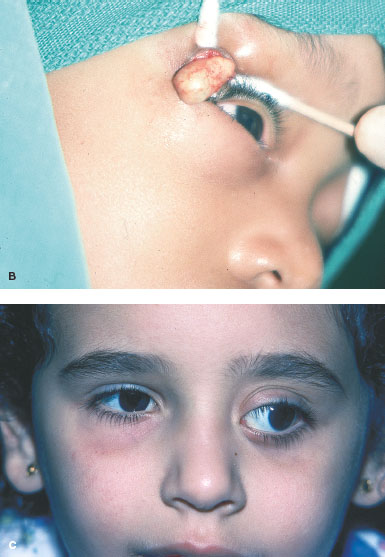
FIGURE 14-1. Dermoid cyst. A. Soft, mobile mass along the superior temporal rim in a 1-year-old patient. This has been present since birth. Dermoid cyst. B. Excision of the dermoid through a lid crease incision. C and D. Proptosis and globe displacement caused by a deep orbital dermoid, which was noted at age 5 years. The fossa formation caused by these lesions is seen on the CT scan. The deep orbital location means they are often not noticed until the child is older. This was completely excised and the patient did well without any further problems. Dermoid cyst. D. CT scan show cystic lesion with bony fossa formation. E. MRI of a dermoid cyst. On a T2-weighted image, the cyst is hyperintense to fat and muscle.
LIPODERMOIDS
Lipodermoids are congenital solid tumors located temporally below the conjunctiva. These are sometimes not noted until later in life. They should be left alone in almost all cases.
Epidemiology and Etiology
• Age: Congenital
• Gender: Equal occurrence in males and females
• Etiology: Developmental anomaly
History
• Present at birth and generally does not change with time
Examination
• Yellowish, pink lesion over the lateral surface of the globe deep to the conjunctiva (Fig. 14-2)
• They vary in size and often have hairs on the surface.
Imaging
• If large, CT scan will show a mass with fat density.
Differential Diagnosis
• Fat prolapse
• Lymphoma
• Prolapsed lacrimal gland
Pathology
• Keratinizing squamous epithelium with adnexal structures
• The underlying dermis usually contains fat and connective tissue.
Treatment
• No treatment
• Attempted excision can damage the adjacent lacrimal ducts and rectus or levator muscles.
• In rare cases when the lipodermoid is very large, the anterior portion can be debulked leaving the conjunctiva unresected.
Prognosis
• Excellent if left alone
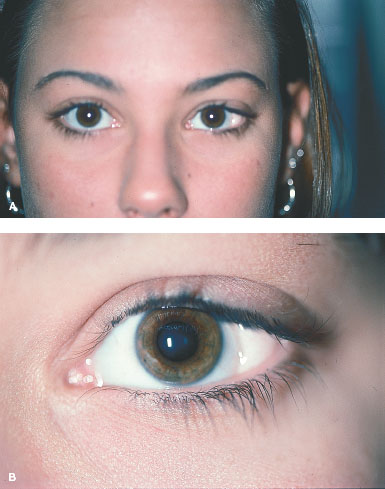
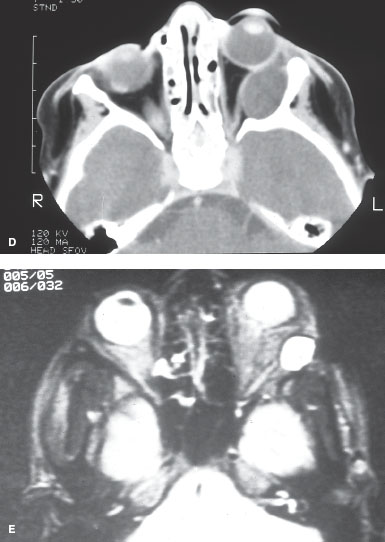
FIGURE 14-2. Lipodermoid. A. Classic location for a lipodermoid, which has been present since birth. B. Close inspection often shows hairs on the lesion. Despite the cosmetic appearance, these are best left alone.
