter 7.2). If there is little to no recovery after 2 to 3 months, then imaging is recommended to rule out a neoplasm.
Epidemiology
The incidence of Bell palsy is 20 to 30 cases per 100,000 people per year. It accounts for almost 75% of all unilateral facial palsy; 40,000 cases occur in the United States each year. Median age of onset is 40, but the incidence is highest over age 70. Men and women, and right and left sides, are affected equally. Pregnant women and patients with diabetes and hypertension are at increased risk.
Clinical
Signs and Symptoms
Patients usually present with rapid-onset (24–48 hours) facial nerve weakness that may progress to complete paralysis. Patients often report pain and numbness around the ear, hyperacusis, and dysgeusia; 70% of patients will have a preceding viral illness.
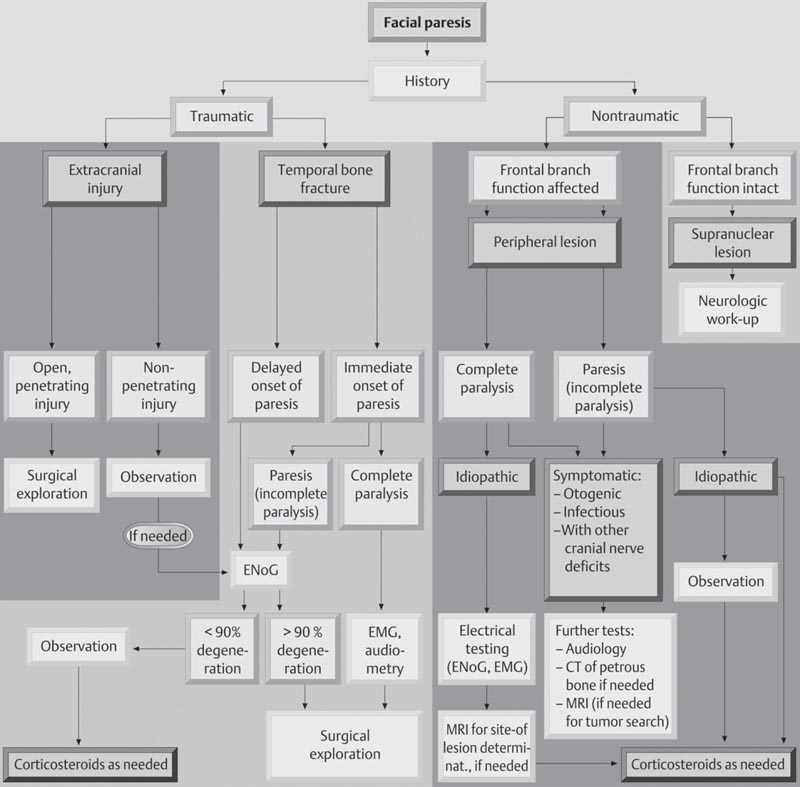
Differential Diagnosis
Idiopathic facial nerve palsy is a diagnosis of exclusion (Fig. 2.6). Herpes zoster oticus (Ramsay-Hunt) is characterized by severe otalgia and vesicular lesions involving the ear, and accounts for 10 to 15% of acute facial palsies. Melkersson-Rosenthal syndrome consists of recurrent bouts of unilateral facial palsy in association with facial edema and a fissured tongue. Facial palsy occurs in 11% of patients with Lyme disease, and may be bilateral. Acute and chronic otitis media with or without cholesteatoma can also cause acute facial palsy, as can necrotizing or malignant otitis externa. Neoplasms need to be ruled out if there is no symptomatic improvement after 2 to 3 months or if the palsy is characterized by slow onset or relapse.
Evaluation
History
The most important information is the history. Time of onset and history of previous episodes are paramount. Hearing loss and vertigo are also important to note. Patients with herpes zoster oticus are likely to experience involvement of the eighth cranial nerve (CN VIII).
Grade | Facial Nerve Findings |
|---|---|
I. Normal | Normal |
II. Mild dysfunction | Slight weakness on close inspection |
III. Moderate dysfunction | Appears normal at rest; weakness with effort but still full eye closure |
IV. Moderately severe dysfunction | Weakness visible at rest; incomplete eye closure |
V. Severe dysfunction | Only barely perceptible motion |
VI. Total paralysis | Complete paralysis |
Physical Exam
A complete head and neck examination is required. Determination is made whether facial nerve function is weak or completely absent. The House–Brackmann scale is often used for charting and physician communication (Table 2.3). If the upper face is spared, then a central etiology is suspected. The eardrum is carefully inspected to rule out acute or chronic middle ear disease, cholesteatoma, or a temporal bone neoplasm, either benign or malignant. The skin is evaluated for signs of vesicular lesions. They may be periauricular, auricular, in the ear canal, or even on the palate, and are expected to be tender and in various stages of healing. Palpation of the neck and parotid gland is crucial in ruling out an extratemporal process. The remaining cranial nerves are also examined looking for evidence for polyneuropathy. An audiogram is recommended to evaluate for a skull base process involving the internal auditory canal (IAC).
Imaging
Imaging is not routinely obtained at presentation if the history is consistent with acute idiopathic palsy. If the history is suspicious for any reason, then a magnetic resonance imaging (MRI) scan of the head with gadolinium enhancement is obtained to visualize the entire course of the facial nerve. If there is any enhancement along the intratemporal course of the nerve, a noncontrast fine-cut temporal bone CT scan will help to delineate the fallopian canal looking for dilation or erosion of the canal. If the palsy shows no signs of improvement within 3 months, many clinicians will then order appropriate imaging as described. Some clinicians will not initially image patients with paresis, but then obtain imaging if the paresis progresses to complete paralysis.
Labs
Labs are not routinely ordered. If the clinical picture does not follow that of an idiopathic palsy, or there are risk factors for other disorders then labs are ordered as indicated. Possible systemic problems to look for include auto-immune syndromes, Wegener disease, sarcoid, Lyme disease, or syphilis.
