
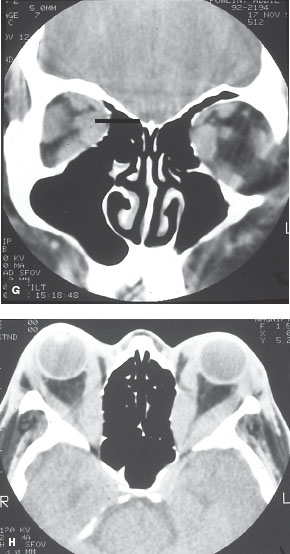

FIGURE 12-1. Thyroid-related ophthalmopathy. A. A patient with very early thyroid-related ophthalmopathy with slight lid retraction on the left. B. In down gaze, there is eyelid lag. C. A 20-year-old patient with severe proptosis, eyelid retraction, and corneal exposure. Thyroid-related ophthalmopathy. D–F. A 45-year-old patient with progressive swelling of the eyes with double vision and recent decreased vision. There is proptosis, chemosis, and limitation of motility. Vision was 20/80 from optic nerve compression. Thyroid-related ophthalmopathy. G and H. CT scans show enlargement of all rectus muscles with crowding at the orbital apex. The patient required an orbital decompression and her vision returned to normal. Thyroid-related ophthalmopathy. I. A patient with severe thyroid-related ophthalmopathy. J. After 3 years and multiple surgeries, there is significant improvement.
IDIOPATHIC ORBITAL INFLAMMATION (ORBITAL PSEUDOTUMOR)
Epidemiology and Etiology
• Age: Children and adults
• Gender: Equal incidence in males and females
• Etiology: This inflammatory process is by definition unrelated to any systemic abnormality and the cause remains unknown.
History
• Acute onset of orbital pain often associated with proptosis, erythema, swelling, and restricted eye movements.
• The symptoms depend on the exact location of the process but pain is common to all presentations.
• Adults more commonly have unilateral disease but in children this can be a bilateral process.
Examination
• The acute inflammatory process can occur anteriorly and present with acute erythema and swelling of the lids and globe.
• It may present as a myositis with restricted motility and pain with eye movement, as a scleritis, a dacryoadenitis, or in the orbital apex with few external signs but significant pain, dysmotility, and decreased vision.
• The presentation is variable depending on the tissues affected. Patients with orbital pseudotumor can have a fever and a leukocytosis (Fig. 12-2).
Imaging
• CT scanning will show thickening of the affected tissues such as enlarged muscles, thickened sclera, enlarged lacrimal gland, or an infiltrate in the orbital fat.
Special Considerations
• Rarely, there may be very few inflammatory signs and a more chronic fibrotic process that is termed sclerosing inflammatory orbital pseudotumor.
• This condition is not very responsive to treatment as treatment is geared toward eliminating inflammation and there is very little inflammation in this process.
• Systemic conditions, such as sarcoidosis, may cause a very similar picture.
Differential Diagnosis
• Orbital cellulitis
• Thyroid-related ophthalmopathy
• Lymphoma
• Sarcoidosis
• Wegener’s Granulomatosis
• Ruptured dermoid cyst
• Metastatic disease
Laboratory Tests
• Patients may have a leukocytosis, peripheral blood eosinophilia, elevated ESR, and a positive ANA. None of these are diagnostic.
Pathophysiology
• A pleomorphic cellular inflammatory response occurs and if not treated or not responsive to treatment there will be a resultant fibrotic response that will progress with time and result in chronic scarring.
Treatment
• Systemic steroids are the mainstay of treatment.
• There should be an improvement in symptoms in 24 to 48 hours.
• The longer the process has been present, the longer it can take for a clinical response.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


