CHAPTER 2
Basic. “Need-to-Know” Immunology
As with all new additions to a practice, some basic principles underlying the diagnosis and treatment of allergy must be digested and understood if the care provided is to prove effective. A “cookbook” or “owner s manual” approach may produce some early successes, but as soon as the first case arrives that presents some atypical patterns, this type of approach may be expected to fail. Such failure may discourage the patient, and repeated failures may easily discourage the physician and undermine the credibility of the practice.
It is not necessary to understand fully all the underlying mechanisms by which allergy affects the body (this is fortunate, as science does not as yet fully understand all these mechanisms). Nor is it necessary to keep at one’s fingertips all the principles of each test devised for the diagnosis of allergy. What is necessary is a basic, general knowledge of the immunologic mechanisms governing allergy as far as they are understood at present, and of how these mechanisms apply to allergy testing and treatment. Details, as presented here, should be reviewed and understood, but they may then be relegated to the realm of “know where to find when needed.”
“NEED-TO-KNOW” IMMUNOLOGY: BASIC IMMUNOLOGICAL PRINCIPLES
There are numerous immunology texts, and most are written at a relatively detailed level, but practicing physicians have a relatively limited interest in learning immunology simply for the sake of immunology. Further, the study of the immune system is extremely complex and continues to evolve, incorporating bits of knowledge being added by way of ongoing research. The immune system appears to have a major place in the body’s function, but many of its specific aspects remain theoretical and at times incomprehensible. As a result of these factors, many practitioners would prefer simply to pay respect to the immune system and then move on to something more understandable and of clinical use.
Unfortunately, allergy cannot be understood or practiced without a basic understanding of immune system function. Simply put, allergy develops as an alteration of the immune system in response to environmental exposures within a genetically susceptible individual. Experience has demonstrated that the immune system can be manipulated to achieve long-lasting benefits in allergy care. Like all aspects of medicine, practices keep changing as new knowledge appears, and an understanding of immunologic principles involving allergy is necessary to evaluate new procedures properly and integrate them into the practice as needed. Every attempt is made here to limit the immunology discussion to what is needed to understand basic aspects of allergy and, to some degree, communicate them to the inquiring patient. The first portion of the following discussion addresses an overall view of the immune system in the normal individual. It is needed as background. The reader should note the “need-to-know” caveat at the end of the following section before becoming discouraged.
Function of the Immune System
The ecosystem exists in a delicate state of equilibrium, within which life must be balanced with death. All organisms exist within this system as both predators (or scavengers), at some level, as well as prey (sources of nutrition). Microorganisms serve an important role within the ecosystem by attacking and breaking down devitalized organic matter so that it may be reintroduced into the environment as a nutrient source. Unfortunately, microorganisms lack the capability for concern for the well-being of the potential host, thus necessitating the need for protection of the potential host. During the life of an organism the immune system provides the means by which it may exist within such a hostile environment. As such, part of the role of the immune system is to provide environmental surveillance, sorting various items encountered within the ecosystem into those that are threatening (e.g., bacteria) and those that are beneficial (e.g., nutrients). One element that is important to this process is the ability of the immune system to differentiate foreign bodies (such as viruses, fungi, bacteria, etc.) from the body’s own cells. Immunologically speaking, the immune system differentiates between “self” and “nonself,” but its function goes beyond that, because it must be able to distinguish between beneficial “nonself” (nutrients) and harmful “nonself” (bacteria and viruses, for example.) Much of the information necessary for this process of recognition is encoded on unique receptors located on the surface of each of the host’s native cells. If a cell is encoded with the appropriate receptors, then the immune system recognizes the cell as “self” and allows it to continue to function. If, on the other hand, the cell does not possess those receptors or is encoded in such a way that the immune system recognizes the cell as “nonself,” a complex series of events intended to neutralize the “invader” will be set into action. Additionally, this process extends to identification of the body’s own cells that have become dysfunctional due to processes such as aging or malignancy.
The immune system consists of several cellular and noncellular components that are present within the central circulatory system, peripheral tissues, and mucosal surfaces of the body. Each of these components acts either independently or in conjunction with other constituents of the immune system to identify, process, or neutralize substances foreign to the body. This large variety of components of the immune system provides flexibility and allows for it to adapt and respond to foreign substances in several ways. Further, it provides for a redundancy of protective systems.
In a broad sense, the immune system can be separated into two categories based on the specificity of the response to an individual foreign body. Innate immunity consists of a generalized, nonspecific response to a foreign substance. This type of response makes use of components of the immune system such as epithelial barriers, macrophage phagocytosis, and activation of the complement cascade. Key to these processes is that they do not depend on specific recognition of the foreign substance by the body, only that it is foreign to the body. In other words, the host can be naive to the invader.