Electrical Testing
Electrical testing continues to be controversial. If a patient is evaluated within the first 2 weeks of the onset, an electroneuronography (ENoG) is obtained. It can only be done 3 days after total paralysis has occurred, and if the contralateral face is unaffected. A stimulating surface electrode is placed at the stylomastoid foramen, and a recording surface electrode is placed at the nasolabial fold. A compound muscle action potential is then recorded and compared with that recorded from the unaffected side. Changes in amplitude are calculated and interpreted as a percentage of nerve fiber dysfunction. If serial ENoGs are performed starting after day three, and the amplitude on the affected side indicates 90% loss of function, then surgical decompression may be an option. Electromyography (EMG) is also recommended in this circumstance, and surgical candidates are expected to demonstrate no voluntary action potentials within 2 weeks of paralysis.
Pathology
Similar to idiopathic SNHL, idiopathic facial nerve palsy as a symptom is likely secondary to multiple insults. Theories focus on virally mediated inflammation followed by ischemia, neural blockade, and degeneration. The inflammation leads to physical compression as the facial nerve enters the fundus of the temporal bone and forms the labyrinthine segment. This region is known as the meatal foramen and is the narrowest portion of the fallopian canal, forming a bottleneck area. Nerve conduction studies on patients undergoing decompression surgery for Bell palsy have consistently demonstrated decreased electrical responses distal to the meatal foramen. Histopathologic studies obtained from autopsy of patients who died shortly after onset of Bell palsy have been reported. The findings are similar though not uniform. Inflammatory neuritis consistent with a viral infection is most often reported, but intraneural vascular congestion and hemorrhage have also been identified.
Viral studies have shown evidence implicating herpes simplex virus (HSV) as the offending agent. Herpes virus has been harvested from nasal and oral secretions of patients experiencing an acute facial palsy. Animal models have also been used to demonstrate acute facial paralysis after intraoral and periauricular inoculation with HSV.
All of these studies are persuasive, but as of yet, not conclusive.
Treatment Options
Medical
Management of Bell palsy consists of high-dose oral steroids (prednisone 1 mg/kg start dose) with a 2 to 3 week taper, and a concurrent week to 10 days of an oral antiviral (e.g., valacyclovir 500 mg orally three times daily). The natural history of the disorder suggests that almost 85% of patients will recover normal or near normal function without treatment, but there is no test to determine outcomes at the time of presentation. Therefore, all patients are treated with the above medical regimen.
Surgical
Surgery for these patients remains controversial. Centers that see large volumes of these patients have developed algorithms that include serial ENoG testing in conjunction with EMG. If patients present within 2 weeks of onset of paralysis, and reach >90% facial nerve degeneration without evidence of EMG action potentials, they are offered middle fossa facial nerve decompression. The middle fossa route enables complete decompression of the labyrinthine portion of the facial nerve, including the meatal foramen, without sacrificing hearing. Small series have shown that patients choosing decompression have a 91% chance of good recovery (House-Brackmann I or II). Patients who refuse surgery have a 58% chance of poor recovery (House-Brackmann III of IV).
Patients who experience poor recovery often require facial enhancement or reanimation procedures. It is vitally important to continue to attend to the eye in these patients, and recommend surgical care to the eye, including tarsorrhaphy, spring, or gold weight, if corneal abrasions occur despite conservative medical care. Refer to Chapter 7.2 for more details. Botox has been used to help with bothersome blepharospasm due to synkinesis.
Outcome and Follow-Up
Patients are followed longitudinally to assess final recovery. Final recovery from a facial nerve injury may not be seen until 18 to 24 months after insult. According to Peiterson’s article charting the natural history of untreated Bell palsy, 71% of patients will recover completely, and an additional 13% will achieve near normal recovery (Hb I or II). Anyone with poor recovery or at risk for corneal abrasion should be considered for surgical reanimation or surgical management of the paralyzed eye. Patients with herpes zoster oticus are at a much higher risk (almost 50%) to experience poor recovery (Hb III or worse). Patients who recover, but then experience a recurrence of symptoms, should be evaluated for a neoplasm, Melkersson-Rosenthal syndrome, or inflammatory/autoimmune conditions.
ICD-9 Code
351.0 | Bell palsy |
Further Reading
Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical management of Bell’s palsy. Laryngoscope 1999;109(8):1177–1188
Peitersen E. The natural history of Bell’s palsy. Am J Otol 1982;4(2):107–111
2.1.4 Ear Foreign Bodies
Key Features
• Ear foreign bodies are commonly found in young children.
• The injury may be acute or chronic, with associated infection.
• Foreign bodies often consist of insects, small batteries, food, beads, pencil erasers, and other inert objects.
• Injury to the tympanic membrane, ossicles, facial nerve, or inner ear must be considered.
Foreign bodies in the external auditory canal are a common problem, especially in pediatric patients. The otolaryngologist often becomes involved after unsuccessful attempts at removal by the patient, parent, emergency room providers, and/or pediatricians. With children, one should have a low threshold for removal under anesthesia in the operating room.
Epidemiology
An ear foreign body is most commonly seen in children under 12 years of age.
Clinical
Signs and Symptoms
An acute foreign body may cause otalgia due to pressure on thin skin of the medial ear canal. Insects are extremely bothersome if alive. Obstruction may cause conductive hearing loss. Chronic foreign bodies, especially organic material such as food, may present with foul otorrhea or purulence. Pronounced hearing loss, vertigo, or facial weakness suggests injury to the middle ear (see Chapter 2.1.2).
Differential Diagnosis
The differential diagnosis includes a foreign body, otitis externa, otitis media, middle ear trauma, or a tumor.
Evaluation
History
In taking the patient’s history, you should inquire about the time course and possible nature of foreign body, if unclear. The previous level of hearing is important, as is a history of known tympanic membrane perforation. Injury involving an only-hearing ear mandates careful, experienced management.