VASCULAR ORBITAL TUMORS
CAPILLARY HEMANGIOMAS
Capillary hemangiomas are benign tumors of the orbit that appear in the first few weeks of life and enlarge over the first 6 to 12 months. They then tend to shrink over time but the initial presentation can be dramatic.
Epidemiology and Etiology
• Age: Noted in the first year of life
• Gender: Equal occurrence in males and females
• Etiology: Abnormal growth of blood vessels with varying degrees of endothelial cell proliferation
History
• Lesions are often noted in first few weeks of life and they grow, sometimes rapidly, over weeks to months.
• They can present deeper in the orbit with proptosis or more superficially as an expanding mass.
• The hemangioma will then involute over months to years. Seventy-five percent of lesions will resolve over 4 years.
Examination
• The lesion appearance is dependent on the location (Fig. 14-3A-C, F, G).
• The more common superficial lesions produce an elevated, dimpled, strawberry-colored lesion.
• Deeper lesions may give a bluish discoloration.
• Deep orbital lesions may only give symptoms of an expanding orbital mass.
• Differentiation between rhabdomyosarcoma and deep capillary hemangioma can only be made with biopsy.
Imaging
• CT scan reveals a mass that can be well or poorly marginated with enhancement with contrast (Fig. 14-3D, E).
• MRI is hypointense on T1 and hyperintense on T2.
• The lesion enhances with gadolinium.
Differential Diagnosis
• Rhabdomyosarcoma
Pathology
• Proliferation of endothelial cells organized into a network of basement membrane–lined vascular channels.
Treatment
• These lesions will regress so hemangiomas are observed for regression unless they cause visual obstruction or astigmatism leading to amblyopia.
• In this case, treatment is required.
• Orbital lesions causing severe proptosis may also require treatment.
• Orbital biopsy is required if the lesion cannot be differentiated from a rhabdomyosarcoma.
• Treatment options include intralesional steroid injection, systemic steroids, or, in select cases, surgical excision.
• Recent studies suggest systemic propranolol may become the treatment of choice.
• Careful monitoring of these babies on propranolol must be done by pediatric cardiology.
Prognosis
• Good
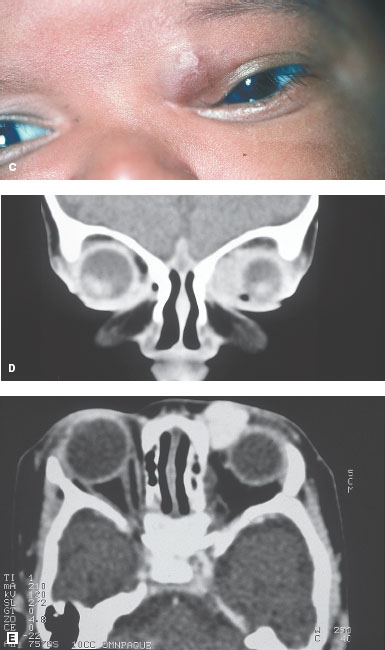

FIGURE 14-3. Capillary hemangioma. A. Subcutaneous capillary hemangioma of the right eyebrow that increased in size over 6 months. The lesion becomes more prominent and red with crying. This lesion resolved over 3 years. B. A small hemangioma on the child’s arm. Capillary hemangioma. C. Superficial orbital hemangioma that had increased in size and was causing amblyopia from 7 diopters of induced astigmatism. D and E. CT scans show this anterior orbital mass, which is well circumscribed and enhances with contrast. This was excised because of the astigmatism and amblyopia. Capillary hemangioma. F. Large cutaneous capillary hemangioma with visual obstruction. G. This lesion responded well to a series of intralesional steroid injections.
CAVERNOUS HEMANGIOMAS
Cavernous hemangiomas can present as asymptomatic, very insidious onset proptosis. More commonly, these lesions present without any symptoms and are found on imaging done for unrelated reasons. They are slowly growing masses that are generally easy to remove depending on their location.
Epidemiology and Etiology
• Age: Adults
• Gender: Most commonly middle-aged women
• Etiology: Unknown
History
• Very slow growth usually means the patient is unsure of the onset or duration of the lesion.
• Most commonly, the presentation is proptosis but rarely there can be symptoms of visual loss.
