CHAPTER 13
Food Allergy
Up to this point, this book has been concerned primarily with the diagnosis and treatment of inhalant allergy (sensitivity to substances inhaled). But there are other types of allergy: ingestant allergy which is sensitivity to substances ingested, and contact allergy, which is sensitivity to items that contact the skin or mucous membranes. These terms are bandied about so freely by the allergist that it is easy to forget that the patient frequently does not understand the distinction and hesitates to ask for fear of appearing stupid. Most aspiring allergists start their program by treating only inhalant allergy, and in many cases only allergic rhinitis, as lower respiratory tract disease tends to involve additional problems other than allergy. Starting with the management of inhalant allergic rhinitis is a realistic approach. The success quotient for those treating this condition is high, and a series of successes both boosts confidence and helps in establishing a reputation for competence. It will not be too long, however, before a situation arises that simply does not fall within the parameters of allergic rhinitis caused by inhalants. It may be that all the symptoms of allergic rhinitis are present, but there appears to be no seasonal or exposure pattern. Alternatively, all the symptoms of allergic rhinitis are present but all the test results are negative. There are several possible explanations for this situation (discussed in Chapter 12), but one possible condition that should immediately be considered is food sensitivity.
For the rhinitis sufferer with negative inhalant test findings, the usual reaction to suggesting the possibility of food sensitivity is, “I’m not allergic to any foods!” This may be translated as, “I don’t have any gastrointestinal symptoms.” It may take a bit of convincing before the patient accepts the fact that an offender may produce symptoms in body locations other than that by which it entered the body. One explanation that is frequently accepted by patients is to remind them that the antihistamine-decongestant tablet taken to relieve nasal symptoms was ingested, not inserted into the nose, yet the result did not surprise the patient at all. In other words, the route of entry frequently has little to do with the response.
THE CONFUSING REALM OF FOOD SENSITIVITY
Some physicians have settled for the degree of success possible in treating only inhalant allergy, electing not to pursue the management of more difficult cases. Although food allergy patients can be straightforward, some are complex or very symptomatic patients, frequently with asthma, skin disease, or chronic rhinosinusitis. Food allergy is also often part of the problem in the “many” syndrome patient (many doctors, many symptoms, many treatments, and many failures). For those to whom less than the best possible result is unacceptable, the field of food sensitivity is a fascinating, sometimes frustrating, and often rewarding one. There is a great sense of accomplishment when a patient, previously written off as hopeless or psychosomatic by other practitioners, responds to simple dietary control measures.
Achieving control of food-provoked symptoms requires an understanding of the many factors involved in food sensitivity. Allergists are justifiably proud of their accomplishments during the past several decades in objectively identifying inhalant allergens and providing predictable results in care. To many physicians, and a majority of third-party payers, it seems incomprehensible that a simple, reliable test for food sensitivity is not even on the horizon. Were such a test available, it would be a fairly simple task to have the patient remove the offenders from the diet, thereby controlling the symptoms. Why does such a test not exist? Careful consideration of several points is necessary to understand the magnitude of the problem.
Definition
The first source of confusion is that there is not even a universally accepted definition of food allergy.1 To the layperson, and even to the nonallergist physician, food allergy is usually defined as an adverse reaction to a food, in a specific patient, in the absence of the same reaction in other people who consume that food. To the allergist, this definition is too simple. The definition of food allergy depends on whether an immune mechanism produces the reaction, and even this definition is not uniform throughout the medical world.
Food sensitivity is known to involve all parts of the immune system, as well as mechanisms entirely outside the immune system. Among most general allergists in the United States, allergy (of whatever type) is defined as an adverse reaction mediated by immunoglobulin E (IgE). This is a Gell and Coombs type I reaction. A type I, anaphylactic, reaction is the only form of allergy easily capable of producing fatal results. These reactions represent only a small percentage of adverse reactions to food, but because of their sudden and severe nature, they have a high degree of visibility. Although type I reactions are easily identified by skin or in vitro testing, such tests are rarely needed, for these reactions are prompt, frequently violent episodes, that are usually quite obvious in their clinical pattern of cause and effect. Because of lifelong persistence, IgE-mediated food allergies are often referred to as fixed’food allergies. Although the patient’s sensitivity to a provoking food may diminish if avoidance is practiced for a period of years, it probably is never completely lost, and is easily reinvigorated by future exposure.