Physical Exam
The examination should include a full head and neck exam. Rule out other foreign bodies. Document facial nerve function and perform a 512-Hz tuning fork exam, if patient is old enough and cooperative. The ear should be examined under the otomicroscope. Any purulence or drainage is suctioned with #3 or #5 Frazier tip suction to enable visualization of the foreign body, canal skin, and tympanic membrane, if possible.
Imaging
High-resolution CT scanning of the temporal bone is the most useful imaging study if there is concern for a middle or inner ear injury.
Other Tests
Perform an audiologic assessment if there is any concern of a middle ear injury.
Treatment Options
Most foreign bodies do not constitute an emergency and can be removed within a reasonable time period (i.e., days). Exceptions requiring prompt treatment include batteries (which cause tissue necrosis due to alkaline or acid leakage), insects, or objects associated with additional trauma to the middle ear or temporal bone. In the adult or cooperative child, one may be able to easily remove a foreign body in the office. If a child is at all uncooperative, it is preferable to proceed with removal under anesthesia in the operating room when convenient, in the next day or so. Live insects are first treated by instillation of 1% lidocaine to the canal, which promptly drowns/paralyzes the insect and anesthetizes the canal skin. The most useful instrument is a blunt otologic right angle hook, which may be positioned medial to the foreign body enabling removal. This is especially helpful for smooth objects, such as beads. An object that can be grasped and is intact may be amenable to the use of alligator forceps. Longstanding decaying organic material associated with infection requires suctioning. Gravel or sand against an intact tympanic membrane is best removed with irrigation. Following removal of a foreign body, careful inspection of the canal skin and tympanic membrane is important. Topical antibiotic and steroid drops for a few days are often helpful in treating or preventing local infection. Oral antibiotics are added for cellulitis, chondritis, and otitis media, as well as for the diabetic or immunosuppressed patient.
The presence of canal skin edema may require the placement of an Oto-Wick. Necrotic tissue secondary to acid or alkaline battery leakage, or thermal burns from slag foreign bodies due to welding are managed with serial débridement and antibiotic steroid drops; wicks or stenting are required for a circumferential canal injury. Management of injuries to the tympanic membrane and the middle ear, as well as temporal bone penetrating trauma are discussed in Chapter 2.1.2.
Outcome and Follow-Up
Uncomplicated removal of a foreign body usually does not require follow-up. If there is any associated infection, follow-up within a few weeks to document resolution following topical therapy is routine.
ICD-9 Code
931 | Ear foreign body |
Further Reading
McWhorter AJ, Limb CJ, Niparko JK. In Eisele DW, McQuone SJ, eds. Emergencies of the Head and Neck. St. Louis, MO: Mosby; 2000:367–369
2.2 Otitis Media
2.2.1 Acute Otitis Media
Key Features
• The presence of middle ear fluid along with a bulging or an inflamed tympanic membrane and pain are features of acute otitis media.
• It may also be accompanied by hearing loss, nausea, vomiting, or otorrhea.
• It is one of the most common childhood illnesses, contributing greatly to healthcare costs.
Acute otitis media (AOM) is very common in childhood, affecting at least 60% of children by age one, and 80% of children by age 3. It is clinically defined as a painful inflamed or bulging eardrum with middle ear purulence and fever, often accompanied by one or more additional systemic symptoms. In this setting, it is primarily viewed as a bacterial infection, and needs to be differentiated from viral OM as well as otitis media with effusion (OME) and chronic otitis media. The mainstay of management remains antibiotics, but some children with recurrent AOM will require surgical management with tympanostomy tubes. Occasionally, children will also require surgical management of a complication of AOM.
Epidemiology
AOM is common in children: 60% of all children under the age of 1 will suffer at least one bout, and that percentage increases to 80% by age 3. It can account for up to 20% of all clinic visits for pediatric patients 10 years old and younger. Specific risk factors other than age include male sex, attendance in daycare, exposure to cigarette smoke, and history of previous infection. There also appears to be a seasonal fluctuation, with more cases occurring in autumn or winter.
Clinical
Signs
Specific signs include an opaque, bulging, and erythematous tympanic membrane (TM) demonstrating poor mobility. If mastoiditis is suspected, the postauricular region may also be erythematous and edematous.
Symptoms
The Agency of Healthcare Research and Quality (Rockville, MD) defines acute otitis media as the presence of a middle ear effusion or the presence of fluid in the ear canal as a result of a ruptured TM with or without TM opacification, erythema, bulging, and hearing loss, and the rapid onset of one or more of the following: otalgia, otorrhea, irritability, and fever with or without anorexia, nausea, or vomiting.
Differential Diagnosis
The differential diagnosis of AOM is really a differential diagnosis for ear pain. Temporomandibular joint disease is probably the most common cause of ear pain that adult patients initially believe may be an ear infection. Another condition that can mimic AOM in adults is herpes zoster oticus. In that case the pain is from reactivation of the herpes virus, and vesicles will be seen in the canal and/or the periauricular region. The otolaryngologist should always consider the possibility of an occult malignant lesion of the upper aerodigestive tract, particularly the larynx, as a source of referred otalgia, especially in an adult patient with a normal ear exam and a history of tobacco abuse. Unilateral otitis media in the adult (more commonly chronic serous effusion) may arise secondary to a nasopharyngeal neoplasm causing obstruction of the eustachian tube orifice.
The most likely cause of ear pain in children is AOM, whether bacterial or viral. Other causes of ear pain are otitis externa, external canal trauma, and an external canal foreign body. Otitis externa can spread from the ear canal out to the auricle as a cellulitis. The auricle may then protrude from the skull with an increased auriculocephalic angle, and closely resemble AOM that has progressed to acute coalescent mastoiditis. AOM must also be distinguished from OME, which can be diagnosed as middle ear fluid with or without hearing loss, but without evidence of acute infection.
