6 Standard Operations for Acute and Chronic Sinusitis
Endoscopic sinus surgery has basically emerged from the operative treatment of chronic empyema or chronic hyperplastic sinusitis. The following description of standard operations is, therefore, orientated on these indications. The operations are rarely also applied to recurrent and complicated acute sinusitis if simple rhinosurgery fails. Other applications such as the endoscopic management of sinusitic complications, trauma, malformations, or neoplasia will be discussed in separate chapters, because they utilize combinations of the techniques described or require special modifications.
Operations in the Nasal Cavity
Septoplasty
In many cases correction of the nasal septum is a prerequisite for good exposure, for safe operating conditions, and for the creation of an ideal shape for the nasal cavity. Furthermore, it is often indicated on its own merits to improve ventilation of the chronically inflamed mucosa. The treatment plan should therefore include mobilization and straightening of the septum.

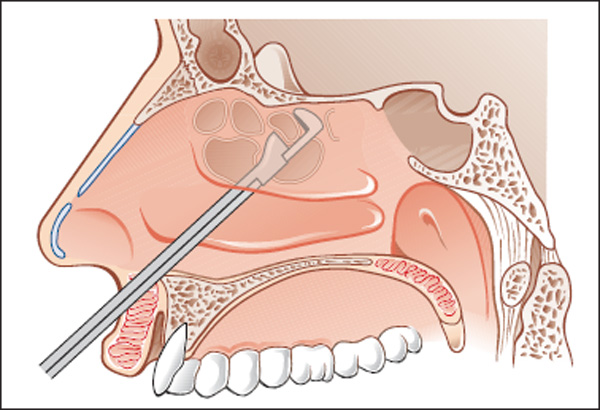
Fig. 6.1 Marked convex deviation of the nasal septum to the left side causing stenosis of the middle nasal meatus, thus promoting unilateral chronic pansinusitis by compressing the middle turbinate stenosing the semilunar hiatus.
The role of septoplasty as a flanking measure to eliminate one cause of chronic rhinosinusitis can easily be read from CT imaging of unilateral pansinusitis on the side of a marked deviation or spur, compressing the middle turbinate laterally and thus stenosing the semilunar hiatus (Fig. 6.1).
Septal resection as described by Killian with destruction of cartilage should be abandoned because it quite unnecessarily robs the septum of its support, and does not improve the function of the upper segment that is so important in the physiology of the airstream. It has been replaced by the cartilage-sparing technique originally described by Cottle. The method can naturally be modified in the individual case, and the following personal method is only one of many variations (Wigand 1978). The pitfalls of concurrent rhinoplasty and ESS (Millmann and Smith 2002) will be mentioned in Chapter 10.
A hemitransfixion incision is first made along the edge of the septal cartilage in the left or right nasal vestibule at the mucocutaneous junction (Fig. 6.2). The perichondrium is completely elevated through this incision down to the floor of the nose only on the side of the hemitransfixion using a semi-sharp dissector. This undermining is continued posteriorly beyond the junction of the cartilage with the perpendicular bone. The contralateral side of the cartilage may also be exposed as far as necessary for trimming or scratching/lifting the perichondrium around the inferior edge.

Fig. 6.2 Hemitransfixion incision in the left nasal vestibule over the entire length of the inferior edge of the septum.


Fig. 6.4 A piece of the perpendicular plate of the septum that has been removed (cm scale). It is reimplanted after being straightened at the end of the operation.
An exposure of both the premaxilla and the palatal ridges together with the prominent dorsal edge of the quadrangular cartilage is also executed on demand–”tunneling” of the posteroinferior segment of the anterior septal base (Fig. 6.3a, b) . This means chiseling off the obstructing lateral crests of the premaxilla and palatal processes (see Figs. 2.3 and 2.35). The frequently inrolled edge of the cartilage is then released backward following its long tail, which often forms the “ascending crest” beside the vomer, and is trimmed with strip excisions.
The vomer itself is completely dissected together with the perpendicular plate on both sides, and resected on demand. First, the mentioned junction between cartilage and bone is opened, and from here the perpendicular plate is denuded back to the sphenoid, and upward close to its insertion in the nasal dome. A central plate is then excised by chisel, trimmed on a side desk, straightened and narrowed if necessary, and replaced in its central position (Fig. 6.4, see also Fig. 2.33). The maneuver is completed with a partial resection of the protuberance of the vomer, mostly of its triangular block (Fig. 6.5). Good reformation of the septal infrastructure facilitates the endoscopic ethmoid surgery considerably, and contributes to easy aftercare and mucosal recovery.

Fig. 6.5 Histological transverse section of the triangular block of vomer with the inferior edge of the quadrilateral cartilage (*) inserting into it (Elastica–van Gieson,×4).
The last step of septal correction should be left until the endoscopic sinus procedure is finished so as to take full advantage of the septal mobility. When the quadrangular cartilage has been denuded on both sides, this last step of the septal procedure is the vestibular rotating suture, a special stitch (Fig. 6.6) that not only adapts the wound edges but also rotates the quadrilateral cartilage in an anterosuperior direction. The cartilaginous septum thus regains its previous tension with respect to the nasal dorsum, which it often loses after removal of the perpendicular plate. The cartilage is held in its original position by the rotating suture, and sinking of the weak triangle is prevented. Posterior rotation of the quadrangular cartilage is much more often the cause of saddling of the nasal dorsum than is resection of cartilage at the lower border. The counteraction is unnecessary when the septal cartilage has been dissected only on one side. When the plate is fragmentary from injury or previous surgery, a rotational fixation of its posteroinferior edge to the premaxilla by a Vicryl suture may help to lift the infrastructure. In addition to the cartilaginous rotation suture, two further deep interrupted sutures are placed through the wound edges to close the hemitransfixion incision securely.
Additional use of fibrin glue may be helpful both in the case of damage to the mucosa and for replantation of bone or cartilage. An adhesive is not usually needed. A moderate compression of the reconstructed septum over 3–4 days with bilateral splints (see Fig. 4.11) fixed by one or two mattress sutures has proved valuable for stabilization and prophylaxis of a septal hematoma. If there was a pronounced hemorrhage from blood vessels in the bone, and the septal mucosa remained intact, it might be wise to execute a small vertical incision in region III (see Fig. 2.30c) in order to provide an outlet for eventual postoperative bleeding. The treatment of epistaxis need not be described; it was comprehensively discussed together with the normal vascular supply by Stamm et al. (2000).
Nasal packing after septoplasty is not obligatory if the septal infrastructure appears fixed and there is no threat of a hematoma occurring. When combined with conchotomy or extensive sinus surgery, however, tamponade with Merocel sponge or gel sponge for one or two days is useful. The interposition of respiration tubes (see Chapter 4) is then beneficial.