Fixed, type I food sensitivity has been estimated to represent between 5 and 20% of all food hypersensitivity. This broad range of estimates is a result of limitations that exist in recognizing other types of food hypersensitivity. In fact, the recognition of mechanisms of food allergy other than via IgE has been very slow to evolve. Breneman wrote, “For 30 years we have had a fixation on IgE as the answer to all food allergy questions. Why? Because we had two good tests for it (IgE RAST and skin tests).” Yet, “IgE explains only a small part of food allergy. Involvement of the entire immune system is evident if the more prevalent delayed-type food allergy is to be explained.”2
In the United States, allergic food reactions other than the anaphylactic type are usually designated hypersensitivity, and reactions outside the immune system are simply adverse reactions. To complicate matters further, in Europe, adverse reactions involving any or all Gell and Coombs categories are usually considered allergy, whereas specific adverse reactions outside the immune system are considered hypersensitivity. These definitions are by no means universally adhered to, however, and rarely does a contributor to the literature bother to define the terms being used when writing an article. This further compounds the difficulty of interpreting the significance of any study. In 1994, at a major pediatric conference, three articles were presented lamenting the lack of uniformity in defining food sensitivity and proposing carefully thought out definition formats. Unfortunately, no two of the articles were in agreement in their choice of terminology.3 Thus, it is not difficult to see why confusion reigns concerning the subject of food allergy, when the parameters of the problem have not even been adequately and consistently defined.
Because this book is designed for clinicians, and especially for physicians newly adding allergy to their practice, this chapter equates the terms for adverse reactions to foods: allergy, sensitivity, and hypersensitivity. These terms are taken to mean an abnormal reaction to a food, observed in one person, but not seen in the general population. The bottom line, after all, is relieving the patient’s symptoms. As will be evident in the portion on treating food reactions, this involves dietary manipulation, which serves to treat both immunologic and nonimmunologic reactions alike.
BIOLOGIC PATHWAYS OF FOOD REACTIONS
Immunologic Reactions
Food may act on the body through any of the four immunologic mechanisms defined by Gell and Coombs (which are explained in detail in Chapter 2).4 In addition to the type I reaction already described, types II, III, and IV have been demonstrated to occur in food allergy In a study of 54 infants with eczema and positive double-blind cow’s milk challenge results, and by comparing multiple simultaneous methods of testing, Isolauri’s group5 found that only 15% were type I, whereas 26% were type IV, 35% were either type II or type III, and 24% were of mixed types. There have been several other recent reports demonstrating similar high prevalence of non-IgE-mediated food allergies.6–11 Type III reactions have been theorized to be the most common immune mechanism in food allergy, though to date few studies have been able to give precise values to the degree to which each Gell and Coombs type occurs. Type IV (cell-mediated) reactions may also be fairly common in food allergy, but the delay of hours to days in appearance of symptoms makes clinical correlation extremely difficult. For clinical use, accurately identifying the type of reaction is not practical, because it can only be done by subjecting patients to multiple forms of testing for the same foods. The underlying mechanism of the immunologic reactions is shown in Table 13-1.
FIXED AND CYCLIC CLINICAL FOOD ALLERGY CATEGORIES
Although each type of immune reaction may involve a different route by which a food may produce an allergic reaction in a patient, these reactions have been clinically divided into fixed and cyclic types. Fixed food reactions are defined as those that always occur when the offending food is ingested in any quantity (even minute amounts). These reactions are often rapid in onset and may be severe. Some cases of delayed symptom onset, producing chronic, rather than acute, illness, have also been ascribed to IgE-mediated reactions. These late-onset type I reactions may involve a prominent late-phase reaction, such as is seen in asthma, but are still incompletely understood. As previously noted, all IgE-mediated sensitivity is normally sustained throughout life, although it may weaken somewhat after several years if there has been no exposure. Fixed reactions are now considered synonymous with IgE-mediated type I reactions.