Evaluation
Physical Exam
The most important portion of the physical exam is inspecting the TM. The auricle and the external canal remain normal in appearance and are not tender to palpation. The appearance of the TM will change as the disease process follows its usual course. Initially, the TM is engorged and hyperemic. The hyperemia is most prominent along the manubrium of the malleus and the periphery of the drum. The TM is sluggish to pneumatic otoscopy, but all normal topographic landmarks are visible. As the infection progresses and the middle ear fills with pus, the TM thickens, bulges, and loses normal landmarks. There may be erythema, tenderness, and edema in the postauricular region, especially in small children.
If the infection progresses untreated, the TM perforates in the pars tensa, and the patient experiences a resolution of pain and fever. If purulence is seen in the external canal, then cultures should be obtained. If the perforation heals, and pus reaccumulates untreated, the infection may spread through the antrum into the mastoid, and the mastoid trabeculae may begin to decalcify, leading to coalescent mastoiditis along with other complications. At this stage, the auricle becomes more prominent from the skull as postauricular edema increases. It is important to differentiate this from a severe otitis externa with painful cellulitis and swelling of the auricle.
Imaging
Imaging is usually not indicated unless coalescent mastoiditis or another complication of otitis media is suspected. If such a complication is suspected, a fine-cut temporal bone CT with contrast is indicated. If the patient is an adult with a persistent unilateral otitis media, and the nasopharyngeal exam is equivocal, then an MRI of the head with attention to the nasopharynx may be considered to evaluate for a mass lesion obstructing the eustachian tube.
Labs
Labs are rarely needed to treat routine AOM. One would expect to see leukocytosis on CBC. Routine cultures can be obtained if the ear is draining, and is absolutely indicated in an infant less than 6 weeks of age. Tympanocentesis is rarely indicated to obtain cultures, unless suspicion is high for a resistant pathogen and empiric therapy might not be indicated. Tympanocentesis may be helpful in the immunocompromised patient, especially the patient with chemotherapy neutropenia or acquired immunodeficiency syndrome (AIDS).
Other Tests
An audiogram is not needed in the acute phase, but can be helpful in evaluating children with recurrent AOM, especially in light of other cognitive delays. In cases where the presence of an effusion is in question, tympano-grams may be helpful. Occasionally, the combination of a good pneumatic exam and an accurate tympanogram are needed to determine the presence of an effusion, even for an experienced otologist.
Pathology
Most commonly, the bacteria that cause AOM will gain entry to the middle ear cleft by way of the eustachian tube. The eustachian tubes of infants are short and horizontally aligned. Infants are also likely to eat in a reclined position. These factors put them at high risk for penetration of nasopharyngeal secretions into the middle ears via the eustachian tubes.
Once they grow into early childhood, they continue to suffer from multiple upper respiratory infections each year, and each bout of nasopharyngeal mucosal congestion can close a eustachian tube, leading to negative pressure behind the eardrum, exudate formation, and infection once the exudate becomes contaminated. An allergy can also lead to AOM secondary to eustachian tube dysfunction.
AOM in adults, especially if unilateral, may be ominous. The nasopharynx must be fully evaluated to identify the cause of the eustachian tube blockage or dysfunction. A nasopharyngeal mass must be ruled out prior to ascribing the cause to either an upper respiratory infection or a recent airline flight. An allergy may also contribute to AOM in adults.
Historically, the most common bacterial pathogens causing AOM have been Staphylococcus pneumoniae (40–50%), nontypeable Haemophilus influenzae (20–30%), and Moraxella catarrhalis (10–15%). Over time, strains of Pneumococcus have become penicillin-resistant due to an alteration of the penicillin binding site, and strains of H. influenzae have become-lactamase positive. Also, recently, children vaccinated with a 7-valent pneumococcal vaccine may have a decreased rate of S. pneumoniae and a subsequent increase in H. influenzae.
Histologically, middle ears display signs of inflammation and edema. The TM and middle ear mucosa are thickened and engorged with an inflammatory infiltrate. There is often frank pus in the middle ear space.
Treatment Options
Medical
There has been a trend toward treating children with uncomplicated AOM symptomatically with pain control and no antibiotics for the first 24 to 48 hours, but this should only be done in children where close follow-up can be performed. Otherwise, uncomplicated AOM is a medical disease, and if persisting more than 24 to 48 hours requires antibiotic therapy. Traditional empiric therapy has been appropriately dosed amoxicillin as a first-line antibiotic because it is effective, well tolerated, and inexpensive. With emerging resistance, the dose of amoxicillin has been doubled to 80 to 90 mg/kg/day. If patients fail to improve at 48 to 72 hours, they can be switched to high-dose amoxicillin-clavulanate. If patients are penicillin allergic, second- or third-generation cephalosporins, macrolides, or clindamycin are all options.
Surgical
AOM is not a surgical disease. In patients failing to respond to empiric therapy, diagnostic tympanocentesis may be done for culture. Removing the fluid from the middle ear may also relieve pain.
Patients evaluated for recurrent AOM may be candidates for tympanostomy tubes. Standard criteria for tube placement include more than three episodes of AOM in the preceding 6 months or more than four episodes of AOM in the preceding 12 months.
Complications
See Chapter 2.2.3 for complications of AOM. Complications of tube placement include otorrhea, retained tubes, and postextrusion perforations. Otorrhea may occur in upwards of 10%, and is treated with appropriate ototopical drops, currently fluoroquinolones as they are not ototoxic. Tubes are watched yearly, and if they have not extruded after 3 years, many otolaryngologists plan removal under general anesthesia. Postoperative perforations are estimated to occur 3 to 5% of the time, and are followed conservatively. If they persist or cause considerable hearing loss, tympanoplasty may be recommended.
Outcome and Follow-Up
Children with tympanostomy tubes require little postoperative care, and physician preference is usually the driving force determining postoperative recommendations. Many otolaryngologists advocate the use of 5 days of antibiotic topical drops twice daily [i.e., Ciprodex (Alcon Laboratories, Fort Worth, TX) or Floxin Otic (Daiichi Pharmaceutical Corporation, Montvale, NJ)] postoperatively only to children with mucoid or purulent effusions found at the time of tube placement. Many otolaryngologists also recommend ear plugs only for children swimming in fresh water, and not during bath or shower time.