Examination
• Axial proptosis is the common presentation.
• If the lesion is at the apex or is very large, it can cause optic nerve compromise (Fig. 14-4A-C) or strabismus.
• Lesions can rarely cause orbital pain or the appearance of a choroidal mass.
Imaging
• CT scan shows an encapsulated, homogeneous, round mass with variable enhancement.
• MRI: isointense on T1 and hyperintense on T2(Fig. 14-4D, E).
• Marked enhancement with gadolinium
Special Considerations
• Rarely, lesions may grow rapidly during pregnancy.
Differential Diagnosis
• Hemangiopericytoma
• Schwannoma
• Fibrous histiocytoma
Pathology
• Encapsulated tumor consisting of large endothelial lined channels with abundant, loosely distributed smooth muscle in the vascular walls and smooth muscle.
Treatment
• Surgical excision is the treatment of choice.
• These lesions are easily removed once exposed.
• They do not regress and slowly enlarge so observation only delays surgery.
Prognosis
• Excellent
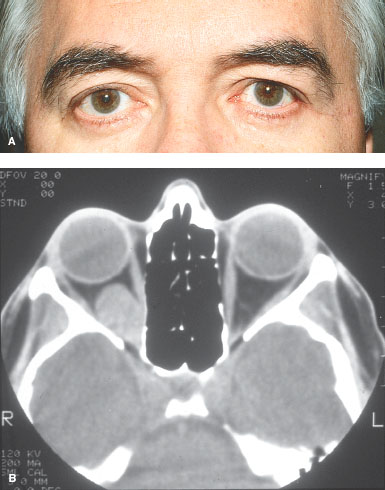
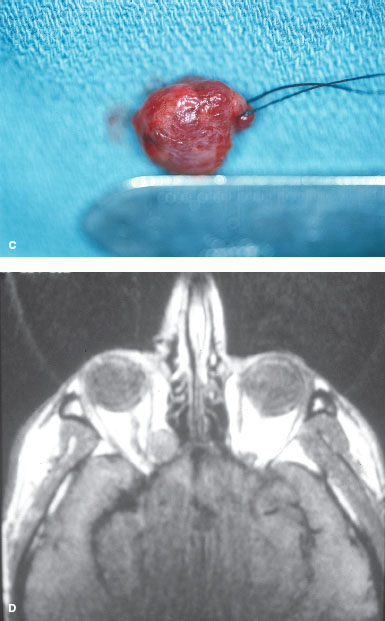
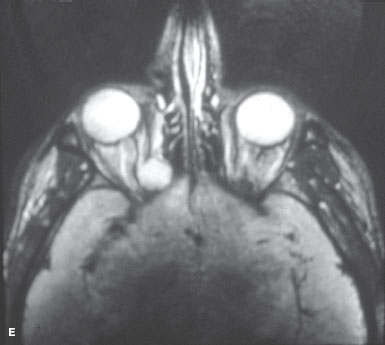
FIGURE 14-4. Cavernous hemangioma. A. A patient with proptosis of the right eye of unknown duration and no other visual or orbital complaints. B. CT scan shows a well-circumscribed intraconal orbital mass. Cavernous hemangioma. C. The mass was excised and was a cavernous hemangioma. D. MRI of a cavernous hemangioma. The T1-weighted image shows the lesion isointense to muscle and hypointense to fat. Cavernous hemangioma. E. On the T2-weighted image, the lesion is hyperintense to fat and muscle.
LYMPHANGIOMAS
Lymphangiomas are rare vascular hamartomas that can behave in many different ways depending on location and growth patterns. This condition can vary from mild rather asymptomatic lesions, to progressively growing, infiltrative lesions, to acute proptosis and visual loss from bleeding into these lesions.
Epidemiology and Etiology
• Age: Usually noted in the first decade of life
• Gender: More common in females
• Etiology: Congenital lesion
History
• These lesions are often noted associated with a spontaneous bleed of the lesion although they likely were present for years prior.
• They can grow slowly and then suddenly hemorrhage.
• Lymphangiomas can manifest as pain, subconjunctival hemorrhage, or as proptosis. Less commonly, the cysts of these lesions are noted subconjunctivally.