Gell and Coombs type | Mediators |
|---|---|
1 (anaphylactic) | IgE |
II (cytotoxic) | IgG, IgM, complement |
III (immune complex) | IgG, complement |
IV (cellular) | Sensitized T lymphocytes |
Fixed reactions are usually immediate, whereas cyclic food reactions may be immediate or delayed, with the delay ranging from a fraction of an hour to as much as 1 to 2 days or longer. These reactions, unlike fixed food reactions, are dose and frequency related. This means that the food may be eaten occasionally without the patient’s sustaining a reaction, but if the food is eaten regularly at every meal, or even every day or so, a reaction will occur. The more frequently the food is eaten, the more rapid and pronounced the response may be expected to be. Similarly, a small quantity of an offending food may be eaten without the patient’s suffering any ill effects, but if a large quantity of the food is consumed, the symptoms will appear. Cyclic food sensitivity is mediated by any component of the immune system other than that involved in the type I Gell and Coombs mechanism.
It is easy to see why identification of a cyclic food allergy can be difficult for the physician, and virtually impossible for the layperson. In the instance of a delayed reaction, it might be necessary to recall every food eaten during several days and make the relevant connection to the reaction. For the average individual, this is not a practical approach. Fortunately, other methods exist for identifying offenders, and these are discussed later.
Masking
An interesting, and very common, clinical aspect of cyclic food sensitivity is the development of masking. Many patients with cyclic food allergies develop a tendency to eat the offending food at every meal, and frequently between meals. Like drug addicts, they “crave” the food because a regular dose of the offending food temporarily relieves some of their symptoms. This temporary improvement is offset by the fact that, overall, the patient’s condition is worsened by the offending food, and if the food is withdrawn from the patient’s diet, a considerable improvement ensues. This does eventually occur, but in the early stages of withdrawal, the patient frequently complains of an increase in symptoms and must be encouraged to persevere until relief is noted (generally after 4 to 7 days). A food can be strongly suspected of causing cyclic allergy with masking when the patient s immediate reaction to a discussion of food sensitivity is, “Don’t take away my chocolate!” (or whatever food it may be). Masking is also suspect when patients always eat just before sleep, or habitually awaken for a snack.
Nonimmunologic Reactions
In addition to provoking the immunologic reactions already described, food is able to affect the body through a variety of pathways not involving the immune system. These reactions may be all but impossible to distinguish, on the basis of symptoms alone, from immunologic reactions. Although many chemical mediators may be involved in various adverse food reactions, the most frequent mediator is histamine, which is contained in mast cells throughout the body. Histamine can be released by both immunologic and nonimmunologic reactions. For example, when certain foods (e.g., strawberries and tomatoes) are ingested, they induce the release of histamine without involving the immune system. Other foods, such as aged cheese or spoiled fish, contain preformed histamine that is released on ingestion. Table 13-2 lists some of the foods that may induce the release of histamine and related substances on ingestion. Thus food, unlike inhalant allergens, is capable of affecting the body through a wide variety of mechanisms, many of which produce very similar reactions.