Fig. 6.6 Diagram of a cartilaginous rotation suture for closure of a right-side hemitransfixion incision. A firm knot rotates the loosened quadrangular plate superiorly into its original position in the nasal columella.
There are pitfalls of concurrent rhinoplasty and ESS. In cases of concomitant chronic rhinosinusitis with severe deformity of the nose, for instance with a markedly deviated nose, the endoscopic exposure may be obscured and the postoperative wound cleansing hampered. In principle, ESS can be combined with rhinoplasty (Millmann and Smith 2002), but one should ensure that the immediate postoperative care of the ethmoids and sinuses will not be disturbed by longer-lasting nasal splinting and packing.
Turbinectomy
The various indications and techniques for narrowing the nasal turbinates (Clement and White 2001), particularly the inferior, do not need to be considered here. However, many ethmoid operations demand reduction of the inferior or middle turbinate, particularly if the nasal airway must be improved or the surgical field must be extended to give a good view and allow instrumentation for the treatment of sinusitis.
Inferior Turbinal Resection
It is often essential to resect the excessively hypertrophic cavernous soft tissue. For this purpose stitch cautery utilizing a CO2 laser has proved valuable and can be properly carried out as a separate outpatient procedure with local spray anesthesia. Immediate relief of the stuffy nose can be expected, but the patient must be informed about some transitory crusting and odor. In cases of extreme flabby hyperplasia, a strip turbinal resection with the long nasal scissors applied along the free lobular edge of the inferior turbinate is also satisfactory, although mild crusting and bleeding from the wound edges in the initial postoperative phase and pain during postoperative treatment are quite common. Treatment with bipolar caustic or fibrin glue is helpful. Bulky posterior tips (Fig. 6.7) are severed with sharp snares.

Fig. 6.7 Bulky posterior tips of the inferior and middle turbinates narrowing the choana. Transoral 90° endoscopic view.
Middle Turbinal Resection
The middle turbinate can be regarded as the guardian of the middle nasal meatus (Fig. 6.8a, b) . It protects th semilunar hiatus against noxious pollution, thus keeping the outlets of the paranasal sinuses clean. It can, on the other hand, obstruct their ventilation and drainage if hypertrophic or dysplastic. It is usually a painful obstacle for rigid endoscopy of the ostiomeatal unit and also for postoperative manipulations in the opened ethmoids. Trimming of the middle turbinate essentially facilitates a clear exposure of the middle nasal meatus. The author principally practices it with ethmoidal surgerywith a particular technique, which slims its free-hanging medial body while respecting its full height and its dorsal fixation at the sphenoid bone (Fig. 6.9a, b) . Utilizing a cutting ringconchotome, the curved hyperplastic edge is resected backward to its dorsal end. This trimming opens a broad gate to the middle nasal meatus, and facilitates the access into the ethmoid considerably without any injury of the olfactory cleft, thus preserving all the bioactive nasal mucosa. Disturbing hemorrhage from the turbinal vessels can be stopped with bipolar cautery.

Fig. 6.8 a, b Left middle turbinate occluding the middle nasal meatus. a Before medialization. b Uncinate process and bulla exposed after medialization of the middle turbinate.

Fig. 6.9 a, b Trimming of the middle turbinate for a broadened access to the middle nasal meatus and ethmoid (schematic drawing).
a Resection of the bulky edge respecting the height of the vertical ground lamella.
b The vertical ground lamella with crests of turbinal cells in its upper segment.
The middle turbinate may also require limited resection if its anterior end is polypoid and blocks access to the middle nasal meatus or the olfactory cleft (Fig. 6.10a, b) . In this case, conservative removal of the excess tissue with the curved nasal scissors or diathermy is indicated.

Fig. 6.10 a, b A soft polyp (*) hanging from the head of the middle turbinate.
a 30° angled endoscopic view.
b Histology of the soft polyp showing pseudo-erectile tissue rich in glands and vessels (Elastica–van Gieson,×3).
The tissue removed must be subjected to histological examination to show whether the lesion was a polyp rich in glands, a papilloma, or some other tumor.
Partial clipping may also be indicated for a paradoxical curvature (Fig. 6.11) occluding the common nasal meatus with the olfactory rim.
If the pneumatization of the turbinate is pronounced (concha bullosa), obstructing the middle meatus, thinning by longitudinal splitting is suitable (Fig. 6.12a–e) . An initial longitudinal incision with a size 15 scalpel, followed by the excision of its lateral lamella with a fissure knife or bone scissors, is worthwhile. In this way, the medial surface with its fine bony lamella is preserved, while the body of the turbinate and its cells can be recognized in steps. If the turbinate is less well pneumatized in its free part but cells are well developed in the upper part, then posteroanterior clearance of the middle and anterior ethmoid cells usually suffices.
If the middle turbinate is even better pneumatized, with cells extending into its inferior segment close to its edge, then all polyps must be removed from the cells of the middle turbinate complex (Fig. 6.13). Its medial lamella then hangs from only a narrow base and is even more unstable if the agger nasi is punched out lateral to the anterior area of the frontal duct. In this situation, it may be appropriate to cut back as much as 50% of the turbinate through a longitudinal curved incision with no regard for damage to the olfactory function. Personal observations show that normal olfaction is often preserved even if the middle turbinate is lost up to its fixed base. It appears that remnants of the turbinate along with the olfactory area of the septum are able to provide a sense of smell.
A large floating medial lamella of the turbinate can later cause “turbinate flutter” during respiration, and the large wound surface can adhere to the lateral ethmoidal wall. A drop of blood at this narrow point is enough to cause the adhesion. This situation can be managed successfully by folding the floating lamella of the turbinate over to prevent both turbinate flutter and unnecessary loss of valuable olfactory mucosa (Fig. 6.14a–d) . The mucous membrane is folded over to reach the roof of the ethmoid and is fixed with fibrin glue. This type of reconstruction has three advantages: stabilization of the fl uttering remnant of the turbinate, patency of the olfactory cleft, and minimization of the wound surfaces. The frontal duct must not be obstructed by parts of the turbinate. As prophylaxis against laterofixation of the weakened turbinate, its permanent (Bolger et al. 1999) or transitory (Lindemann et al. 2002) suturing to the septum was recommended. With respect to an open olfactory cleft, a definite synechia has to be avoided.