• These lesions enlarge with upper respiratory infections.
Examination
• The findings on examination are dependent on the location of the lesion.
• The most common presentation is associated with sudden bleeding into the lymphangioma.
• If the bleed is superficial, then a subconjunctival bleed is seen and the cysts of the lymphangioma are often found (Fig 14-5A, B). If the hemorrhage is in the orbit, the findings may only be proptosis (Fig 14-5C).
• Careful evaluation for evidence of a lymphangioma superficially should be done in these cases. Imaging will aid in the diagnosis if the lesion is entirely orbital.
Imaging
• CT scan: Poorly circumscribed, heterogeneous mass
• MRI: Hyperintense on T1; very hyperintense on T2, with possible area of fluid and blood (Fig. 14-5D, E)
Special Considerations
• Surgery performed on a lymphangioma increases the chances of spontaneous bleeds within the lesion.
• Surgery should only be done if absolutely necessary.
Differential Diagnosis
• Diagnosis can usually be made with MRI.
Pathology
• Nonencapsulated mass with large serum-filled spaces lined by flat endothelial cells
• The interstitium has scattered lymphoid follicles.
Treatment
• Observation unless the spontaneous bleeding causes visual loss, corneal exposure, or severe cosmetic disfigurement.
• Generally, with time the blood will resorb.
• When an orbital hemorrhage causes visual loss, drainage of the hemorrhage should be performed.
• Debulking of the lesion or orbital decompression are other treatment options.
• Lymphangiomas are infiltrative so excision is very difficult and there is usually significant bleeding associated with excision, which is only performed as a last resort.
Prognosis
• Variable depending on the growth of the lymphangioma
• Progressive lesions have a high incidence of visual disability and poor cosmetic result.
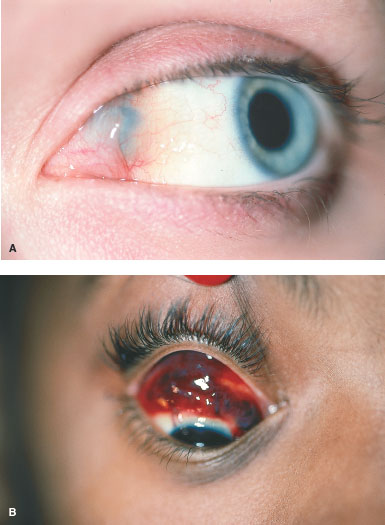
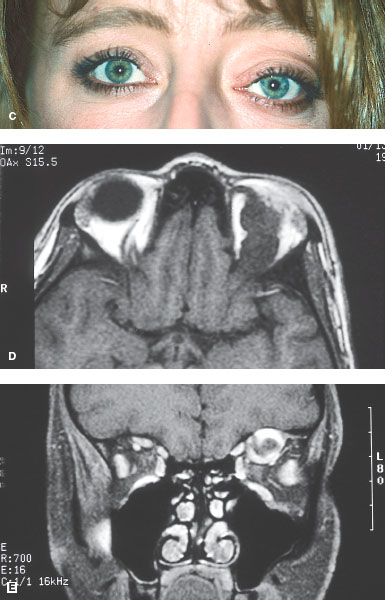
FIGURE 14-5. Lymphangioma. A. Patient with sudden onset of orbital discomfort and proptosis. Medially, a small area of hemorrhage is noted with subconjunctival cysts consistent with a lymphangioma. B. More obvious hemorrhage was noted along with the onset of deep orbital pain. Multiple cysts can be seen in the hemorrhage. Imaging was consistent with a lymphangioma. Lymphangioma. C. Proptosis of the left eye with recurrent episodes of orbital pain. The pain was usually associated with an increase in the proptosis. D and E. MRIs show a superior orbital mass with area of fresh and old blood consistent with a lymphangioma.
HEMANGIOPERICYTOMA
Hemangiopericytoma is a rare lesion that can mimic a cavernous hemangioma but has more rapid growth and is more likely to cause symptoms. These can recur and have a chance of metastasis.
