CHAPTER 15
Allergy and Sinus Disease
Although the complaint “Doctor, I have sinus” is commonly heard by the otolaryngologist, the exact meaning of “sinus” to a patient remains a highly individual matter. Some of these patients have primary complaints that represent allergy. Others have infection, nonallergic rhinitis, or even migraine headaches. Therefore, the most important initial step is to establish the exact symptoms that are troubling the patient, the chronology of the illness, and, if applicable, the response to various previous therapeutic attempts. In other words, the presence or absence of active sinus disease must be determined by a history, physical examination, and appropriate ancillary tests (endoscopy; radiographic studies). This chapter assumes that all this has been done, and that the patient indeed does suffer from some form of sinusitis. In such instances, there is often a distinct relationship between such sinus problems and allergy, and it behooves physicians engaging to treat these patients to understand and address this relationship. To do so ensures better results, and to ignore such a concordance increases the chance of a poor therapeutic outcome or a rapid recurrence of symptoms.
ROLE OF THE OSTIOMEATAL COMPLEX
The concept of the ostiomeatal complex (OMC) as the key to sinus disease is generally attributed to the work of Messerklinger.1 Even earlier, however, Proctor2 underscored the importance of the ethmoids and infundibulum as the key structures in producing disease in other sinuses. The OMC is located in the middle meatus and represents the region into which empty the maxillary, anterior ethmoid, and frontal sinuses. It is bounded by the ethmoid bulla, the uncinate process, and the middle turbinate (Fig. 15-1). Although anatomic abnormalities may result in OMC blockage, by far the most frequent cause of such obstruction is mucosal edema. Edema may be caused by infection, allergy, or various nonatopic triggers. It is worth emphasizing that not all sinus disease is related to obstruction or dysfunction of the OMC. Host factors (e.g., immune deficiency, diabetes, etc.) may also play a role. The message to bear in mind is that sinusitis may be due to numerous factors (Table 15-1), some of which may respond to surgery, whereas others will not. Unless allergy is appropriately ruled out or adequately treated, the patient with recurrent or chronic sinusitis may experience less than optimum results from medical and/or surgical management.
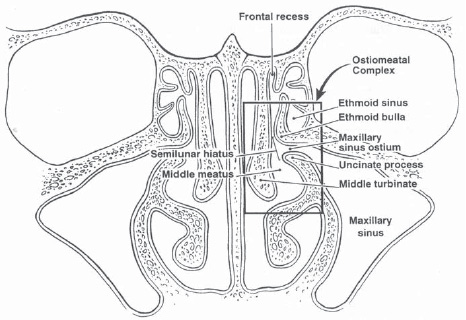
Figure 15-1 The ostiomeatal complex (area within the box), which is of key importance in the prevention and management of sinus disease.
RELATIONSHIP OF ALLERGY AND SINUSITIS
There has been gradual acceptance that allergy may be a significant contributor to sinus disease. In 1995, Slavin3 reviewed the concordance of allergy and sinus disease (as high as 75% in some series) and indicated that this finding, significantly more frequent than the prevalence of allergy in the general population, “supports the impression that allergy is an important associated and probably predisposing factor in sinusitis.” In one study, patients with acute sinusitis showed a significantly higher number of positive results on allergy skin tests in comparison with control groups.4 In children, a high correlation between allergy and sinus disease has also been demonstrated.5,6 Such studies have made it clear that it is no longer necessary to defend the practice of investigating and treating allergy in every patient with sinus disease. Rather, to omit such a consideration would appear to be questionable.