Fig. 6.11 Paradoxical curvature of the left middle turbinate and marked septal deviation to the contralateral side. Coronal CT.

Fig. 6.12 a–e Management of concha bullosa.
a 30° endoscopic view.
b Coronal CT scan showing the large turbinal cavity and marked septal deviation to the contralateral side compressing the right nasal cavity with its contents.
c Schematic drawing of the sagittal incision and resection of the lateral half of a diseased bullous concha. The resection follows the dotted line.
d Status after resection of the lateral part of the diseased bullous concha with restitution of drainage and ventilation.
e Preservation of the medial lamella and opening of the polypoid turbinate cells after lateral resection of the turbinate.

Fig. 6.13 Excised lateral wall of an extensively pneumatized middle turbinate (inch scale).

Fig. 6.14 a–d Remodeling of the medial turbinate.
a Only the thin medial lamella remains after clearance of the turbinate cells from the right side of the nasal cavity (70° telescope).
b After careful removal of the medial bony lamella, the mobile mucosal flap developed from the middle turbinate is folded laterally and glued in place. A compact turbinate body is thus attained without loss of the olfactory mucosa, and the olfactory cleft is widened (right nasal cavity, 70° telescope).
c, d Plastic reconstruction of the middle turbinate (schematic drawings).
Polypectomy
Polyps in the nasal cavity basically belong to a chronic polypous ethmoiditis and must be treated in this context. Only exceptionally are they limited to the middle nasal meatus or to the middle turbinate. If they are detected endoscopically in these regions, CT imaging of the paranasal sinuses is always indicated. Only if sinus surgery does not appear necessary or is contraindicated for certain reasons does a symptomatic solitary polypectomy using a sharp wire sling or a shaver appear justifi ed. Care must be taken not to lacerate the mucosal lining of the nasal dome. Scarification in this compartment is a frequent cause of hyposmia.
Removal of Foreign Bodies
Small foreign bodies such as pieces of paper, parts of plastic toys, or pellets (Fig. 6.15a, b) may lodge in the nasal airways and be difficult to remove without injuring the mucosa, turbinates, or septum. A simple withdrawal with pincers or hooks may become hazardous if previous attempts have pushed the objects into the depth, or if they are incrusted, becoming rhinoliths. These may grow and require endonasal surgery or even external surgery.
The exact position of a foreign body and the precise application of instruments must be monitored endoscopically. General anesthesia is seldom indicated (only for infants); local anesthesia and decongestion of the cavernous turbinates are often helpful to mobilize a fixed object.
Utilizing adequate blunt hooks from the ear surgeon’s armamentarium or a forceps, it is usually easy to grip the problem object and extract it anteriorly. Be careful not to push it into the pharynx, which could provoke its aspiration.
Biopsy and Tumor Removal
Biopsies can be taken for histology and localized areas of tissue can be removed very precisely under endoscopic control. A self-retaining speculum and the operating microscope may be useful for dissection in the nasal introitus and the anterior third of the nose, for example, for precise excision of papillomas from the nasal vestibule. However, the surgical endoscope comes into its own for manipulations in the posterior third of the nasal cavity. The endoscope is also a great help in transnasal biopsy of the nasopharynx. In most cases, local anesthesia suffi ces, but general anesthesia with packing of the pharynx may be more comfortable for both patient and surgeon if severe bleeding is to be expected, for example, after a punch biopsy of a nasopharyngeal angiofibroma or if anatomical narrowing makes access difficult for the biopsy forceps. The high-frequency diathermy needle with a slender grip and interchangeable hooks, loops, etc., has proved invaluable for bloodless removal of tissue specimens, and for dividing adhesions.

Fig. 6.15 a, b Jammed foreign bodies in the nasal cavity.
a Metallic nut behind the nasal valve.
b Plastic pearl below the inferior turbinat
Intranasal endoscopic surgery for tumors, described more fully in Chapter 11, may be successful depending on the site, extent, and pathology of the lesion, and it may also be used as a palliative partial resection or for complete excision with a healthy margin. Lesions with a narrow base or those confined to one turbinate are particularly suitable for complete removal. The endoscopic findings must be supplemented by tomography in most cases, to exclude extension beyond the nasal cavity and invasion of the skull base. Preferably the tumor should have been shown to be benign by previous biopsy. The technique is determined by circumstances: Lesions with a soft pedicle can be removed with the cutting snare, but broad-based sessile lesions require excision, possibly with division of their bony base with the chisel, and if necessary resection of the turbinate. Bulky benign lesions can be removed piecemeal using the punch forceps under endoscopic control. The base should be removed by drilling the underlying bone with a diamond burr. This method is particularly suitable for the treatment of circumscribed inverted papillomas, as personal experience extending over many years has shown.
Intranasal excision of a malignant tumor confi ned to the nasal cavity and adjacent paranasal regions, under endoscopic control, can be carried out with success after preoperative CT scanning for careful assessment of the extent of the lesion. This procedure is comparatively easy for small lesions whose complete extent is within the visual field of the endoscope (Fig. 6.16). Larger malignancies can also be removed under rigid adherence to procedure (see Chapter 11). Whenever they have invaded the facial skeleton or trespassed the anterior skull base, a combined endoscopic–external technique appears necessary. The treatment plan must include histological assessment of specimens taken from the apparently healthy margin of the wound, vigorous drilling of the underlying bone, and continuous close endoscopic follow-up.

