FIGURE 12.1 B-scan probe positions. Transverse position (top-left) with probe orientation as indicated by the white mark is parallel to the limbus, longitudinal position (top-right) with the probe perpendicular to the limbus, axial position with the probe centered on the cornea. (Reprinted with permission from Byrne SF, Green R. Ultrasound of the eye and orbit, 2nd ed. New Delhi, India: Jaypee Brothers Medical Publishers Pvt. Ltd., 2010.)
Specific Indications of Ultrasonography in Children and Infants
Echography can be very helpful in a number of pediatric vitreoretinal conditions, including cases of opaque media from corneal or lenticular opacities, anterior chamber or vitreous hemorrhage, and vitreous opacities; detection of retinal detachment; measurement of visible fundus lesions such as retinoblastoma or other tumors; identification of intraocular foreign bodies; and biometry in congenital glaucoma, anisometropic amblyopia, and unilateral persistent fetal vasculature (PFV) in which differences between eyes can be determined.
Many of these indications cause an appearance of a white pupil described as leukocoria and is the most common indication for ophthalmic ultrasonography in the pediatric population (2). The most serious cause of leukocoria is retinoblastoma, which is potentially lifethreatening if not diagnosed and treated.
Retinoblastoma
Retinoblastoma should always be suspected in a child with an intraocular mass lesion. The majority of these tumors occur in children under the age of 3, but rare cases occur even in adults. Retinoblastomas can occur in an endophytic (growth into the vitreous) or an exophytic form (growth under the retina), but some tumors display elements of both growth patterns. A majority (90% to 95%) of these lesions have calcium deposits ranging from those seen only microscopically to those easily detectable on imaging studies. Ultrasound is very sensitive in detecting calcium (Fig. 12.2), whereas magnetic resonance imaging (MRI) is not. Fine calcium deposits can be missed on computed tomography (CT). A less common form of retinoblastoma is the infiltrating type that grows within the retina and presents as nonspecific retinal thickening (Fig. 12.3). Diffuse infiltrating retinoblastoma occurs often in older children and does not contain calcium (see also Chapter 26).
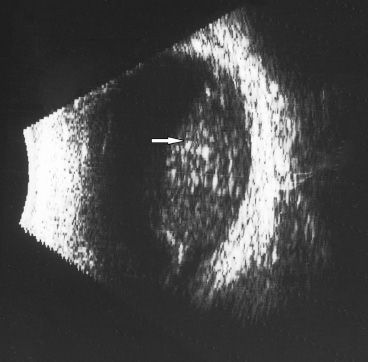
FIGURE 12.2 Retinoblastoma with diffuse fine calcium deposits (arrow). As the gain on the B-scan is reduced, the high reflectivity of the calcium will remain bright.
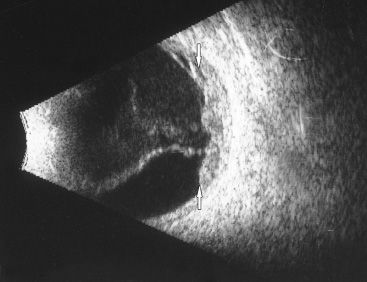
FIGURE 12.3 Diffuse retinoblastoma (arrows). This lesion is not seen on ultrasound as a discrete tumor mass, but is more irregular and extends underneath the retina. No calcium is detected.
Most retinoblastomas are found in the posterior segment of the eye, but can rarely be found in the peripheral retina. These can mimic a chronic inflammatory process and be confused with intermediate uveitis or pars planitis (Fig. 12.4). The anterior location is best visualized using immersion ultrasound. Higher-resolution probes (20 MHz to 50 MHz) show greater detail than a standard 10-MHz probe, but the 10-MHz probe permits the display of the entire extent of the tumor and its relationship to adjacent structures.
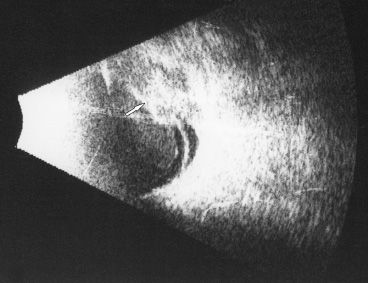
FIGURE 12.4 Pars planitis. The B-scan probe on the temporal globe is angled very anteriorly to visualize this area of the pars plana (arrow).
When retinoblastomas spread outside the globe, it is generally by invasion of the optic nerve. Echography is usually unhelpful in this situation because microscopic invasion of the optic nerve cannot be detected even though the retrobulbar optic nerve can be visualized by the B-scan and measured very accurately by the A-scan. MRI can more reliably detect invasion of the optic nerve, but false-negative and false-positive results have been reported (3). Usually both modalities are recommended for suspected optic nerve invasion including the detection of trilateral retinoblastoma.
Echography is a very useful in the evaluation of retinoblastoma. Ninety-five percent of these tumors have characteristic ultrasonographic findings, but 5% are atypical and create clinical challenges in this potentially fatal condition. Still, in many cases, ultrasonography is combined with CT and MRI imaging.
In a series of 227 cases presenting with leukocoria that clinically simulated retinoblastoma, PFV (see Chapters 3 and 53) was most commonly misdiagnosed as retinoblastoma (4).
PFV can appear in a number of forms. Ultrasonography is able to distinguish anterior PFV from posterior PFV, although many patients can have a combination of these two. PFV is unilateral in over 90% of cases, but when bilateral carries a poorer visual prognosis. Axial length is generally shorter in eyes with PFV than in the normal contralateral eye by 0.5 to 1.0 mm, and this can be a helpful differential finding as measured by A-scan.
Findings in the posterior variant of PFV include vitreous membranes, a stalk (remnant of Cloquet canal) extending from the optic nerve to the posterior lens capsule, optic nerve dysplasia, and retinal folds. Imaging of the stalk by echography can be difficult and may require different B-scan probe positions at high gain to demonstrate it. A transverse view with the probe held parallel to the limbus will cut across the stalk making it appear as a small echolucency. A longitudinal position with the probe perpendicular to the limbus demonstrates the stalk as an elongated echodensity as the sound beam is reflected along its length (Fig. 12.5). A longitudinal cut inferonasally often provides an easy and useful image particularly in the infant eye. Sometimes vitreous traction on the retina can cause a focal or total retinal detachment.
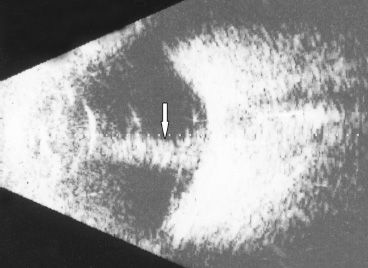
FIGURE 12.5 PFV with vitreous stalk (arrow). Vascularity was detected as rapid spontaneous flickering movements inside the band during the examination.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