I. Outflow tract obstruction |
A. Mechanical |
1. Septal deviation |
2. Mass lesions (polyps, tumors, foreign body) |
3. Middle turbinate abnormalities (paradoxical, concha bullosum) |
4. Lateral nasal wall abnormalities (uncinate, extramural ethmoid cells) |
B. Pathophysiologic |
1. Infection |
2. Allergy |
3. Rhinitis medicamentosa |
4. Hormonal aberrations |
5. Idiopathic (vasomotor) rhinitis |
6. Ciliary dyskinesia |
7. Mucosal damage |
II. Pathogen exposure |
A. Frequency |
1. Health care workers |
2. School teachers, day-care workers |
3. Parents and siblings of small children |
4. Flight crews, salespersons |
B. Type of pathogens |
1. Drug sensitive |
2. Drug resistant |
III. Impaired host resistance |
A. Immune deficiency (primary, acquired) |
B. Constitutional factors (diabetes mellitus, anemia) |
IV. Other contributory factors |
A. Trauma (swimming, diving, nasal intubations) |
B. Irritation (smoke, pollution) |
Allergy may affect the sinuses in three ways: by the direct effect of the a llergic event, by enhancing reactivity (or priming), and by contributing to the formation of polyps.
Direct Effects of the Allergic Reaction on Sinuses
An acute Gell and Coombs type I, immunoglobulin E (IgE)-mediated allergic event results in the release by tissue mast cells and basophils of both preformed and newly formed mediators of inflammation. These include inflammatory agents (e.g., histamine, platelet activating factor, tryptase, kinins), spasmogens and mucous secretagogues (e.g., prostaglandins, leukotrienes), and cellular attractants (neutrophil and eosinophil chemotactic factors). This process results in an acute reaction characterized by mucosal edema, mucus secretion, and vasodilation with increased vascular permeability. A late stage, marked by cellular influx, maintains many of these circumstances. As a consequence of such a reaction in the nasal mucosa, obstruction of the OMC may occur. The increased production of mucus by the sinus mucosa is trapped within the various sinus cavities, resulting in stagnation. These thick secretions form a medium for the aerobic and/or anaerobic growth of pathogens, setting the stage for secondary infection or perpetuating existing infection. Thus, in patients with borderline competence of the OMC, allergic reactions and the edema and hypersecretion that accompany them may tip the balance from adequate function to disease.
Allergy and Altered Responsiveness (Priming)
In 1968, Connell7 reported his observations that in pollen-allergic patients, more nasal symptoms (especially obstruction) were produced by the same amount of pollen exposure at the end of a pollen season than at its beginning. He called this phenomenon priming. He found it to be related to the degree of allergen exposure (i.e., threshold lowered more by larger allergen challenges). It was specific to the challenged mucosa, so that if only the lower airway was challenged, no priming was exhibited by the nasal mucosa. Connell also found that the affected mucosa demonstrated heightened sensitivity to challenges by other stimuli. The phenomenon was reversible, ceasing after allergen challenges were discontinued.
The mechanism of priming has been clarified by further studies.8 It appears to result from the release of additional mediators, such as histamine, TAME esterase, and prostaglandin D2, caused by an increased influx of inflammatory cells.
It has been shown that priming can affect eustachian tube function.9 The parallel between the eustachian tube and the OMC is readily apparent. Thus, it certainly seems logical that repeated allergic challenges and untreated allergic reactions could adversely affect the function of the narrow channel through which the key sinuses ventilate and drain. It follows that appropriate management of allergy, including the prevention of the allergic reaction whenever possible, should be part of the management of sinusitis.
ALLERGY AND POLYPS
In the early days of our specialty, polyps were classified as being of “allergic” or “inflammatory” origin, based on the presence or absence of eosinophils within their stroma. More recently, the view formerly espoused that all polyps have an allergic origin has given way to the opinion voiced by Slavin10 that allergy occurs infrequently and independently in patients with nasal polyps, and that “the routine allergic evaluation of patients with nasal polyps should be discouraged in the name of health care cost containment.”
Other reported observations indicate that polyp development begins as epithelial rupture (caused by edema).11 Tissue prolapse, the development of a vascular stalk, and epithelialization of the prolapsed tissue follow, resulting in the formation of a full-blown polyp. The cause of rupture can be trauma, infection,12 allergy,13 or a combination of factors.