The children are otherwise followed with a postoperative audiogram and interval visits at 6 to 12 months until the tubes extrude.
ICD-9 Code
382.9 | Acute otitis media |
Further Reading
American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics 2004;113(5):1451–1465
Brunton S, Pichichero ME. Acute otitis media: influence of the PCV-7 vaccine on changes in the disease and its management. J Fam Pract 2005;54(11):961–968
Rothman R, Owens T, Simel DL. Does this child have acute otitis media? JAMA 2003;290(12):1633–1640
Sautter N, Hirose K. Otitis media. In: Hughes GB, Pensak ML, eds. Clinical Otology. 3rd ed. Stuttgart/New York: Thieme; 2007:223–235
2.2.2 Chronic Otitis Media
Key Features
• Chronic or chronically recurring middle ear drainage through a perforated tympanic membrane (TM) is seen.
• Chronic otitis media is associated with a conductive or mixed hearing loss.
• It may occur with or without cholesteatoma.
Chronic otitis media (COM), also referred to as chronic suppurative otitis media with or without cholesteatoma, is characterized by continuous or intermittent otorrhea via a longstanding TM perforation. (This condition is to be distinguished from persistent serous effusion of the middle ear, sometimes referred to as chronic otitis media with effusion but better termed “chronic serous otitis.”) If the drainage has stopped, but the perforation persists, the condition is considered inactive. An associated conductive hearing loss may be present, and polyps on the TM or in the middle ear raise the suspicion of concomitant cholesteatoma. Management is initially medical, but can become surgical for recalcitrant cases or those with significant hearing loss or cholesteatoma.
Epidemiology
The epidemiology of COM is not well defined. This is due to its being part of the spectrum of otitis media. It shows no gender preference, but does show a preference for certain populations – Native Americans, American Eskimos, and Australian Aborigines.
Clinical
Signs
Signs include a perforated eardrum with or without polypoid granulation within the middle ear or external auditory canal. Polypoid changes, retraction pockets, or desquamating debris may indicate cholesteatoma. Fevers, neck stiffness, and any change in mental status may be signs of an intracranial complication.
Symptoms
Symptoms usually consist of chronic or intermittent painless otorrhea. Pain may indicate a coincidental otitis externa, or an impending intratemporal or intracranial complication. Hearing loss is often present. An erosive cholesteatoma may breach the otic capsule resulting in SNHL, tinnitus, vertigo, and imbalance. Facial paresis or paralysis is rarely seen, but may be present with or without cholesteatoma.
Differential Diagnosis
Other than COM, painless otorrhea with a TM perforation may result from carcinoma of the TM or middle ear and can arise from ears with a history of COM. Any polypoid material removed needs to be sent for pathologic evaluation. Wegener granulomatosis may present in an adult as COM with fluctuating hearing loss and cranial nerve palsy without a previous history of OM. Tuberculous OM should be considered in a draining ear that does not improve despite maximal medical and surgical treatment. The classic description of tuberculous OM is painless otorrhea with multiple TM perforations.
Evaluation
Physical Exam
The physical exam focuses on the draining ear, and specifically on adequate visualization of the eardrum. Often inflammation, especially of the skin of the ear canal, must be controlled first. This may require treatment with topical or oral antibiotics. Once the canal edema has resolved, the TM is meticulously cleaned under an operating microscope. All debris and granulation tissue are cleaned, especially those covering the posterosuperior quadrant of the TM, and any tissue samples are sent to the pathology laboratory. Frequent cleaning and home ototopical medication with an acidic irrigation (acetic acid) may be needed prior to successfully drying the ear.
Imaging
Obtaining CT scans prior to surgical management is controversial, and dependent upon surgeon preference and training. Some surgeons will not scan any patients, some will scan only those with cholesteatoma, and some obtain CT scans for all patients being evaluated with COM. Most surgeons would agree that anyone suffering from a suspected intratemporal or intracranial complication of COM should be imaged with a high-resolution CT scan of the temporal bones with and without contrast. Also, anyone undergoing revision surgery should be imaged. CT scans yield information regarding disease and local anatomy that improves the informed consent process, and makes patients and especially parents more comfortable regarding the decision to undergo surgery.
Labs
Drainage, especially if recalcitrant to empiric therapy, should be cultured. Aerobic and fungal cultures are routinely sent. Additional blood work is rarely indicated. If the onset of symptoms is bilateral, recent, and accompanied by fluctuating hearing loss, or cranial nerve palsy, then c-ANCA is sent to rule out Wegener granulomatosis.
Other Tests
An audiogram is obtained once the ear is dry and prior to any surgical intervention. A conductive hearing loss is expected, and a mixed loss is not uncommon. Some authors feel that COM can lead to SNHL over time. Any granulation retrieved from the ear is sent to pathology to rule out carcinoma.
Pathology
The most common pathogens leading to COM are Pseudomonas aeruginosa and Staphylococcus aureus. They gain access to the middle ear through the perforated TM. They then spread from the middle ear to mastoid. These same pathogens can also colonize the avascular debris collecting within a cholesteatoma. A recent problem is the emergence of methicillin-resistant S. aureus (MRSA) COM.
The middle ear mucosa becomes thick, fibrotic, and infiltrated with inflammatory cells. Mucosal edema leads to polyp formation and granulation. Bony vascular channels embolize secondary to chronic inflammation, leading to bone erosion, particularly involving the ossicular chain. Cholesteatoma may erode bone by additional local inflammatory response and osteolytic enzymes.
Treatment Options
The goals of treatment are elimination of infection and restoration of function.