In contrast to innate immunity, adaptive immunity describes the hosts ability to mount a specific response targeting a foreign body that is recognized by the immune system. This process requires prior exposure to the foreign body, which leads to antigen processing, sensitization, formation of antibodies, and specific activation of T and B lymphocytes. This type of response is based on recognition of a specific antigen by an antibody or lymphocyte. The allergic response is a classic example of adaptive immunity.
Components of the Immune System
ANTIGEN
The adaptive response is triggered by an antigen, which by definition is the key element within a foreign body capable of eliciting an immune response when recognized by a sensitized antibody or lymphocyte. Antigens typically consist of short protein or polysaccharide sequences that are contained within a foreign body. Because antigens consist of only portions of the foreign body, they frequently must be processed to an optimal size and configuration that will facilitate interaction with the immune system. Typically, this processing occurs when a substance first enters the body. At that point it is identified as foreign to the body and phagocytosed by a macrophage or other antigen-presenting cell. Within the macrophage the foreign body is processed and that portion capable of triggering an immune response (antigen) is cleaved and “displayed” on the external surface of the cell’s membrane. While in this position, the antigen is presented to a T lymphocyte by direct cell-to-cell contact and the process of “programming” cellular (B and T lymphocytes) and noncellular (antibodies) components of the immune system to recognize the particular antigen is initiated. This series of steps is referred to as sensitization.
LYMPHOCYTES
Lymphocytes represent the key cells that form the basis of the adaptive immune response, and are responsible for such things as immunologic memory, rapid expansion of the immune response, triggering of other cellular and noncellular components of the immune response, and production of antibodies. Lymphocytes are all produced in the bone marrow, but after release into the circulation they differentiate into two distinct populations. One of these populations of lymphocytes further differentiates into T lymphocytes after undergoing further processing within the thymus gland (thymus-dependent). The mature T lymphocyte is defined by the presence of T-cell receptors (TCR) on its surface, which serve as sites for direct cell-to-cell communication with a variety of other immune cells. T lymphocytes are also capable of secreting chemical messengers, referred to as cytokines, which serve to direct behavior of other cellular components of the immune system. T lymphocytes further differentiate into T-helper or T-suppressor cells, each capable of up-regulating or down-regulating inflammatory responses, respectively. Each of these populations of differentiated T lymphocytes offset the actions of the other, thus providing control of the inflammatory process. The T lymphocyte also plays an active role in cell-mediated immunity (type IV hypersensitivity), presented later in this chapter. These characteristics of the T lymphocyte provide for its important function as a director of the immune response.
B lymphocytes constitute the other large population of lymphocytes crucial to immune function. The primary role of the B lymphocyte is ultimately to produce antibodies (immunoglobulins). As with T lymphocytes, these cells are derived from a pool of naive lymphocytes that are formed within the bone marrow. But unlike the T cell that matures in the thymus, the continued maturation of the B cell takes place within the bone marrow (hence B for bone marrow-dependent lymphocytes). During this process, the cell membrane of the B lymphocyte acquires and expresses a multitude of nonspecific antibodies [immunoglobulins M and D (IgM, IgD)]. This process is antigen independent and yields a B cell that is prepared for further antigen-specific differentiation after it exits the bone marrow.
When in the periphery, the B cell undergoes a process by which it acquires the capability to produce an antigen-specific antibody. This multistep process is referred to as isotype switching and is under the direct control of the T-helper cell (CD4). In a simplified sense, the host comes into contact with a foreign body. In the case of allergy, this contact usually takes place at a mucosal surface [respiratory mucosa, conjunctiva, gastrointestinal (GI) tract, etc.], as this is the point of initial entry of most substances or organisms foreign to the host. The foreign body is then phagocytosed and processed, as described previously, by an antigen-presenting cell (macrophage, Langerhans cell, etc.). The antigen that represents and is specific to that invader is then positioned on the surface of the antigen-presenting cell and presented to a TCR site of a T-helper lymphocyte (CD4). Although this process is regulated by chemical mediators that are secreted by the T lymphocyte (cytokines), the information that is specific to the antigen can be transferred only by this process of cell-to-cell contact.
After the T lymphocyte gains this antigen-specific information, it presents this information by way of cell-to-cell contact to a naive B lymphocyte. This enables the B lymphocyte to differentiate into one capable of producing antibodies unique to the antigen. After the process of isotype switching has occurred, that B-lymphocyte lineage is committed to production of a single antibody unique and specific to a single antigen. Each B lymphocyte is thus capable of reacting to a specific antigen, should it ever encounter that antigen. Initially it may seem that a system in which each B lymphocyte is responsible only for a single antigen might be somewhat inefficient, but as a whole, a person’s B-lymphocyte pool may display as many as 10 million different attachment configurations for different antigens, rendering it fully capable of expanding to the size necessary to function adequately.