In addition to the histamine-triggered induction of adverse reactions to foods described previously, certain enzyme deficiencies may make foods incompletely digestible, and food-borne toxins may cause gastrointestinal injury, resulting in symptoms that may be virtually indistinguishable from those of food allergy. Lactase deficiency is a well-known example. These are also noted in Table 13-2.12
1. | Food intolerance: abnormal, nonimmunologic reaction to ingested food or additive Example: lactose intolerance |
2. | Food poisoning: reaction caused by endotoxins or exotoxins within the food, or released by contaminating microorganisms or parasites Example: Escherichia coli gastroenteritis |
3. | Pharmacologic food reaction: adverse reaction to pharmacologic effects of chemicals found in food or additives, or stimulated by them, that is not immunologic in nature Examples: (a) direct effect of caffeine (stimulation), red wine (tyramine headache), food additives (monosodium glutamate headache); (b) release of histamine from strawberries, tomatoes, egg whites, spoiled tuna, aged cheese |
COMPLICATING FACTORS
Cumulative Reactions and Cross-Reactivity
Like inhalants, ingestants (foods) contain a large variety of biologic antigens, any number of which may be sensitizing. Different foods may contain several such antigens in common. As with inhalants, the number of such antigens shared by different foods determines the degree to which these foods immunologically cross-react. In the case of botanical foods (i.e., grains, fruits, vegetables, and foods prepared from them) cross-reactivity is common, although frequently unrecognized by either patient or physician. For those without extensive botanical knowledge, specific references may be helpful. Appendix 1 contains a cross-reactivity list providing information that is both useful and interesting. For example, how many laypersons would recognize potato and eggplant as close relatives? This cross-reactivity among foods may easily result in an accumulation of similar antigens in the system from several different foods to which the patient is sensitive. The resultant unrecognized increase in the total load of allergens affects the pattern of cyclic allergy, which is affected by both dose and frequency of ingestion. Patients may think that they are eating only a limited amount of a particular food, or eating it at infrequent intervals, but if they are in fact eating other cross-reacting foods of the same food family, the result may be the same as if large quantities of the primary offending food are eaten regularly. It is the total amount of the reactive allergen in the system at one time, and/or the frequency with which the body is exposed to the allergen, that determines the intensity of symptoms produced by cyclic food allergy. To determine the eating habits of the patient, not only must individual consumed foods be identified, but cross-reacting foods must also be considered, and the total quantity of each cross-reacting food family group should be estimated.
In the case of nonbotanical foods (meat from mammals, fish, birds, and other animals), studies of cross-reactivity are more limited. In this food group, IgE-mediated food allergies, mainly those caused by crustaceans and mollusks, are well known. As previously noted, IgE-mediated food sensitivity is a relative rarity and usually presents no difficulty in diagnosis, as reactions are usually prompt and noticeable. Cyclic food responses are more subtle, and hence more difficult to recognize. The non-IgE-mediated antigenic reactions involving meats have not been extensively studied, and hence knowledge of cross-reactivity within this group is limited. When considering cross-reactivity in the nonbotanical food group, it is largely necessary to use clinical ingestion trials, investigating only nonanaphylactic foods that are being eaten.
A taxonomic classification of botanical foods correlates with allergenic cross-reactivity to a considerable degree of accuracy. The closer the taxonomic relationship of an organism is to another, the greater the number of similar antigens they share. Food plants cross-react extensively between the species within a single genus, to a lesser extent with closely related genera within a family, and to a still lesser extent with related families within an order. It is a reasonable assumption that foods derived from animals do the same. The more distant the evolutionary time interval separating the development of two families from the primordial line, the fewer similar antigens are likely to be encountered. There are exceptions for strongly conserved allergens, however, which may rarely cause even different classes or phyla to cross-react. Clinical experience supports this taxonomic view, although complete immunologic confirmation would require more ability to characterize non-IgE-mediated food reactions than is currently available.
The working hypothesis for estimating cross-reactivity in nonbotanical foods is the same as for plants: that antigens of animals of the same genus will probably cross-react to a significant degree, whereas antigens of animals of different genera are less likely to do so. For example, consider chicken and turkey. Many commercial charts of cross-reactivity list as a group simply “birds.” This is not a uniform group, any more than “seafood” is a single entity. Chicken (Gallus domesticus) is the oldest and most widely distributed form of domestic meat known. All chickens are believed to have been derived from the red jungle fowl of India, and despite extensive manipulation of breeding through the millennia, it probably maintains most of the same allergens originally present. Turkey (Meleagris gallopavo), on the other hand, is a bird native to the Western Hemisphere, domesticated only in the last few centuries. Even though these birds are in related genera, our clinical knowledge indicates that although cross-reactions do occasionally occur, there is often little cross-reactivity between chicken and turkey. A similar situation exists between beef and bison. The cow (Bos domesticus) is thought to have evolved from the extinct European auroch. The American bison, or buffalo (Bison bison), on the other hand, is a New World creature. Although they are closely related genera, and capable of interbreeding, bison meat has only rarely been found to cross-react with beef. More distantly related animals, for example, ostrich and chicken, or cattle and deer, are even less likely to cross-react.