Epidemiology and Etiology
• Age: Middle age
• Gender: Equal occurrence in males and females
• Etiology: Tumor originates from the pericyte. This is a rare orbital tumor.
History
• Insidious onset of proptosis and mass effect but usually more rapid onset than a cavernous hemangioma
Examination
• Proptosis is often the only finding.
• These lesions appear more often in the superior orbit but intraconal location is also common (Fig. 14-6A, B).
Imaging
• CT scan: well-circumscribed, encapsulated mass
• MRI: isointense on T1; hyperintense on T2 (Fig. 14-6C, D).
• Enhances with gadolinium
Special Considerations
• These lesions have the potential for recurrence locally whether the pathology is benign or malignant.
• Malignant lesions can recur and can also metastasize.
Differential Diagnosis
• Cavernous hemangioma
• Fibrous histiocytoma
• Schwannoma
Pathology
• Uniform spindle-cell tumor with a sinusoidal vascular pattern; can be divided into benign, intermediate, and malignant forms.
Treatment
• Complete excision in the capsule is the best treatment.
• Recurrence, if malignant, may require exenteration.
Prognosis
• Variable. Patients must be followed for at least 10 years for local recurrence or metastasis.
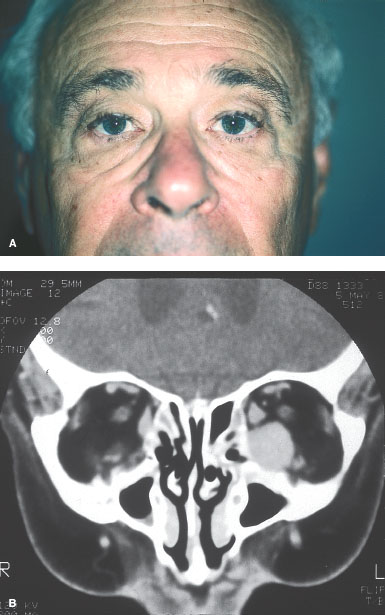
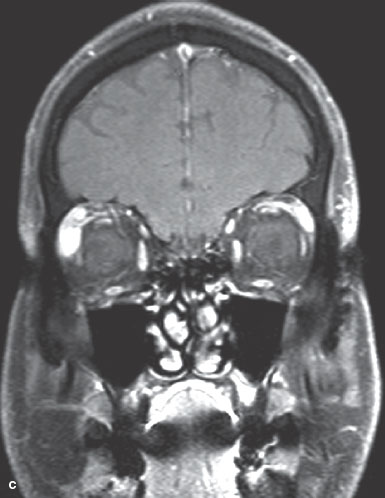
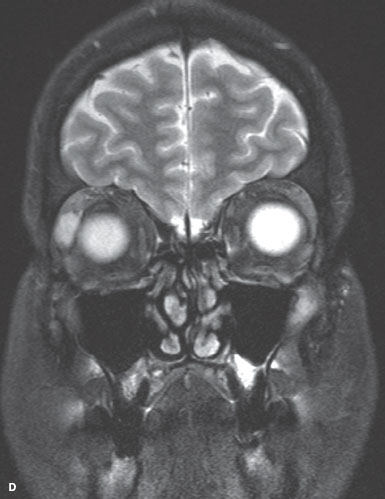
FIGURE 14-6. Hemangiopericytoma. A and B. A 55-year-old man presented with increasing proptosis over 6 months and diplopia. There is axial proptosis on the left and a well-circumscribed mass on CT scan. Pathologic examination revealed a hemangiopericytoma. Hemangiopericytoma. C. T1-weighted coronal MRI with contrast and fat suppression shows a hemangiopericytoma next to the right lacrimal gland. Hemangiopericytoma. D. T2-weighted coronal MRI of the same hemangiopericytoma next to the right lacrimal gland.
ORBITAL VARICES
Orbital varices will present in the 20s and 30s with a history of years of intermittent proptosis. These lesions can be superficial and noticeable or deep with only proptosis as a sign of the lesion. Most lesions should be left alone unless there is extreme orbital pressure with functional deficit or a severe cosmetic disfigurement.