Fig. 6.16 Circumscribed hemangiopericytoma (*) of the head of the middle turbinate. The histological diagnosis was provided by the Pathological Institute of the University of Erlangen–Nuremberg.
Under these circumstances, intranasal surgery for malignant tumors has, during recent years, emerged as an accepted therapy option.
Endoscopic Use of the Laser
Division of a choanal atresia in the newborn and infants using the operating microscope and a carbon dioxide laser has proved to be very valuable. It is simple, but application of the beam to the correct point can be obstructed by the turbinates or septal spurs. The nasopharynx should be protected before beginning coagulation. The technique and the aftercare will not be discussed at this point.
The carbon dioxide laser can be controlled carefully under the operating microscope but it can be directed upon only part of the nasal mucosa because the beam is directed forward. For this reason the argon or the Nd:YAG lasers are useful in the angular nasal cavity. In the latter case the laser beam can be conducted around corners by a flexible cable (see Fig. 4.10a) and directed to the target using special curved hollow probes; its action can be monitored by the irrigating-suction endoscope. The laser is the treatment of choice for coagulation of bleeding lesions, such as hereditary telangiectasia, and for the localized cautery of a hypertrophic inferior or middle turbinate.
If the laser is used for coagulation or excision of tissue with a cartilaginous framework, such as the septum or the nasal ala, the inevitable spread of heat can lead to chondronecrosis.
Operations on the Ethmoids
Indications
• Chronic or recurrent maxillary sinusitis
• Chronic hyperplastic polypoid sinusitis of the ethmoid and the maxilloethmoidal junctional zone
• Complications of inflammation
• Foreign bodies and trauma of the ethmoid and of the anterior skull base
• Tumors of the ethmoid and neighboring areas
• Transnasal access to the frontal and sphenoid sinuses, to the anterior skull base, and to the orbit and lacrimal sac
Principles
The operation should be tailored to the individual patient and the extent of the chronic sinusitis, but the goal must always be restitution of free aeration and drainage of the whole ethmoid compartment. Basically, the procedure consists of sharp resection of cell septa with their adherent soft tissues without laceration of neighboring healthy mucosa. The lining texture covering the roof and outer walls of the ethmoid should thus be preserved at any rate, even if diseased. The middle turbinate with its attachment at the roof of the ethmoids is a key landmark ensuring the security of the procedure. It may be partially removed depending on the extent of the disease, but the value of preserving or reconstructing the olfactory cleft must be stressed.
The middle nasal meatus is the gateway to the ethmoids. The functional pathway from the semilunar hiatus to the ethmoid infundibulum and then to the frontal sinus, the anterior ethmoid cells, and the antral cavity via the primary maxillary ostium should be exploited surgically. Ethmoid operations are usually combined with correction of the upper part of the nasal septum. The correct choice and direction of the instruments minimizes the danger of injury to the orbit and the anterior skull base, but a CSF fistula due to tearing of olfactory fibers may occur, and should be repaired immediately. Partial resections may be more difficult and more dangerous than complete exenteration if the surgeon has not acquired sufficient experience with the topography.
Operations on the ethmoid are usually carried out under general anesthesia. An increasing number of rhinosurgeons, however, prefer an intervention with local anesthesia. Topical application of lidocaine, and especially of cocaine, can be sufficient for minor operations. The latter also provides a marked local reduction of blood. Intraorbital block anesthesia of both ethmoidal nerves contributes considerably to a painless procedure.
Operative Technique
Anterior Partial Ethmoidectomy
This limited resection of the anterior ethmoids, often cited as “infundibulotomy” or “remodeling of the ostiomeatal complex,” aims at a recanalization of the draining system for the frontal and maxillary sinuses and the anterior ethmoid in case of its blockade by hyperplastic mucosa or polyps. While a simple resection of the uncinate process according to Killian opens only the semilunar hiatus (hiatotomy), a limited resection of the bulla and neighboring cell septa together with the uncinatectomy according to Messerklinger exposes both the ethmoidal infundibulum and the primary maxillary ostium, thus providing reventilation and drainage to the mentioned subregions (Stammberger and Posawetz 1990; see also more recent reports by Levine and Clemente 2005, Simmen and Jones 2005). Wide exposure of the infundibulum is often sufficient to induce recovery of severe hyperplasia of the sinus mucosa (Messerklinger 1979). This principle of treatment provides definite healing more often than simple nasoantrostomies. Because of the individual variation in shape of the middle meatus, surgical exposure of the infundibulum under endoscopic vision must be adapted to the type and extent of the resection of bone and mucosa.
The middle meatus can be well seen with the 25° telescope: The characteristic protrusion of the ethmoid bulla and the marked groove of the semilunar hiatus are easily located (Fig. 6.17). A secondary antral ostium is often to be found close to its posterior end, but it may be concealed or covered with swollen mucosa, or may be absent. The ethmoid infundibulum is an anterior prolongation of the semilunar hiatus lying between the ethmoid bulla and the uncinate process.
The ethmoid infundibulum can be exposed by opening the semilunar hiatus (hiatotomy) by careful removal of its walls, in particular the upper edge of the uncinate process . Polyps projecting from its gutter (Fig. 6.18a, b) must often be removed first with a delicate grasping forceps or with a shaver. A strip of mucosa and bone is then removed from the uncinate process using a sickle knife carried forward parallel to the upper edge of the hiatus (Fig. 6.19a, b) . A fine cutting forceps is placed in the existing gutter and is used to remove tissue from the uncinate process until the primary antral ostium, several anterior ethmoid cells, and the frontonasal duct are visible in the now open infundibulum, allowing free drainage (Fig. 6.20a, b) . If inflammatory hyperplasia is found in the cells of the bulla, the cells can be carefully opened from the hiatus, checked, and if necessary removed (Fig. 6.21a, b) . The procedure ends with minor procedures such as removal of polyps or minimal extension of the window at the maxillary ostium. A final inspection shows the ethmoidal infundibulum and some opened marginal cells with their preserved lining mucosa.