Not only multiple genera, but also multiple phyla exist in the sea, an edible fauna even more diverse than on the land. Many laypersons have come to believe that they are sensitive to “seafood.” The person who suspects they have “shellfish” allergy is discussing two very distantly related phyla, Crustacea and Mollusca. Although contamination is always a possibility, as when shrimp larvae become lodged in an oyster s filtration system, true cross-reactivity between crustaceans and mollusks is rarely seen, and is not a usual problem. Cross-reactions can also sometimes occur between cephalopod mollusks (octopus; squid) and oceanic fishes, because of the fact that both are parasitized by an allergenic roundworm, Anasakis, whose antigens, unlike the worms, are not destroyed by cooking. Among both freshwater and oceanic fishes, cross-reactions among the over 40 different edible fish families are normally not observed. The exceptions, which occur in a minority of fish allergy cases, are caused by sensitization to parvalbumin, a highly conserved protein found in most, if not all, fish.
Appendix 5 lists some of the common staple animal foods in the typical American diet. It must be stressed that this represents only a starting point from which to explore cross-reactivity However, it is a reasonable approach, as opposed to the “substitute” foods suggested in some of the commercial literature, so that persons allergic to common meats do not have to try locating whale or hippopotamus! When cross-reactivity between meats other than those listed is to be considered, a reasonable approach is to use the same principle already applied to the foods previously described. One can check the scientific name of the animal in question in an encyclopedia or on the Internet, at http://animaldiversity.ummz.umich.edu/index.html If the genus of the two foods being compared is the same, there is probably significant cross-reactivity. If the genera are different, there is less chance that they cross-react. It must be borne in mind that this is simply a guide. There may at times be some cross-reactivity between even very distantly related organisms, and people are unique in their allergic sensitivity. However, consideration of cross-reactivity based on the scientific taxonomy of a food provides a very useful starting point.
Concomitant Food Reactions
In addition to cross-reactivity between various types of botanical food, cross-reactivity frequently exists between inhaled pollens and ingested foods of the same botanical family. Thus, the ingestion by a patient with active inhalant allergy of a cross-reacting food may produce a greater reaction than expected. This is called a concomitant food reaction. Such clinically observed cross-reactivities between inhalants and foods have usually been confirmed by radioallergosorbent test (RAST) inhibition studies (Fig. 13-1), which use a precise in vitro competition technique for confirming the presence of cross-reacting antigens.
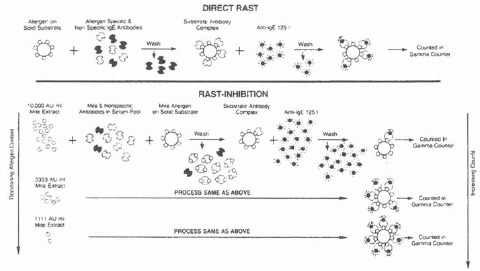
Figure 13-1 Radioallergosorbent test (RAST) inhibition is performed as a modification of the RAST to determine cross-reactivity between various immunoglobulin E (IgEJ-mediated allergens, whether inhalant, food, or both. First, one of the antigens to be tested is serially diluted. The antigen dilutions are then added in measured amounts to a patient s serum known to contain specific IgE for the other antigen to be tested. After this is done, a RAST is run for the second antigen. If the two antigens cross-react, some of the specific IgE will be bound before the serum is exposed to the RAST disk. This makes less unbound IgE available to bind to the RAST disk. The RAST reading, therefore, will be lower than that seen without exposure to the first antigen. The degree to which the reading drops with each serial dilution is a measure of the cross-reactivity between the two antigens. (With permission from Mason WW, Ward WA. Otolaryngolic Clinics of North America. Philadelphia: WB Saunders; 1992:108.)