Medical
In many cases, medical therapy is employed to dry disease preoperatively, permit better office assessment, or manage the patient with comorbidities in whom surgery is contraindicated. COM may be initially treated with empiric ototopical antibiotic drops. Awareness of ototoxicity has made fluoroquinolone drops the preferred method of treatment. Ototopical drops reach the middle ear in such high concentrations, that resistance is rarely an issue. See Table 2.4 for topical treatment options. If the drainage does not respond, then cultures are indicated to rule out a rare resistant strain such as MRSA or a fungal infection. Vinegar washes or 2% acetic acid drops may be effective. There are several topical powders that also may periodically be applied if drops do not work. One such mixture includes ciprofloxacin, boric acid, dexamethasone, and fluconazole. Appropriate long-term IV antibiotics may also be indicated if an osteitis is suspected. Another effective topical powder preparation to help dry the chronically draining ear that is unresponsive to drops is chloramphenicol 50 mg, p-aminobenzenesulfonamide 50 mg and amphotericin 5 mg, with or without hydrocortisone 1 mg; this is mixed and delivered 1 or 2 puffs via a powder insufflator (e.g., OTOMED, Lake Havasu City, AZ) twice daily. Another option for office management is aqueous gentian violet, which has antifungal properties, and may be “painted” over inflamed areas under the otomicroscope.
Topical Agent | Typical Dose Regimen |
|---|---|
2% acetic acid | 5 drops 2–3 times daily |
2% acetic acid/1% hydrocortisone solution | 5 drops 2–3 times daily |
Floxin otic | 10 drops twice daily |
Ciprodex or Cipro HC otic | 5 drops twice daily |
Cortisporin otic suspension | 5 drops 3 times daily |
CSF powder (chloramphenicol 50 mg, p-aminobenzenesulfonamide 50 mg and amphotericin 5 mg, with or without hydrocortisone 1 mg) | 2 puffs twice daily |
Gentian violet (aqueous) | Physician applies topically under microscope in office as needed |
Surgical
There are multiple reasons to operate for COM. The infection and drainage can be eradicated, the TM can be repaired, the hearing can be improved, and in the case of cholesteatoma, the disease can be removed and the ear made safe. It is better to dry the ear prior to surgical intervention, but sometimes it is not possible. In cases of drainage at the time of surgery continue with culture-directed antibiotics in the preoperative and postoperative period.
Surgical algorithms vary by preference, training, and experience. The following is a general list of options (nonexhaustive) with definitions.
1. Tympanoplasty without mastoidectomy: eradicating disease limited to the middle ear, whether TM grafting is or is not required. Otorrhea can be controlled, the TM repaired, middle ear cholesteatoma removed, and hearing improved or stabilized. TM grafting material includes loose areolar tissue, temporalis fascia, perichondrium, vein, or cartilage. The graft can be placed either medial or lateral to the TM.
2. Atticotomy: during tympanoplasty, but without performing a mastoidectomy, removing the posterior bony annulus and scutum can improve visualization into the posterior mesotympanum, hypotympanum, and attic. The entire ossicular chain can be visualized and cleaned, as can the tympanic portion of the facial nerve. This can facilitate removal of granulation, retractions, and small cholesteatomas, especially for disease lateral to the ossicles. This is ideal for pars flaccida cholesteatoma that is lateral to the ossicular chain. Cartilage is used to reconstruct the missing bone to prevent repeat retractions, and a mastoidectomy can be avoided in certain cases.
3. Tympanomastoidectomy with an intact canal wall: opening the mastoid in conjunction with debriding and reconstructing the middle ear can improve outcomes in selective patients. Patients with previously failed tympanoplasty or longstanding otorrhea can be harboring mastoid granulations and infection. Cholesteatoma extending into the antrum will require this approach.
Microsurgical techniques are required to exenterate all involved air cell tracts. With appropriate thinning of the posterior ear canal and the tegmen, the epitympanum can often be completely exposed. When patient anatomy makes this impossible, partial transcanal atticotomy can be performed concurrently. The facial recess may be opened to improve middle ear access and aeration. Removal of the malleus head is often required for disease extending medial to it or into the supratubal recess. A second-look operation is often planned in cases of cholesteatoma, to assess for recurrent disease and/or perform ossicular reconstruction.
4. Tympanomastoidectomy with canal wall down: this technique is employed in managing COM with extensive cholesteatoma, and rarely in uncomplicated COM without cholesteatoma. This technique is indicated in otherwise unresectable disease, noncompliant patients, only-hearing or already anacusic ears, and patients with small or contracted/sclerotic mastoids prior to surgery. Removing the posterior canal wall increases visualization of the anterior epitympanum, the posterior mesotympanum, and provides access to remove disease more effectively from the sinus tympani. Mastoid cavities may fail, harbor cholesteatoma, or chronically drain if a high facial ridge is left, a dependent mastoid tip results, the TM graft fails, or the meatoplasty is inadequate. Surgeons must carefully attend to these fine details to ensure success.
Complications
Complications of COM are divided into intratemporal and intracranial, and are covered in Chapter 2.2.3. Complications from surgery for COM are covered here. Postoperative complications are rare if surgery is performed meticulously. The best care for otologic postoperative complications is prevention. Postoperative pain is usually mild, and all patients calling with severe pain need to be evaluated. Wound infections are treated with culture-directed antibiotics. Pseudomonas is the most likely offending organism, and fluoroquinolones are likely to be the most effective agent used. Postoperative hematomas at the site of graft harvesting are rare, but need to be drained when encountered.
Facial nerve injuries are rare. The use of facial nerve monitoring during even routine ear surgery is becoming widely accepted. Intraoperative injury needs to be addressed immediately, with appropriate nerve exploration, decompression, and grafting if indicated. Getting the advice of a partner or a more experienced otologic surgeon can be helpful in these cases. Facial function that is normal initially, and then worsens over time is usually the result of edema, and is managed expectantly with antibiotics and oral steroids. When a patient awakens from a mastoid procedure with an unexpected facial weakness, it is prudent to observe the patient for a few hours to allow for the reversal of the affects of any local anesthetic used during the procedure prior to reexploration.