Fig. 6.17 Left middle nasal meatus with the complex of the middle turbinate, the bulla, and the uncinate process. The semilunar hiatus is visible as a thin upward-curved line (25° telescope).


Fig. 6.19 a, b Resection of the uncinate process to expose the ethmoidal infundibulum.
a Sickle knife at the start of the resection line (25° telescope).
b Resected segment with a millimeter scale above.

Fig. 6.20 a, b The opening of the anterior ethmoid cells after resection of the left uncinate process.
a The ethmoid infundibulum is thus exposed. A small polyp (*) lies centrally, and on the right there is a secondary maxillary ostium (arrow) in the anterior fontanelle (70° telescope).
b The ethmoidal infundibulum in its full length.

Fig. 6.21 a, b Anterior partial ethmoidectomy.
a Infundibulotomy and partial resection of the bulla. A white polyp (*) obstructs the view into the terminal recess anteriorly. On the left side a speculum beneath the middle turbinate can be seen (left side, 25° telescope).
b Anterior partial ethmoidectomy. Several small polyps have been removed after exposure of the infundibulum and the cells are opened. On the right side the opening of a newly created middle meatal antrostomy can be seen (70° telescope).
Anterior Complete Ethmoidectomy
Often chronic hyperplastic mucosal inflammation affects only the cells bordering the middle meatus, as can be well shown by CT scans (Fig. 6.22). Circumscribed posterior ethmoiditis is less common. Clearance of different regions of the ethmoid may therefore be indicated. The goal of anterior ethmoidectomy is complete exenteration of the anterior ethmoid with preservation of the mucosa lining its external wall and roof. The use of an operating endoscope with angled telescope is absolutely essential since residual cells walled off by scar tissue cause foci of recurrent ethmoiditis. Therefore, it is also advisable to secure free drainage for the frontal sinus. Blind resection without visual control is dangerous because perforation of the orbit or the anterior cranial fossa and tearing of the olfactory fibers, leading to a CSF leak, can happen more easily in the anterior than in the posterior ethmoid.

Fig. 6.22 a, b Chronic ethmoiditis confined to the left anterior ethmoid.
a CT scan showing circumscribed opacity of the right middle ethmoid (*) whereas the left side is clear.
b Endoscopic view after anterior partial ethmoidectomy (infundibulotomy). Exposure of the ethmoidal infundibulum after excision of the uncinate process and the bullar cells. The frontal recess of the ethmoidal bulla with a small slit into the nasofrontal duct is visible. Note the preservation of the lining mucosa (70° telescope).


Fig. 6.24 a, b Obstructive nasal polyposis.
a Polyp obstructing the view on the left middle turbinate.
b After careful removal of the polyps, the left middle turbinate and the middle meatus come into view. Mucosal defects and partial opening of the ethmoidal cells can make orientation difficult (25° telescope).

Fig. 6.25 Sharp anterior ethmoidectomy. Note the whitish areas of preserved lining mucosa at the ethmoidal roof between the small resection wounds after sharp resection of the ethmoidal cells (70° telescope).
The most popular method of anterior complete ethmoidectomy is based on that originally described by Halle (1923), in which the anterior ethmoid is entered via the semilunar hiatus and the ethmoidal bulla (Fig. 6.23). Polyps filling the nasal cavity (Fig. 6.24a, b) are removed with forceps or shavers after intensive decongestion of the mucosa with epinephrine-soaked pledgets, providing a reliable view of the shape and position of the often markedly atrophic or polypoid middle turbinate. After exposure of the semilunar hiatus and the ethmoid infundibulum, and opening of the bulla widely, the ethmoid system is opened cell by cell with sharp cutting forceps and punch (see Figs. 6.41,6.42). Under endoscopic or microscopic control the suprastructure of the middle turbinate and the lateral wall are dissected with utmost preservation of their lining mucosa (Fig. 6.25). Then the honeycomb of cells and polyps is removed lateral to the medial lamella of the turbinate, preserving the stump of the middle turbinate. The cells are removed with the punch, or opened with a sharp upward-curved forceps and cleared up to the base of the skull. It is useless to plan a previously determined route of removal of named cell tracts. All cells lying between the body of the middle turbinate or its medial lamella and the lateral ethmoid wall (the lamina papyracea) should be broken down gently and removed. The ethmoid gallery is thus cleared between the middle turbinate and the orbital wall as far as the overhang of the agger nasi, which can be resected (Fig. 6.26). An angled telescope must be brought into use at this point for the further-rostral part of the procedure. Once again the necessity for care around the point of insertion of the middle turbinate to the skull base is emphasized: a row of olfactory fibers runs through the skull base onto its medial lamella and these can be damaged. Firm resistance during breaking down of the party walls of the ethmoid cells or removal of polypoid mucosa may indicate that an olfactory fiber has been grasped in the instrument. Energetic tearing is always to be avoided, as ethmoid cells and their mucosa can almost always be removed without force. A particularly dangerous dural tear may also be signaled by the oozing of dark venous blood.