The classic example of inhalant and food cross-reactivity is that between grasses and cereal grains (which are, in reality, grasses). The phenomenon has also been demonstrated between such apparently diverse items as apple (the fruit) and birch (the pollen), as well as between ragweed and members of the gourd family (watermelon, cantaloupe). A more extensive list of cross-reacting inhalants and foods is found in Appendix 1. The clinical significance of concomitant reactions is that all allergens, although they enter the body by different routes, contribute to the total allergic load. For example, a person mildly sensitive to both apple and birch pollen might have no reaction on eating an apple in the fall, but when birch trees are pollinating in spring, eating the same amount of apple might precipitate a severe reaction. This type of reaction is one more complexity to confuse and confound the unwary allergist and the allergic patient.
Speed of Digestion
Digestive action does not always proceed at the same rate. As a result, foods transiting the digestive tract are retained, in an antigenically intact form, for variable times within the gut. Even though a food is eaten at the same time each day, if digestion and absorption (for one reason or another) are proceeding at different speeds on different days, food antigens may accumulate in the digestive tract at a given time on one day, and be largely absent at that time on another. Food is thus digested and absorbed into the circulation in a less predictable manner than is generally imagined. This affects food ingestion diary analyses by making less regular and predictable any cause-and-effect relationships between each food eaten and the symptoms produced. It also complicates diagnosis and treatment by dietary rotation, a technique discussed later (see Treatment of Food Allergy).
Antigen Alteration
As if the previous problems were not enough, simply identifying a basic food to which a patient is allergic does not necessarily clarify all the possible ramifications of the situation. With inhalants, the offending substance is delivered to the nasal mucosa in its natural, unaltered state. Although some foods are usually eaten raw, more commonly foods are processed in some manner before being eaten. This may be by cooking, fermenting, marinating, or any number of methods designed to prolong the storage or enhance the palatability of the food. All such procedures are capable of altering the antigens present in the food, and the degree and pattern of such alteration are not predictable. Although some of the antigens of the basic food remain, others are changed or destroyed. In addition, new antigens may be created during processing. For example, a patient sensitive to cow’s milk would be expected to also show sensitivity when eating cheese, but the sensitivity might be less than that displayed when whole cow’s milk is ingested. Also, other allergens may have been created by alteration of the antigens of cow’s milk during processing into cheese, so that some patients may react to cheese, but not to milk. This alteration of food antigens by preparation is one of the factors that has limited the effectiveness of testing for food allergies using “pure” food material prepared by reference laboratories. The material used in testing does not necessarily represent the material to which the patient is actually exposed.
Additives
In addition to the antigen alteration produced by the processing of foods, most foods, even after processing, have various additives applied prior to being eaten, either by the person preparing the food, or by the person consuming the food. This range of additives, limited only by the tastes of the persons involved, may range from salt and pepper to spices, flavor enhancers (such as monosodium glutamate), lemon, garlic, and a host of other materials. Each carries its own antigens, which may have their own individual effects, or some of the antigens in the additive may be the same as those of the food to which they have been added. In this case, there will be a cumulative effect comparable with that of eating two or more foods in the same family.
A great deal of material has appeared in the literature during the past several decades about the effect of xenobiotics, the “invisible” chemicals present in foods and water. These include pesticides, antibiotics, hormones, preservatives, coloring agents, and many other categories of chemicals. Although these substances undoubtedly affect some persons, there is much disagreement as to the degree and nature of their effects. Realistically, attempting to include such substances in an evaluation of food allergy is beyond the scope of the developing allergist, who will encounter enough difficulty in identifying major offenders and trying to provide a significant degree of control by limiting those offenders. A reasonable approach to the problem of intrinsic chemicals is to advise the patient that if, after as much as possible has been done to control food allergy, problems persist when food or water from a particular source is consumed, that source should be changed. For the patient who is truly this sensitive, certified organic food sources with no additives are often available, and people can also be encouraged to grow some of their own food, and to use purified water. Patients who continue to have major symptoms as a result of possible chemical exposures should be referred to senior physicians who are knowledgeable about chemical illness.