Mild vertigo is common following any middle ear procedure, but intra-operative labyrinthine injury results in severe postoperative vertigo (and possible anacusis). Addressing the defect immediately with bone wax or fascia is helpful, but patients will likely still suffer severe vertigo requiring a few days of hospitalization. In this setting, postoperative oral or parenteral vestibular suppressants are administered, and vestibular exercises will hasten recovery.
Granulations and synechiae in the ear canal or canal wall down cavity are removed when encountered, and occasionally meatoplasties require revision.
Outcome and Follow-Up
Perioperative antibiotic use varies widely among surgeons. Many surgeons advocate the use of preoperative and postoperative systemic antibiotics only if the ear cannot be dried prior to the surgery. Surgery is primarily outpatient, with patients returning for an office visit at either 1 or 2 weeks. At that visit most of the reachable packing is removed, and the patient is placed on ototopical drops nightly. Canal wall down cavities are filled with an antibiotic/steroid ointment, and the patient is started on ototopical drops twice a day. Patients are then seen at 4 to 6 week intervals to inspect the graft and clean any granulations. Water is kept out of the ears until complete epithelialization occurs. Routine audiometry is generally performed at 8 to 12 weeks.
The literature cites success rates of surgical management for COM anywhere from 78% to over 90%. Surgical technique and disease severity both factor into outcomes. Cholesteatoma recurrence rates cited in the literature also range anywhere from 3 to 50%. With these percentages in mind, patients are usually followed for several years.
ICD-9 Codes
381.3, 381.4, 382.1, 382.2, 382.3 Chronic otitis media | |
385.30 Cholesteatoma |
Further Reading
Cruz OLM, Kasse CA, Leonhart FD. Efficacy of surgical treatment of chronic otitis media. Otolaryngol Head Neck Surg 2003;128(2):263–266
Haynes DS, Harley DH. Surgical management of chronic otitis media: beyond tympanotomy tubes. Otolaryngol Clin North Am 2002;35(4):827–839
Slattery WH. Pathology and clinical course of inflammatory diseases of the middle ear. In: Glasscock ME, Gulya AJ, eds. Surgery of the Ear. Toronto, ON: BC Decker; 2003:422–433
Weber PC. Chronic otitis media. In: Hughes GB, Pensak ML. Clinical Otology. 3rd ed. Stuttgart/New York: Thieme; 2007:236–249
2.2.3 Complications of Acute and Chronic Otitis Media
Key Features
• Antibiotics have produced an overall decline in the frequency of complications of otitis media.
• Complications of acute and chronic otitis media may be both intracranial and extracranial.
• The most common extracranial complication is postauricular abscess; the most common intracranial complication is meningitis.
Acute otitis media is one of the most common diagnoses in patients presenting to physicians. Approximately 85% of all children will have at least one episode. A fraction of patients go on to suffer complications due to progression of infectious and inflammatory processes. More than 60% of patients who suffer complications do so within the first two decades of life. Complications are subdivided by site (extratemporal, intratemporal, and intracranial).
Extratemporal Complications
Subperiosteal Abscess
Mastoiditis either directly erodes the bone of the lateral wall of the mastoid or traverses mastoid emissary veins into the subperiosteal space adjacent to the mastoid.
Signs and Symptoms
Fever, malaise, and pain are associated with a subperiosteal abscess.
Physical Exam
On the physical exam the patient may present with otalgia, otorrhea, an anteriorly and laterally displaced auricle, and fluctuant, erythematous, postauricular fluid collection.
Imaging
CT is the preferred imaging mode.
Treatment Options
The recommended treatment typically includes myringotomy with or without tube, incision and drainage of the abscess, and IV antibiotics. Cortical mastoidectomy is frequently recommended, particularly in the presence of cholesteatoma.
Bezold Abscess
Mastoiditis leads to erosion of the mastoid tip bone deep to the digastric ridge. Purulent material is directed into the neck, deep to the sternocleidomastoid muscle (SCM).
Signs and Symptoms
Fever, malaise, and neck pain are associated with a Bezold abscess.
Physical Exam
The patient may present with otalgia, otorrhea, and a tender upper cervical mass.
Imaging
Contrast-enhanced CT will confirm the presence of a rim-enhancing cervical abscess in combination with mastoiditis.
Treatment Options
Recommended treatment includes IV antibiotics, myringotomy with or without tube, cortical mastoidectomy, and incision and drainage of the neck abscess.
Intratemporal Complications
Labyrinthine Fistula
A labyrinthine fistula is caused by an erosion of otic capsule bone and exposure of the membranous labyrinth. The incidence is 7% of patients with cholesteatoma. 90% of fistulas occur in the horizontal semicircular canal.
Signs and Symptoms
A significant number of patients will be asymptomatic, and fistulas will only be discovered within the course of mastoidectomy. 62% of patients complain of periodic vertigo or imbalance. Patients may experience the Tullio phenomenon (vertigo induced by loud sounds). SNHL may also be present, but is neither sensitive nor specific.
Physical Exam
Fistula testing (nystagmus with pneumatoscopy) is positive in ~50% of patients.
Imaging
Thin-cut temporal bone CT is preferred; however, small fistulas may still be missed.
Treatment Options
Treatment is controversial, as violation of the labyrinth may result in a dead ear. Many authors recommend canal wall down mastoidectomy, leaving cholesteatoma matrix overlying the fistula to form the lining of the exteriorized mastoid cavity. In cases of small fistulas that have not violated the membranous labyrinth, some authors advocate complete matrix removal and semicircular canal resurfacing with bone pate, fascia, or a similar sealant. Others recommend leaving the matrix in place, leaving the canal wall up, and coming back to remove the matrix and resurface the labyrinth at a second stage.
Coalescent Mastoiditis
Suppurative progression of untreated or incompletely treated acute OM results in erosion of the mastoid cavity trabecular bone. Time course of progression is typically 2 to 4 weeks.
Signs and Symptoms
Symptoms include fever, malaise, and otalgia.