Epidemiology and Etiology
• Age: Usually noted in the first through third decades of life
• Gender: Equal occurrence in males and females
• Etiology: Dilatation of pre-existing venous channels
History
• Patients with nondistensible varices present with recurrent episodes of thrombosis and hemorrhage in the lesion (Fig. 14-7E, F).
• This leads to proptosis, pain, motility restriction, and even decreased vision. These symptoms resolve as the hemorrhage resolves.
• The distensible varices present with pain, proptosis, and pressure symptoms associated with straining, bending forward, or Valsalva (Fig. 14-7A, B).
• The changes in the orbit and lids associated with this venous distension are also noted.
Examination
• Distensible varices are diagnosed easily by having the patients bring their head into a dependent position and note the filling of the varix.
• Nondistensible varices are more difficult to diagnose.
• The patient will present with symptoms of an acute hemorrhage into the lesion as noted previously.
• There is generally no external hemorrhage present or any sign of a varix in this type.
Imaging
• CT scan may appear relatively normal or with just a small diffuse mass on axial cuts.
• In the dependent position (coronal cuts), the mass will enlarge as the varix fills with blood (Fig. 14-7C, D).
• Nondistensible varices will show a diffuse mass that enhances with contrast.
Differential Diagnosis
• Lymphangioma is the main differential and differentiation from the nondistensible varix is not always possible.
Pathology
• Well-defined venous channels
Treatment
• Conservative observation in most cases
• If a nondistensible varix bleeds and visual or exposure symptoms require intervention, drainage of the blood clot is usually the treatment of choice.
Prognosis
• Variable. Progressive lesions can be disfiguring and successful treatment is difficult.
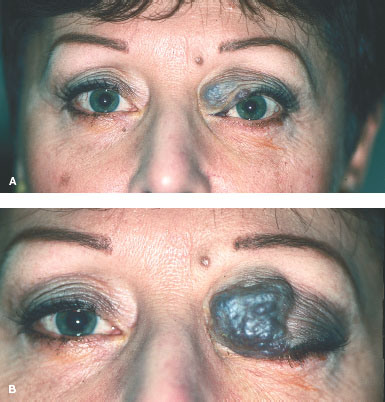
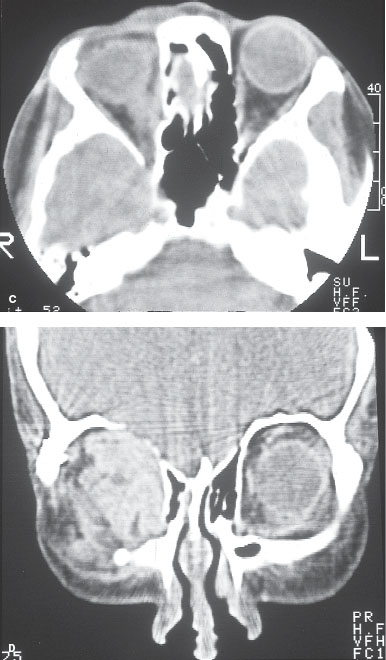
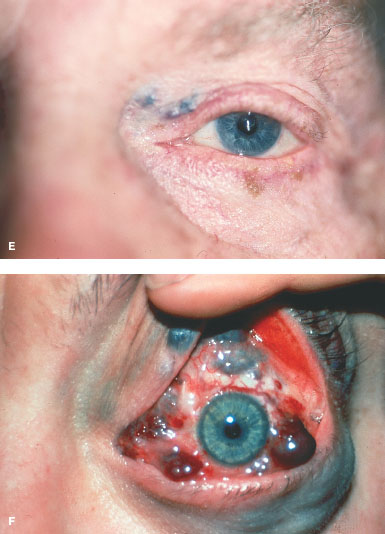
FIGURE 14-7. Distensible orbital varix. A. A 55-year-old woman with a distensible varix in her superior medial orbit. B. Valsalva results in massive enlargement and closure of the eye. Distensible orbital varix. C. CT scan showing the medial orbital varix. D. When the head is placed in a dependent position for the coronal CT, the varix fills with blood, accounting for the enlargement of the lesion on the coronal cuts. Distensible orbital varix. E. Nondistensible varix may be deep in the orbit with only a small anterior component. F. Diffuse orbital involvement with multiple varices.