Multiplicity of Target Organs
It has already been stressed that the portal of entry for an allergen may have little effect on the site or type of eventual reaction. Although it is true that inhalant allergens primarily affect the respiratory tree, even this is not always the case. Food allergens show no such limitations in their range of action. Before the allergic reaction can occur, the foods must be digested, and the digested antigens absorbed into the circulation and carried to the target organ. This much is not difficult to understand, but why allergens circulating throughout the body should affect certain organs and not others is still not understood. Virtually any organ or organ system can serve as a target organ, and the organ is not specific to the food. In other words, cow’s milk may produce a rash in one person and asthma in another. The target organ in the first person is the skin, and in the second it is the lungs. The reaction is specific to the patient, and if milk causes asthma in one patient, milk will normally continue to cause asthma in the same patient. It will not switch to causing a rash. Of course, there may be more than one target organ from the beginning. Milk, for example, might cause both asthma and diarrhea as soon as the patient becomes sensitized. If this is the case, the symptom pattern may fluctuate in severity over time, varying with the amount of milk consumed and the interval between exposures, but rarely will the pattern change. Therefore, new symptoms developing in another target organ usually indicate sensitivity to a new, and different food.
Virtually any organ system in the body may be a target organ for adverse reactions to food. The symptoms depend on the nature of the target organ, not on the type of food, and are not greatly influenced by the type of immunologic or nonimmunologic mechanism causing the reaction. As described in Chapter 2, and reiterated in the portion of this chapter on the nature of food reactions, most food reactions involve the release of histamine, or other similar mediators, into the tissues of the target organ, which in turn, produce tissue edema and inflammation. It can be quite difficult to determine the specific mechanism involved, except for the clinical difference between fixed and cyclic reactions. If the target organ is the external carotid artery complex, for example, a migraine headache will result. If the target organ is the intestinal tract, cramping and diarrhea may be expected. The reactions within each tissue at a cellular level are very similar, but each organ responds differently to inflammatory injury.
The “Leaky Gut Syndrome”
Yet another factor may even further complicate the picture of food allergy. Some patients report being “allergic to everything.” However, clinical studies on food allergy, worldwide, have been in agreement that rarely are patients primarily allergic to more than five or six foods. These “universally allergic” patients, however, appear to react adversely to an immense range of foods, typically to almost every food that is tested. Frequently, such reactions have not been a lifelong problem but have developed within a short period of time. This apparent contradiction in patterns, which is not uncommon, can be easily explained.
The mature intestinal tract, functioning properly, is a sophisticated immunologic filter. Food substances are not absorbed from the intestine into the circulation until digestion has broken them down into such small macromolecules that the immune system tends to consider them as building blocks rather than potential offenders. The intestinal tract, however, is easily shocked, and when such shocks occur, the gut wall becomes much more permeable and absorbs larger macromolecules of food, which then produce sensitization, and true allergic reactions. Many factors can shock the intestinal tract to this degree. They include infection or parasites, immaturity, and immunologic insults, including food allergy.12
Infection is a complex subject, but it is necessary only that the allergist realize that infection can give rise to increased gut permeability. In cases in which almost all food allergy tests are positive, some evaluation to identify fungal, bacterial, or parasitic causes should be considered, especially if the history suggests potential reasons for one of these to develop.