Physical Exam
On the physical examination, purulent otorrhea or a bulging TM, postauricular erythema, tenderness, and edema displacing the auricle anteriorly and inferiorly are found.
Imaging
A CT scan confirms mastoid and middle ear opacification with erosion of trabecular mastoid cavity bone. Frequently, erosion occurs primarily adjacent to the sigmoid sinus.
Treatment Options
Recommended treatment includes myringotomy with or without tube, IV antibiotics, and cortical mastoidectomy. Others advocate myringotomy alone and IV antibiotics for 3 to 6 weeks with serial CT confirmation of resolution of mastoid and middle ear opacification.
Petrous Apicitis
Petrous apicitis is a rare complication resulting from the spread of infection into air cells within a pneumatized petrous apex (the prevalence of pneumatization is 30%).
Signs and Symptoms
The classic triad of deep retroorbital pain, purulent otorrhea, and ipsilateral abducens palsy (Gradenigo syndrome) is seen. CN VII and VIII dysfunction also may occur.
Imaging
A CT scan will show opacification of a pneumatized petrous apex.
Other Tests
MRI and lumbar puncture (LP) are helpful to assess concurrent intracranial processes.
Treatment Options
First-line therapy is long-term IV antibiotics secondary to the difficulty of surgical access to the petrous apex. Abscess, necrotic bone, or failed medical therapy requires surgical drainage. Hearing status determines the choice of approach. Hearing preservation may be attempted by infracochlear, infralabyrinthine, retrolabyrinthine, subarcuate, and middle fossa approaches. Translabyrinthine or transcochlear approaches may be used for nonhearing ears.
Facial Paralysis
Facial paralysis results from inflammation of dehiscent segments of the facial nerve secondary to infection.
Imaging
CT scanning for AOM-associated incomplete paralysis may not be necessary, but may help in operative planning in the setting of cholesteatoma or complete paralysis.
Pathology
In the setting of children with AOM, a congenitally dehiscent tympanic segment of the facial nerve is suspected. The paralysis is usually incomplete and resolves within 3 weeks. In the face of COM and cholesteatoma, dehiscence is typically due to fallopian canal erosion secondary to disease. Onset may be slow and progressive. The prognosis is poorer and recovery slower.
Treatment Options
Paralysis due to AOM is treated with IV antibiotics and myringotomy. Cholesteatoma-associated paralysis requires mastoidectomy, nerve decompression proximal and distal to the diseased segment, and débridement of inflammatory tissue.
Acute Suppurative Labyrinthitis
Acute suppurative labyrinthitis results from direct bacterial invasion of the labyrinth, resulting in total auditory and vestibular loss. Acute suppurative labyrinthitis may lead to meningitis and vice versa.
Signs and Symptoms
Acute-onset total sensorineural deafness and severe vertigo are signs of acute suppurative labyrinthitis.
Pathology
Predisposing factors include congenital inner ear malformations and otic capsule erosion secondary to cholesteatoma.
Treatment Options
Labyrinthine functional loss is unavoidable, but patients should be treated with antibiotics to prevent the progression to meningitis. Vertigo is treated symptomatically and typically improves as patients compensate.
Intracranial Complications
Meningitis
Meningitis is the most common intracranial complication of OM.
Signs and Symptoms
Fever, headache, nausea, vomiting, photophobia, and nuchal rigidity are symptoms of meningitis. Seizures, ataxia, and other focal neurologic signs are ominous findings.
Imaging
CT or MRI is essential to rule out other intracranial processes and establish the safety of LP.
Other Testing
LP is diagnostic (suggestive CSF findings: increased pressure, increased protein, decreased glucose, inflammatory cells or bacteria present).
Pathology
The potential routes of bacterial spread from the ear to the CSF include hematogenous seeding, bony erosion with direct spread, and bony channels (suppurative labyrinthitis, Hyrtl’s fissures, congenital defects, and traumatic defects).
Treatment Options
Because meningitis is the most common complication seen with OM, detailed antibiotic guidelines are listed in Table 2.5. First-line therapy is IV antibiotics, myringotomy, and steroids (decreases hearing and neurologic sequelae). In the presence of cholesteatoma, coalescent mastoiditis, or failure of medical therapy, mastoidectomy is indicated.
Brain Abscess
The most frequently lethal intracranial complication of OM is a brain abscess.
Signs and Symptoms
The clinical course is multistage, starting with fever, malaise, nausea, vomiting, headache, mental status changes, and seizures. This may be followed by a quiescent phase with moderate clinical improvement. The third stage, thought to represent abscess growth and ultimate rupture, is a rapid and fulminant return of symptoms with sudden clinical decline.
Neonate (<1 month) • Ampicillin +gentamicin; or ampicillin third + generation cephalosporin |
Newborn (1–3 months) • First choice: Ampicillin +(cefotaxime or ceftriaxone) + dexamethasone (0.15 mg/kg every 6 h × 4 d) • Alternative: Chloramphenicol + gentamicin |
Infant or Child (>3 months) • First choice: (Cefotaxime or ceftriaxone) + dexamethasone • Alternative: Ampicillin |
Older Child or Adult • (Cefotaxime 2 g IV every 6 h or ceftriaxone 2 g IV every 12 h) + ampicillin 2 g IV every 4 h + dexamethasone 0.4 mg/kg every 12 h × 2 d vancomycin (child 15 to 22.5 mg/kg IV every 6 h; adult 1 g IV every 12 h) • If Pseudomonas suspected: Cefepime 2 g IV every 8 h instead of cefotaxime or ceftriaxone • For a penicillin-allergic patient in whom cephalosporin cannot be used: Vancomycin 15–22.5 mg/kg IV every 12 h + trimethoprim/sulfamethoxazole 15 to 20 mg/kg/day IV divided every 6 h or • Vancomycin 15 to 22.5 mg/kg IV every 12 h + chloramphenicol 1 g IV every 6 h ± rifampin 600 mg once daily |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