ARTERIOVENOUS MALFORMATIONS
Arteriovenous malformations (AVM) present with variable severity. All cases involve the connection of an arterial flow into a venous drainage area such as the cavernous sinus. There may be subtle swelling and redness of the eye and orbit or the presentation may be severe proptosis, exposure, and intraocular vascular congestion.
Epidemiology and Etiology
• Age: Older adults, except after trauma, which can occur at any age
• Gender: Equal occurrence in males and females
• Etiology: Trauma (basal skull fracture) results in high-flow fistulas
• Degenerative vascular process in patients with hypertension and atherosclerosis results in a low-flow fistula.
History
• Abrupt onset of proptosis, chemosis, arterialization of the conjunctival vessels in one eye.
• This occurs in a high-flow AVM.
• High-flow AVMs will have more severe symptoms but often have the history of head trauma.
• Low-flow AVMs are in older patients, are slower in onset, and the symptoms are less dramatic.
Examination
• Proptosis, chemosis, dysmotility, arterialization of the conjunctival vessels (corkscrew pattern) (Fig. 14-8A, B), and elevated intraocular pressure are seen in AVMs.
• In high-flow states, the retinal vessels are affected with venous congestion.
Imaging
• CT scan and MRI show an enlarged superior ophthalmic vein and there may be enlargement of the extraocular muscles (Fig. 14-8D and E).
• Orbital Doppler shows reversal of flow in the superior ophthalmic vein and is diagnostic of an AVM (Fig. 14-8C).
Differential Diagnosis
• Orbital pseudotumor
• Orbital cellulitis
• Thyroid-related ophthalmopathy
• Chronic conjunctivitis
Treatment
• Low-flow AVMs will often resolve spontaneously.
• The signs may worsen as the fistula closes off. High-flow lesions often require attempted selective embolization to close the fistula.
• This may also be needed in low-flow lesions that result in uncontrolled glaucoma, diplopia, or vascular occlusion.
Prognosis
• Variable. Many low-flow AVMs will close on their own. Treatment for AVMs is successful but does have a risk of visual loss.
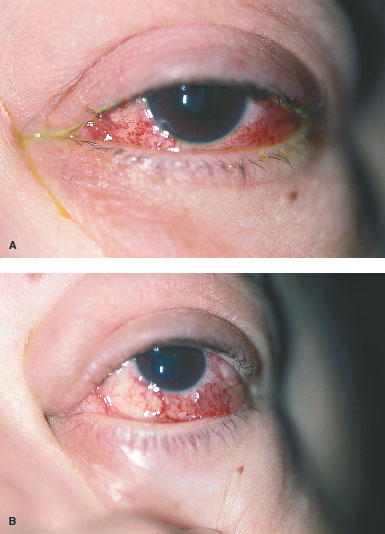
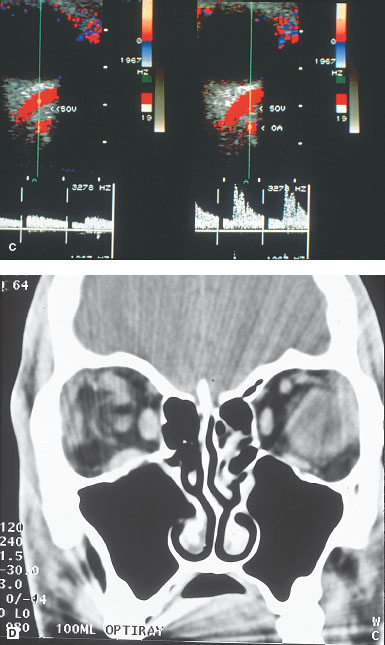
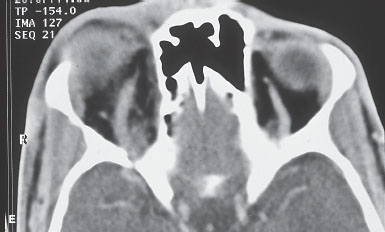
FIGURE 14-8. Arteriovenous malformation. A and B.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