Within the described populations of lymphocytes, a small population of cells is given the responsibility of “remembering” that the host has been in contact and processed an antigen in the past. These lymphocytes are referred to as memory cells. This allows the immune system to reduce its population of active lymphocytes during times when the host is not exposed to a particular antigen while not having to reinitiate the process of sensitization on subsequent exposures. Both B lymphocytes and T lymphocytes may become memory cells, storing the identity of the invading allergen and being able to recognize the pattern on subsequent appearances and institute appropriate defensive action. When one of these memory cells contacts an antigen to which it was sensitized, then the other components of the cellular and non-cellular adaptive immune response are rapidly expanded.
CYTOKINES: THE BODY’S CHEMICAL MESSENGERS
Virtually all of the immune system is regulated by the secretion of several chemical messages (protein hormones) known as cytokines, which allow for general communication between cells. Many subcategories of cytokines currently exist, giving rise to some nominal confusion at times, but all function in a similar fashion. The cytokines that are involved in the innate immune response are largely produced by mononuclear phagocytic cells, and are also known as monokines. In the case of an adaptive immune response to antigenic stimulation, activated lymphocytes produce cytokines, which are sometimes known as lymphokines. Yet another family of cytokines, which enhance the growth and differentiation of stem cells and immature bone marrow cells, are referred to as colony-stimulating factors. Further, because one of the principal sources of cytokines is the leukocyte, and because their biologic activity is primarily directed at other leukocytes, another group of cytokines are generically known as interleukins. Current terminology numbers these interleukins (ILs), so that common designations are IL-1, IL-2, etc. Although it is sometimes easy to become lost within the nomenclature of the various cytokines, it is important to remember that despite the nominal differences, all function in a very similar fashion to provide communication between various populations of cells within the body.
The generally accepted functions of cytokines are to (1) mediate natural immunity; (2) regulate lymphocyte activation, growth, and differentiation; (3) regulate immune-mediated inflammation; and (4) stimulate cell growth and differentiation. The effects and target cells of cytokines remain under active investigation, and this base of knowledge is constantly expanding. The serious student may consult other sources for more detailed information,1–3 but for purposes of this discussion, the general concept explained here will suffice.
COMPLEMENT SYSTEM
One further component of the immune system requires mention: the complement system. This is a group of enzymes that react in a cascade pattern when stimulated by an antigen that has attached to an invader, gaining strength and amplifying as the cascade progresses. An exact knowledge of the routes involved is rarely necessary for the clinician. The end result of complement activation is to produce one of three responses: (1) complement may aid the ingestion of offending cells (invaders or dying or diseased body cells) by the major phagocytes of the body; (2) complement reacts with various other immunologic components to produce direct cytolysis of invaders; or (3) complement may facilitate immune complex reactions, which are discussed in the following section on the malfunctions of the immune system involved in allergy. The complement system can be triggered in either a specific or nonspecific fashion, and therefore can contribute to either innate or adaptive immune responses.
Summary of the Immune System
This has been, despite appearances, a very cursory introduction to the basic functions of the immune system. Even so, trying to absorb even this much may seem daunting. How much of the previous information does one actually need to know to understand the position of allergy in the much larger field of immunology, and therefore how allergy can be diagnosed and treated? Certainly, not everything must be committed to memory. Reading it through to establish a familiarity with the terms should provide a reasonable introduction to the aspects of the immune system directly involved in allergy, and therefore of importance as background material to the clinician. One may then go back to review parts of the discussion as needed, if portions of the sections on testing and treatment become confusing.
ALLERGY AND THE IMMUNE SYSTEM
Allergy: Nature versus Nurture
Allergy, in a practical sense, is a malfunction of the immune system. The normally functioning immune system identifies true environmental threats to the body, as well as internal cellular disorders, and attempts to remove the offenders from the body. The allergic response occurs when the immune system identifies as dangerous an environmental exposure that does not actually present any threat to the host and, therefore, institutes defensive action. The defensive action may be limited, or it may be greater than that needed to defend against true offenders. This situation, in part, appears to be genetically influenced. In other words, the potential for development of an excessive response to harmless exposures, such as dust, molds, pollens, and certain foods, may be predetermined in each individual. If the exposure to a potential allergen does not occur, the individual will never show a response. (In the allergic patient, “antigens” are frequently referred to as “allergens,” as they are capable of inducing an allergic reaction.) Conversely, if the individual is exposed to a substance to which no antigenic attachments exist in that person’s immune system, that person cannot become allergic to the substance.