A small CSF leak indicates tearing of an olfactory fiber (Fig. 6.27a, b) . The operation should be interrupted, and the fistula closed as follows: First, it is inspected very carefully with the endoscope, and the integrity of the neighboring bone is tested by careful probing with a fine dissector. Mucosal remnants are removed from a surrounding area of 2–3 mm with a small double forceps. An oval mucosal flap is now harvested from the free edge of the inferior turbinate, carefully smoothed on its internal surface and freed of bone, but not overly thinned. This free mucosal graft is fixed over the fistula with a wide overlap using fibrin glue after hemostasis has been achieved. The procedure ends with an endoscopic check and packing, using two layers of moist Gelfoam left in place for more than 2 weeks. Under this lies a layer of packing of gauze strips soaked in aureomycin, exerting slight upward pressure; it too should be left in place for at least 10 days. The defect should heal within 4 weeks (Fig. 6.28). Small perforations of the anterior base of the skull due to other causes can be managed in a similar manner.

Fig. 6.27 a, b CSF fistula after tearing of an olfactory fiber in the right nasal cavity.
a CSF fistula resulting from a tear of the olfactory mucosa at the upper attachment of the middle turbinate. The olfactory fibers are visible.
b Closure of the fistula with a glued mucosal flap from the inferior turbinate (*). The frontal sinusotomy lying anterosuperiorly is seen from below.
The ethmoidal roof deserves particular attention: one should be anxious to identify and spare the long crest containing the anterior ethmoidal artery. It is normally located at the area where the distance between the medial orbital wall and the middle turbinate is shortest. Anteriorly, the most rostral cells are more easily dissected after a marginal resection of the agger nasi . This procedure also plays a key role in opening of the frontal sinus and in the prevention of recurrent polyps and cicatricial stenosis, but it destabilizes the middle turbinate, whose anterior edge merges into the agger nasi. One jaw of a 90° upward-cutting punch is passed under the bony overhang uniting the most anterior part of the medial lamella of the middle turbinate with the lateral ethmoid wall (Fig. 6.29). Under it open the agger nasi cells that form part of the most anterior ethmoid cell system, which are usually affected by diffuse polyposis. This step can easily be done during ethmoidectomy without endoscopic control, but if it is omitted, loculated sinuses remain, hindering free drainage from the frontal sinus. On the other hand, too aggressive resection of the agger nasi can damage the lacrimal canal running within it.


Fig. 6.29 Diagram of the exposure of the anterior ethmoid cells by resection of the agger nasi.

Fig. 6.30 The straight and 45° upward curved sharp forceps are very suitable for the mucosa-preserving resection of the ethmoid cells.

Fig. 6.31 Exenterated and healed left ethmoid sinuses with the anterior ethmoid artery running transversely in a thin bony shell (*). The frontal sinus has been widely fenestrated from below and can be seen opening anterosuperiorly. The olfactory cleft (**) and the medial lamella of the middle turbinate can be seen on the left-hand side of the picture (70° telescope).
Complete exposure of the most anterior ethmoid cells demands the help of the 70° telescope. The first step is uncovering the lateral wall of the ethmoid that tapers both in height and breadth as it runs anteriorly. A specially designed, rounded, 45° upward-cutting ethmoidal forceps is valuable for this step: it must always be introduced parallel to the lamina papyracea. The bony septa inserting perpendicularly into the lamina papyracea can be broken down and the surface smoothed safely by closing its jaws (Fig. 6.30).
The most ant erosuperior part of the ethmoid system is often relatively acellular and it varies widely in form. Also, a slender upper track of cells sometimes running forward over the larger cells along the base of the skull can escape the naked eye. Endoscopic inspection is therefore necessary to pick up these small niches and clefts, and to inspect the recesses bulging laterally into the orbit.
Complete removal of mucosal polyps from the lateral anterior ethmoid cell systems is particularly important in massive polyposis because recurrence can easily arise from remnants that are readily overlooked at this point. Small paraturbinate cells or recesses of the ethmoid are occasionally found during antrostomy even lying lateral to the insertion of the inferior turbinate, and they can be a source of recurrence.
With the angular telescope it is always easy to see the transverse bar housing the anterior ethmoid artery in the anterior part of the ethmoid roof (Fig. 6.31). This bulge is an important landmark forming the boundary between the danger area of the ethmoid containing olfactory fibers and the ascending part of the ethmoid roof or the posterior wall of the frontal infundibulum lying a few millimeters in front of the bar. The two are usually separated by only one cell. If the artery has been damaged with the punch, the bleeding can be controlled quite easily using bipolar coagulation, but the arterial stump can retract into the orbit, causing a massive extraperiosteal or subperiosteal hematoma and leading to exophthalmos or even blindness caused by compression of the optic nerve. Swelling or hematoma of the eyelids are harmless and are treated by ice packs; but orbital hematoma, immotility of the eyeball, mydriasis, or an absent light refl ex demand immediate decompression of the orbit by emergency measures such as removal of the lamina papyracea and incision of the periorbita, eventually combined with a lateral canthotomy (see Chapter 9).

Fig. 6.32 a, b Exposure of the nasofrontal duct.
a A small polyp (*) obstructs the view into the nasofrontal duct after exposure of the anterior ethmoid cells.
b A free view of the frontal duct is obtained only after endoscopic removal of the polyp (70 ° telescope).
If the orbital periosteum is breached, allowing orbital fat to enter the nasal cavity, the protruding tissue is replaced and possibly scarified using bipolar coagulation. This procedure should of course be used only for small defects. For added safety, a small piece of lyophilized dura can be fixed over the defect with fibrin glue.
In cases of marked polyposis of the anterior ethmoids it appears prudent to take care of a free frontoethmoidal communication. One can often find the frontal recess of the ethmoid opening into a nasofrontal duct, or will reach the infundibulum of the frontal sinus directly after removal of occluding polyps (Fig. 6.32a, b) or of a last cell, which is normally situated in front of the anterior ethmoid artery. It is sometimes difficult to identify marginal cells in the frontal infundibulum or at the frontal skull base if they are small and covered by hard bone. An anterior ethmoidectomy normally stops dorsally at the oblique ground lamella of the middle turbinate. The maxillary cavity is often opened accidentally (Fig. 6.33).