The infant has not yet developed a mature intestinal tract, and as a result, varying degrees of leakage of macromolecules are common. This is the reason why a small child frequently strongly manifests allergic clinical problems, although skin testing and/or in vitro tests indicate little or no response. Skin testing and/or in vitro testing is reliable for IgE-mediated allergy, but major amounts of IgE usually have not developed in infants, even if they have the genetic makeup to allow such an abnormality to appear. Prolonged or frequent exposure to allergens is required for significant amounts of specific IgE to develop. As stated elsewhere, it is often of little value to test a child for pollen allergy before the age of 5 or 6 years, and even sensitivity to perennial allergens (e.g., dust, mold, and pet epidermals) is usually minimal before the age of 2 or 3 years. On the other hand, the intestinal tract at birth, and for several months thereafter, is “porous.” The allergic child with gut immaturity may be expected to demonstrate a wide range of food allergy symptoms, including nasal and eustachian tube congestion, in addition to eczema and gastrointestinal complaints. It has been frequently observed that the vast majority of recurrent otitis media cases, appearing before age 1, can be controlled simply by eliminating cow’s milk from the diet. For the child with major allergy symptoms of any type, analyzing the diet and replacing the major staples (in the infant, usually the formula) with another basic food type frequently reduces or eliminates the problem. It is reassuring to the parents to note that most such early food allergy problems eventually resolve as the intestinal tract matures, the child is treated with a rotation diet, and permanent damage to the affected target organ is prevented by appropriate medical and surgical therapy.
Most pertinent to the present discussion is the effect of true food allergy on the gut. When the gut is exposed to true allergenic offenders, the organ may become shocked, a state of intestinal local anaphylaxis. The allergic inflammation of the gut wall creates a vicious cycle of abnormal permeability leading to more inflammation, and to even further enhanced permeability to allergens, resulting in the eventual development of a multitude of food sensitivities. When the initial offenders are identified and removed from the diet, the gut recovers, and the patient then becomes able to tolerate many or all of the other foods previously considered by the patient to be allergens. To some degree, this allergic leaky gut syndrome is probably triggered by an increase in the total ingested portion of allergic load beyond some critical limit. It probably is easier to exceed this critical limit if other factors that tend to cause gut permeability are also present. Therefore, a good history should always be obtained to seek out such factors (such as extensive antibiotic use that could lead to intestinal yeast overgrowth).
Summary of the Problem of Food Reactions
A person with multiple symptoms, especially if the symptoms are not always manifested concurrently, may be suspected of being sensitive to several foods, each causing different symptoms through involvement of different target organs. Although both specific immunologic and nonimmunologic pathways are involved in food hypersensitivity, it is also true that a single food may utilize more than one pathway, and one patient may have more than one type of reaction under way at any one time. Allergenic foods may shock the gut. Foods may act in combination with each other or with inhalants. All these factors explain the virtual impossibility of developing a simple test for food sensitivity. In analyzing the results of the multiple routes and multiple possible reactions, it is necessary to look at the bottom line; determine the specific reactions that have occurred, attempt to identify the cause-and-effect relationship (not an easy task), and maintain a high degree of suspicion for food reactions. Many patients dismissed as hypochondriacs have been cleared of many or all of their symptoms and returned to productivity by successful treatment of food sensitivities. In similar fashion, other patients, with intractable, severe allergies, not responding well to drugs and immunotherapy, can be improved or cleared by appropriate treatment of their food allergies.
NURSE’S NOTE
There are many types of food reactions. Immediate (Gel I and Coombs type l IgE-mediated) food reactions always carry the potential for anaphylaxis, and foods known to cause them should be avoided indefinitely by the patient. Cyclic food reactions, generally Gel I and Coombs type III, may be treated successfully by dietary manipulation. This requires careful detective work by the patient and members of the allergy team, however.
The allergy nurse or assistant is often the person to whom the allergy patient turns for answers, and so this person must be knowledgeable in the area of food families to aid the patient with suspected food allergy. Lists of “hidden sources” of common allergenic foods are available from many antigen suppliers. Examples are provided in Appendix 4.
When patients are asked to complete a diet diary, it is important that they realize that they wm not be judged on the results. Otherwise, what is often returned is what patients think they should be eating, not what they actually consume, if a dietitian is not available in the allergy office, the allergy nurse or assistant is often asked for help in planning a diet that provides adequate nutrients while avoiding offending foods. For example, the patient on a milk-free diet must consider calcium supplementation, Fortunately, it is often possible to obtain this information from commercial sources and books on food allergy.