The fact remains that allergy may be a cause (possibly a very significant one) of sinonasal polyps. The review by Slavin that led him to the conclusion that allergy is not a significant factor in polyp development included allergy testing primarily by prick/puncture methods. Although prick testing is generally adequate to diagnose significant degrees of sensitivity to inhalant antigens, negative prick test results must be followed by intradermal tests (which are much more sensitive) before the true absence of atopic skin reactivity can be confirmed. In addition, the material reviewed by Slavin did not include investigation for food allergy, which may influence polyp development. Thus, his evaluation of a possible effect on polyps may have significantly underestimated the incidence of allergy in the populations considered.
An interesting phenomenon is the presence of allergen-specific IgE in the nasal mucosa and/or polyps of patients with no systemic evidence of allergy.14 This suggests that in some patients local allergy may play a role in sinonasal polyposis.
Certainly, experienced rhinologists who deal with allergy have made the clinical observation (unfortunately, unconfirmed thus far by scientific studies) that in patients in whom allergy and polyps coexist, appropriate management of the allergy significantly lessens the likelihood of polyp recurrence. Therefore, as a practical matter, all patients with rhinosinusitis and nasal polyposis should have some sort of allergy workup. This may be as simple as a thorough history with attention to indicators of allergy, or as complex as complete evaluation for inhalant and food sensitivity.
PHARMACOTHERAPY FOR ALLERGY IN THE PATIENT WITH SINUSITIS
Some consideration must be given to the effect of concomitant allergy and sinus disease when various medications are considered in these patients.
Antihistamines
For years, it was thought that antihistamines should not be administered to patients with sinusitis, lest these compounds thicken nasal secretions, thereby contributing to stagnation of secretions and crust formation with obstruction. For similar reasons, the use of antihistamines in asthmatic patients was questioned. This idea remains valid in regard to the administration of conventional, first-generation (sedating) antihistamines, which have significant anticholinergic side effects. However, the second-generation preparations, such as loratadine, cetirizine, and fexofenadine, are essentially free of this side effect and may safely (and effectively) be used to provide symptomatic relief in patients with allergy and sinus disease and/or asthma.15
It has been shown that the administration of either of the antihistamines terfenadine and astemizole concurrently with either of the macrolide antibiotics erythromycin and troleandomycin, which are also metabolized by the cytochrome P-450 oxidase system, may result in cardiac arrhythmias, such as torsades de pointes, in a very small percentage of patients.16 This warning has not been extended to some of the newer macrolides, such as clarithromycin and azithromycin. Other compounds, most notably systemic antifungals, may also produce arrhythmias when given with terfenadine or astemizole. Both terfenadine and astemizole have been withdrawn from the U.S. market, and all antihistamines introduced subsequent to this time have been subjected to careful scrutiny regarding their cardiac effects when given with various antibiotics and antifungals. Although this caution is now mainly of historic interest, it serves as a warning and a caution when administering antibiotics to patients receiving concomitant medications for other problems, such as allergy.
Decongestants
Patients with both allergy and sinusitis experience nasal obstruction as a result of the disease process. Because both problems tend to be chronic, these patients are more prone than others to become dependent on topical nasal decongestants, producing a “rebound rhinitis.” This may occur in as little as 5 to 7 days. One study (using normal volunteers, not patients with rhinitis) has suggested that restricted usage of a long-acting preparation (e.g., oxymetazoline) for even longer periods may not produce a rebound phenomenon.17 Nevertheless, until further work confirms this, it is best to utilize systemic decongestants, rather than topical preparations, in patients with allergy and/or sinus disease.
Mucolytics
Although only limited clinical studies support the use of mucolytics in treating sinusitis,18 most physicians (based on clinical experience) routinely employ them (e.g., guaifenesin) to thin secretions that have become thick and tenacious, thereby aiding sinus drainage and evacuation of secretions. However, patients with associated allergy may often complain that these drugs are making their allergy worse, as the end result that they perceive is an increase in thin nasal secretions. A word of forewarning is generally sufficient to result in patient acceptance of this treatment, when needed.