Fig. 6.33 Opening of the left antrum into the middle meatus by anterior ethmoidectomy. The medial lamella of the atrophic middle turbinate has been preserved. The anterior ethmoid cells filled with polyps lie under the agger nasi (70° telescope)
If the frontal duct is still not visible after exposure of the most anterior cells under the agger, its position is determined by careful probing and its lumen is exposed by removal of overlying polyps (see Fig. 6.32a, b) . Scarring after cell removal may occlude a previously open communication. The surgeon has to decide on a prophylactic frontal sinusotomy in the individual case.
The middle turbinate may be left entirely intact at infundibulotomy or anterior ethmoidectomy for circumscribed ethmoiditis. Although disease of individual cells may require the cells to be opened and the lateral part of the turbinate to be removed, its medial surface should be completely preserved.

Fig. 6.34 a, b Posterior ethmoidectomy with transethmoidal sphenoidotomy.
a A view of the posterior ethmoid cells after perforation of the basal lamella of the left middle turbinate (25° telescope).
b After removal of the posterior ethmoid cells the anterior wall of the left sphenoid sinus and its ostium come into view (70° telescope). It remains partially covered by the posterior attachment of the middle turbinate (* indicates ethmoid roof; ** indicates sphenoid ostium).
Dissection of the olfactory cleft requires special attention. One of the main symptoms of chronic sinusitis is loss of the sense of smell, usually due to mechanical obstruction of the olfactory cleft. The sense of smell may return rapidly or gradually after the operation, provided that enough olfactory epithelium remains following restitution of aeration and drainage. It is doubtful whether the olfactory epithelium is capable of regeneration by surface expansion. Great care must therefore be taken, even during minor procedures such as polypectomy, to preserve mucosa on the upper third of the medial lamella of the middle turbinate and on the corresponding surface of the septum, to lacerate as little mucosa as possible, and to preserve bone. If ulceration in this region can be prevented– for example, by extremely careful diathermy removal of polyps and adhesions under endoscopic control– the prospects of recovery of the sense of smell are good. Unfortunately, repeated extraction of nasal polyps in the doctor’s office without correction of the septum and without clear operating conditions often leads to a superficial defect of the turbinate and septum, with resulting synechiae of the upper nasal cavity. Many of these patients go through life with no sense of smell.
Posterior Ethmoidectomy
An isolated posterior ethmoidectomy sensu strictu without exposure of at least parts of the anterior ethmoid is technically impossible and virtually never indicated. It may become practicable and useful, however, in connection with operations on the sphenoid sinus for various reasons. Its most frequent implementation, in combination with an anterior ethmoidectomy as a total mucosapreserving ethmoidectomy, is required as treatment of diffuse chronic ethmoiditis.
After exposure of the ground lamella of the middle turbinate in its oblique portion, this partition is carefully perforated with a sharp small Blakesley forceps in a horizontal direction, parallel to the sagittal plane. One has to keep the course of the skull base in mind and to avoid an upward-directed penetration. Skull base lesions with CSF leaks may otherwise be encountered. Injuries of the orbit after too forceful puncture in an incorrect direction have also been reported. After a first ouverture, the exenteration is executed with straight and angled sharp forceps and punches of different sizes (Fig. 6.34a, b).
The posterior ethmoid labyrinth is thus exenterated, switching from the anteroposterior to a posteroanterior direction. Figure 6.35 a, b shows some remnant cells with their party walls. Polypoid mucosal edema, tenacious mucus, or pus often ooze out in cases of polypoid ethmoiditis. The tangle of cell walls and polyps is removed carefully using a sharp cutting forceps; the instrument must always be directed posteriorly. At a point from 1 to 2 cm above the upper edge of the posterior nasal choana there is no great danger of perforation of the base of the skull because the surgeon encounters the thick anterior wall of the sphenoid sinus or the rigid plate of the sphenoid plane if he goes too high.
It is advisable not to expose the posterior ethmoid cells as far as the ethmoid roof directly at this point, but first to expose and remove the anterior wall of the sphenoid sinus , to avoid dissection toward the base of the skull (Fig. 6.36). The level of the roof of the ethmoid sinuses can be deduced from the direction of the easily visible roof of the sphenoid so that resection of the posterior ethmoid cells with a punch can now proceed safely in a posteroanterior direction (see Fig. 2.61). The blunt end of the punch cannot perforate the anterior cranial fossa even if excessive pressure is exerted.

Fig. 6.35 a, b Posterior ethmoidectomy with small sphenoid sinusotomy.
a After a posterior ethmoidectomy with involuntary posterior resection of the middle turbinate, the anterior wall of the sphenoid is exposed (*). The upper edge of the choana lies at the lower edge of the picture (70° telescope).
b The anterior wall of the left sphenoid sinus has been opened and a view of the roof of the cavity above (*) is shown. The base of the skull is reached in this manner (70° telescope).

Fig. 6.36 Removal of the anterior wall of the sphenoid sinus by a punch. There is no danger to the optic nerve and the carotid artery, but brisk bleeding from the sphenopalatine artery is frequent.
The lateral boundary of the posterior ethmoid demands care: Occasionally the canal of the optic nerve may form a visible bulge or can even be surrounded by an extensive Onodi cell so that it lies almost completely within this cell (Fig. 6.37a–c) . However, the optic nerve is safe from injury if the forceps is not directed laterallyduring this first phase of removal of the posterior ethmoid cells but introduced toward the anterior wall of the sphenoid sinus in the midline, parallel to the septum.
The consecutive dissection of the posterior ethmoids can usually be carried out without difficulty, with total preservation of the middle turbinate, provided that the ethmoid has not yet been destroyed by polyposis with necrosis or by scarring after previous surgery, and provided that the ethmoid does not extend far laterally below or above the optic nerve (Onodi cell). Clear endoscopic r microscopic visualization is essential.