Although genetics appears to play a large role in the potential to develop allergy, recent epidemiologic studies suggest that this process may also be partially under the control of early environmental exposures. This information has been augmented by the recent realization that two populations of T-helper lymphocytes exist that can only be differentiated by the array of cytokines that they are able to produce. One population of T-helper lymphocytes (TH1 cells) produces a profile of cytokines that promote an immunologic response targeted against bacterial invaders. The other population of T-helper lymphocytes (TH2 cells) produces a profile of cytokines that direct cellular and noncellular components of the immune system to respond in an “allergic” fashion. Because these two distinct populations of T-helper lymphocytes are derived from the same pool of cells, it appears that environmental experiences that are encountered early in life such as bacterial infection, hygiene, and antibiotic exposure may influence an individual’s ratio of TH1 to TH2 cells. It has been suggested that those individuals who have a high TH1/TH2 ratio are less likely to develop allergy, whereas those with a lowTHl/TH2 ratio are much more likely to develop allergy and asthma. This theory is referred to as the hygiene hypothesis.
Although it is true that most allergic patients do respond to a variety of offenders, the lay designation of the patient who is “allergic to everything” does not exist. The potential number of allergens to which any one person may react is large but limited. This fact may be of some importance in preparing a testing program for a patient. Although sensitization may occur at any stage of life, and rarely occurs on limited or early exposures, a patient who has lived for years in the same place with no significant change in activity or occupation will usually have had enough exposure to the potential allergens present to induce a reaction, if one can occur. If the patient has had extensive testing and treatment and has been doing well, and suddenly has a marked increase in allergy symptoms, it is rarely necessary to repeat the previous tests. Instead, a diligent search for a new exposure and sensitization is indicated.
TYPES OF ALLERGIC MECHANISM
It is common to think of allergy as a disease that is immunoglobulin E (IgE) mediated. Allergy, however, may appear as a malfunction of many parts of the immune system, and frequently more than one mechanism is involved. The complexity of the problem led two investigators, Gell and Coombs, to divide allergic reactions into four types. Although not a perfect delineation, as it is quite possible for more than one reaction to occur simultaneously, the designation is of great use in understanding and treating allergy.
Type I Reactions
Type I allergy (Fig. 2-1), also known as atopy or immediate hypersensitivity, is the best-known form of allergy and is the type usually associated by the public with the diagnosis of allergy. As far as is known, all inhalant allergy is a type I reaction. A small percentage of food allergy represents a type I reaction. Insect sting allergy is also type I, as is penicillin sensitivity. This is the only potentially life-threatening form of allergic reaction commonly seen, and it can proceed to anaphylactic shock and death. Type I reactions are produced by IgE, which is present in greater than trace amounts in an estimated 20 to 30% of the population. This type of allergy is the only form that can be diagnosed reliably by skin testing and also by in vitro testing, leading a large percentage of the allergy community to consider this condition the only true form of “allergy” and to refer to all other adverse reactions by a different designation. (The controversy about the definition of allergy is discussed in some detail in Chapter 13.)
Type I allergy produces an immediate reaction in most cases, occurring within seconds to minutes. If the target organ is the upper respiratory tract, the classic “hay fever” pattern will be seen, with extensive sneezing, rhinor-rhea, often conjunctivitis, and itching. If the target organ is the lower respiratory tract, cough, increased sputum, and wheezing may occur. Systemic type I reactions may include urticaria, angioedema, and, in the extreme case, anaphylactic shock that can result in death.
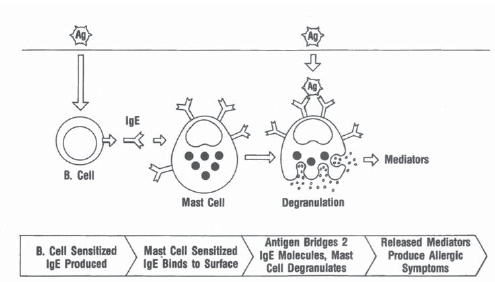
Figure 2-1 Gell and Coombs type I hypersensitivity reaction. An antigen passing through the respiratory or gastrointestinal mucosa sensitizes a B lymphocyte, which, in turn, initiates production of immunoglobulin E (IgE). The IgE binds to the surface of mast cells, sensitizing them. A second exposure to the antigen results in bridging of the IgE molecules and triggers degranulation of the mast cell, resulting in the release of mediators that produce hay fever, asthma, urticaria, etc. (Adaptedfrom RoittIM, Brostoff], Male DK. Immunology. 4th ed. London: Mosby; 1996; and Mygind, N. Essential Allergy. Oxford: Blackwell Scientific Publications; 1986.)