Mast Cell Stabilizers
The prototype of this category of drugs, cromolyn, is an excellent preventive agent in the treatment of allergic rhinitis. Appropriate use of cromolyn before an anticipated allergy exposure may prevent a priming phenomenon caused by repeated allergic events. In a few fortunate patients with allergy and recurrent sinusitis who have borderline obstruction of the OMC, preventing the direct effects of the allergic reaction already described by the regular use of a mast cell stabilizer may permit adequate sinus ventilation and drainage, thereby avoiding the need for surgical intervention.
It should be pointed out that cromolyn is not effective in the treatment of polyps, nor does it have a primary antiinflammatory effect (such as is exhibited by corticosteroids). As pointed out later, if patients are placed on nasal corticosteroids, the use of cromolyn becomes redundant.
Finally, in our experience we have noted that patients using cromolyn in the face of active nasal and sinus infection often complain that it produces a nasal burning. This should cause the clinician to suspect infection strongly and treat it appropriately.
Corticosteroids
These potent antiinflammatory drugs are frequently effective in treating rhinosinusitis from a variety of causes, not just allergy. As pointed out in Chapter 7 on pharmacotherapy, appropriate instruction of the patient regarding the proper use of corticosteroids is required, as well as monitoring to ascertain the need for their continued use and to watch for undesirable topical or systemic effects.
At least theoretically, corticosteroids inhibit the body’s natural defense against infection through their effect on the inflammatory response. However, recent work has shown that topical nasal corticosteroids actually enhance recovery from infectious sinusitis when given in conjunction with antibiotics. Thus, there appears to be no need to discontinue their use in patients with allergy who develop an active purulent sinusitis.
IMMUNOTHERAPY IN THE PATIENT WITH SINUSITIS
Because of the concordance between allergy and sinusitis, many patients with sinus disease are candidates for immunotherapy. When the appropriate treatment of the sinus disease fails to produce adequate resolution and surgery is indicated, the question that constantly arises is whether these injections should be begun before surgery or afterward. Ideally, allergy therapy should be instituted 6 to 12 weeks before surgical intervention is employed. This is not to make the surgery unnecessary (although, happily, that is sometimes the result). Rather, addressing allergy before surgery and continuing the therapy after surgery provides the greatest likelihood of a desirable long-term result.19
If the need for surgical intervention is pressing, immunotherapy may be begun after surgery. However, these patients should be urged to start allergen avoidance and environmental control measures at the earliest possible moment. Likewise, appropriate pharmacotherapy should be instituted. If surgery must precede immunotherapy, it is best to wait for about 4 weeks to do any skin testing or begin allergy injections, to allow the immune system to normalize after the stress of surgery.
It is important, when immunotherapy is begun in patients with both allergy and sinus disease, to be certain that all parties concerned understand the indicators of success. Some of these patients may not have “typical” allergic symptoms of rhinorrhea, sneezing, and pruritus. If they understand that their allergy treatment is aimed at preventing episodes of hypersecretion and mucosal edema, however, they will be able to appreciate the benefits of fewer “sinus”-type symptoms.
Patients on immunotherapy, in whom an active infection develops involving the nose and sinus, frequently demonstrate increased (and often unacceptable) local reactions at their injection sites, with no change in antigen dose or allergen exposure. This may call for a brief dose adjustment or even the omission of injections for a week or so, and it should also trigger a search for and appropriate treatment of the infection. Rarely do these episodes significantly alter the overall course of immunotherapy. However, the allergy nurse or assistant should be constantly alert for situations in which large local reactions occur for no apparent reason (such as an increased exposure to allergens or a change in dose). When this occurs, the possibility of an infection should be entertained, and the patient should be seen by the physician if necessary for further evaluation.
NURSE’S NOTE
Allergy nurses and assistants should be alert to the situation in which a patient, for no apparent reason, begins to have significant local reactions after allergy injections. If these patients have experienced no increased antigen exposure or had no change in their dosage, the possibility of a complicating infection should be strongly considered. Most patients receiving allergy injections tend to blame all their nasal symptoms on allergy and never consider that infections may produce similar problems, It is heipful to encourage these patients to see the physician to check this possibility, and to assess the reason for their local reactions.