Fig. 6.37 a–c Dangerous course of the optic nerve through the posterior ethmoid and sphenoid.
a Coronal CT scan showing the prominence (arrow) of the optic nerve channel in the left sphenoid cavity.
b The opened lateral wall of the posterior ethmoid with the optic nerve (*) in direct reach of the sharp forceps.
c Exposure of the optic nerve in an Onodi cell during posterior ethmoidectomy.

If trauma or tumor growth requires a broader exposure of the posterior ethmoid compartment, one should not hesitate to resect the posterior one-third or one-half of the middle turbinate for free access. This procedure (Fig. 6.38) is especially suitable for major resections of the sphenoid (Fig. 6.39a–c).
Total Ethmoidectomy
For the treatment of initial stages of chronic sinusitis and of circumscribed lesions, a partial resection of the ethmoid may be an adequate procedure. Cases of advanced, mostly diffuse, sinusitis, however, require its complete exenteration (Fig. 6.40a, b) . The latter term must not be confused with radical ethmoidectomy, which would imply the removal of the diseased mucosa. Endoscopic surgery, in contrast, aims at the utmost preservation of the mucosa, respecting the lining texture at its outer walls. Total ethmoidectomy, though removing all cell septa and opening all marginal cells, is therefore conservative surgery. For this purpose, the use of sharp bone cutting forceps and punches is mandatory (see Fig. 4.7a) . Blunt instruments, like the Blakesley forceps, breaking instead of cutting the cell septa, often tear off adjacent lining mucosa, thus unnecessarily exposing the underlying bone. Induction of scar formation and of osteoneogenesis are unwanted sequelae.
If massive polyposis hides the entrance into the ethmoids, a powered instrument like the “shaver” is useful for initial clearance. It removes polyps more precisely than blunt forceps or slings, which are also likely to injure healthy mucosa at the turbinates or septum. The subsequent ethmoidectomy thus starts under better preconditions, and can be performed with less blood loss (Fig. 6.40b) . Continuous hemostasis with cotton swabs, soaked in epinephrine, may contribute to a perfect dissection under endoscopic or microscopic control.
The frequently necessary combination of a complete ethmoidectomy with surgery of the great cavities will be summarized as pansinus operation after the description of the related sinus surgery on p. 131.

Fig. 6.39 a–c Anterior wall of the sphenoid sinus.
a Covered by the posterior attachment of the middle turbinate.
b Exposed (*) by resection of its posterior third. The left choana lies below.
c Fenestration of the anterior sphenoid wall (25° telescope).

Fig. 6.40 a, b Massive nasal and paranasal polyposis requiring an endoscopic pansinus operation.
a Axial CT image.
b Posterior ethmoid cleaned. The upper edge of the choana is at the lower edge of the picture. The anterior ethmoid and nasofrontal transition still blocked by small polyps.
Anteroposterior Approach
This most common procedure combines both the abovedescribed methods of anterior and posterior ethmoidectomy, starting with resection of the uncinate process and the bulla. Its advantage lies in the principle of opening the focus of chronic ethmoiditis–the ostiomeatal complex– first and subsequently following the routes of its proliferation. The procedure can thus be individually adapted to the extent of the pathology. Its disadvantage lies in the danger of involuntary injury of the anterior skull base because the cutting and perforating instruments are necessarily directed posterosuperiorly against the ethmoidal roof (Fig. 6.41). However, a soft and careful dissection supported by the knowledge of landmarks and distances (see Chapter 2), will avoid such misfortune.
Posteroanterior Approach
Either performed as an independent technique or in combination with the anteroposterior approach, the posteroanterior full exenteration of the ethmoids has proved effective and safe for cases with advanced polyposis or difficult-to-manage scar formation. Whenever there is restricted view of the ethmoidal walls and skull base, due to pathological tissue or hemorrhage, this posteroanterior process will be of great help, because the retrograde use of angled punches with a blunt tip (Fig. 6.42) instead of acute forceps excludes greater risks.
The procedure is usually premised upon a transnasal opening of the sphenoid sinus (see p. 110). After resection of its anterior wall, one will look at its roof and proceed anteriorly, resecting the posterior ethmoid cells, then the bulla, turbinal cells, and finally the anterior ethmoid with good orientation at the sagittal ground lamella of the middle turbinate and at the lateral ethmoidal wall, the orbital partition. This dissection, employing sharp punch or angled forceps, allows a quick and safe exenteration of the ethmoid with preservation of the lining mucosa at roof and outer walls. It usually also prevents injury of the ethmoidal arteries crossing the ethmoid roof. The most anterior cells can be reached easily after marginal resection of the agger nasi.

Fig. 6.41 Anteroposterior ethmoidectomy (schematic drawing). The mouth of the biting forceps is directed against the skull base.
The main prerequisite for the safety of the procedure is an optimal view of the surgical field. It is true that a large part of the procedure can be carried out under direct vision through the nostril using a long nasal speculum, but for the deeper regions optical magnifi cation is necessary, using the operating microscope where forward vision suffices and the angled telescope to see around corners. The author usually uses a 70° angled telescope with an irrigation-suction handpiece.
The second principle is complete opening of the cells to guarantee healing of the chronic polypoid mucosal inflammation. Remaining cells are often the point of origin of persistent disease. These two aspects therefore led us to develop complete ethmoidectomy, in which an entirely visible ethmoid compartment is created with no remaining narrow areas and no remaining cells. The resulting wide upper nose was a new and surprising experience, which did not lead to drying of the regenerating mucosa or to the development of ozena.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


