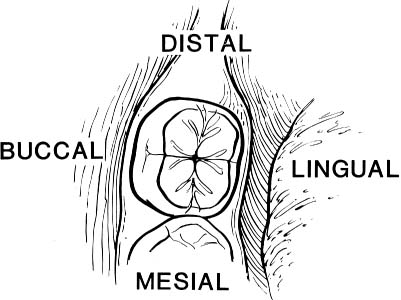
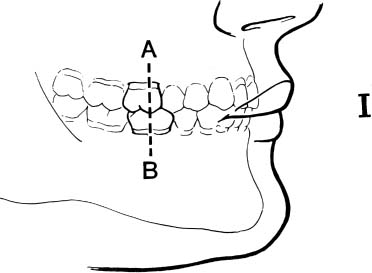
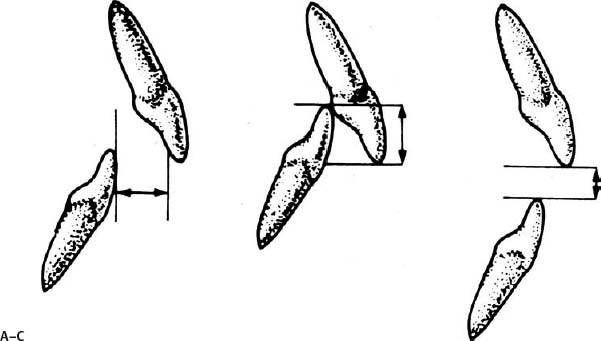
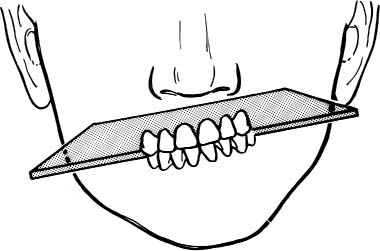
5 Mandibular Facial Fractures Post-traumatic facial deformities pose some of the most challenging problems confronting the reconstructive surgeon. The main objectives in the initial repair of facial fractures are restoration of function and reestablishment of the preinjury appearance. Even in the best of hands, acute management of maxillofacial trauma may be less than optimal. Delay in initial management due to associated life-threatening injuries, failure to recognize the magnitude of injury, unsuccessful exposure and reduction, and operative complications may all contribute to secondary cosmetic deformity and dysfunction. Such deformities may cause pain and impair mastication, vision, speech, and hearing. The cosmetic abnormality may lead to deleterious emotional and social sequelae.1 Secondary reconstructive procedures for correction of persistent post-traumatic maxillofacial deformities can provide excellent outcomes when used appropriately, and improvement in any preexisting, preinjury deformities may even be possible. However, adequate repair of the initial injuries in a timely fashion is still the optimal management. This chapter focuses on secondary reconstruction of post-traumatic mandibular deformities, and the following chapter focuses on secondary reconstruction of post-traumatic maxillary deformities. Many of the basic principles remain the same regardless of the site of injury. Minor deformities not affecting occlusion can occasionally be adequately camouflaged with onlay bone grafts or alloplastic implants. However, severe deformities and those causing malocclusion are usually not adequately corrected with simple bone grafts and implants. In these cases, restoration of normal anatomical position of facial bones typically involves complete exposure, osteotomies with repositioning of displaced bone, rigid internal fixation, and bone grafts to fill gaps left by the movements.2 Multiple staged operations are frequently necessary to correct complex deformities involving multiple facial bones.3 An understanding of normal occlusion and classification of malocclusion is critical in the management of post-traumatic deformities, especially those involving the mandible. Simply stated, occlusion is the relationship of the maxillary teeth to the mandibular teeth. Accurate evaluation of occlusion requires evaluation in the sagittal, transverse, and vertical dimensions. Molars usually have four cusps, with grooves between these cusps (Fig. 5.1). The cusps adjacent to the tongue are the lingual or palatal cusps, and those adjacent to the cheek are the buccal cusps. Those cusps located anterior on the molar toward the dental midline (the space between the central incisors) are referred to as mesial, and those located posterior on the molar away from the dental midline are distal. This dental terminology, in which the molars are distal and the incisors are mesial, should not be confused with other terminology that uses the vertical center of the body as midline in which the molars are proximal and the incisors are distal. The term intercuspation refers to the fitting together of opposing molar cusps and grooves. The posterior maxillary teeth are normally shifted one-half tooth width distal (or posterior) to the corresponding mandibular teeth because the maxillary central incisors are approximately one-half tooth wider than the mandibular central incisors. This shifting prevents the cusps from striking end on end, allowing for normal intercuspation. Fig. 5.1 Dental terminology. Mesial means toward the dental midline (the space between the central incisors). Distal means away from the dental midline. Buccal is adjacent to the cheek. Lingual is adjacent to the tongue. (From Donald PJ. The Surgical Management of Structural Facial Disharmony: A Self-Instructional Package. Washington, DC: American Academy of Otolaryngology–Head and Neck Surgery; 1985:12. Reprinted with permission.) Fig. 5.2 Angle’s classification of occlusion. Class I normal or centric occlusion. (From Donald PJ. The Surgical Management of Structural Facial Disharmony: A Self-Instructional Package. Washington, DC: American Academy of Otolaryngology–Head and Neck Surgery; 1985:13,14, 15. Reprinted with permission.) In the sagittal plane, molar relationships are described independent of anterior dentition relationships. The Angle classification system refers only to the anteroposterior (mesial-distal) relationship of the maxillary first molar with the mandibular first molar. In Angle class I occlusion, which is considered normal or centric occlusion, the mesial buccal cusp of the first maxillary molar intercuspates with the buccal groove of the first mandibular molar (Fig. 5.2). In Angle class II malocclusion, the mesial buccal cusp of the first maxillary molar is mesial (anterior) to the buccal groove of the first mandibular molar. In Angle class III malocclusion, the mesial buccal cusp of the first maxillary molar is distal (posterior) to the buccal groove of the first mandibular molar. A posterior open bite occurs when there is no intercuspation at all and a vertical space exists between the mandibular and maxillary molars. Relationships of the anterior teeth are described independently of molar relationships. The term overjet refers to the horizontal relationship of the maxillary incisors to the mandibular incisors. Normal overjet occurs when the maxillary incisors are 2 to 4 mm anterior to the mandibular incisors. Inadequate overjet, also termed a nterior crossbite, is present when the maxillary incisors are posterior to the mandibular incisors, and excessive overjet is present when the maxillary incisors are > 4 mm anterior to the mandibular incisors. The term overbite refers to the vertical relationship of the maxillary incisors to the mandibular incisors. Normal overbite occurs when the incisal edges of the maxillary incisors overlap the incisal edges of the mandibular incisors by 2 to 4 mm. Excessive overbite, also called deep bite, is present when there is > 4 mm of vertical overlap between the mandibular and maxillary incisors. An anterior open bite exists when there is no overlap and a vertical space exists between the mandibular and maxillary incisors (Fig. 5.3). Transverse relationships refer to the side-to-side positioning of the posterior dentition. Because the maxillary arch is wider than the mandibular arch (due to the greater width of the maxillary central incisors compared with the mandibular central incisors), the maxillary dentition normally overlaps the mandibular dentition in the transverse plane. The maxillary incisors and cuspids are normally anterior (labial) to the mandibular incisors and cuspids. The lingual cusps of the maxillary bicuspids and molars normally fit in the grooves between the lingual and buccal cusps of the mandibular bicuspids and molars, whereas the buccal cusps of the mandibular bicuspids and molars normally fit in the grooves between the lingual and buccal cusps of the maxillary bicuspids and molars. A lingual crossbite is present when the maxillary buccal cusps either fit end to end with or are lingual (medial) to the mandibular buccal cusps. When the maxillary lingual cusps are buccal (lateral) to the mandibular buccal cusps, a buccal crossbite exists (Fig. 5.4). Fig. 5.3 Incisor relationships. (A) Overjet. (B) Overbite. (C) Open bite. (From Bailey LJ, Simmons KE, Warren DW. Orthodontic problems in children. In: Bluestone CD, Stool SE, Kenna MA, eds. Pediatric Otolaryngology. Vol 2. Philadelphia: WB Saunders; 1996:1030. Reprinted with permission.) Fig. 5.4 Transverse dental relationships. (A) Bilateral buccal crossbite. (B) Bilateral lingual crossbite. (C) Unilateral lingual crossbite (left) and normal relationship (right). (From Powell N, Humphreys B. Considerations and components of the aesthetic face. In: Powell N, Humphreys B, eds.: Proportions of the Aesthetic Face. New York: Thieme-Stratton; 1984:11. Reprinted with permission.) Another important occlusal concept to be aware of is the curve of Spee, which represents a gentle superior curvature in the occlusal plane from posterior to anterior (Fig. 5.2). Abnormalities in this curvature can result in vertical malocclusion. For example, an anterior open bite exists when the maxillary curve of Spee is greater than the mandibular curve of Spee, whereas a posterior open bite occurs when the mandible has a greater curve of Spee than the maxilla. The anterior plane of occlusion may be abnormal as well. For example, an asymmetric mandibular or maxillary arch can result in an obliquely oriented bite (Fig. 5.5). Finally, the abnormal position of one or two teeth is not always a reflection of an underlying bony abnormality. The term version refers to a single tooth in crossbite with surrounding teeth that are in a normal relationship. The abnormally positioned tooth is labeled by the direction in which it is displaced, such as in lingual, palatal, or buccal version. Fig. 5.5 Obliquely oriented bite. (From Donald PJ. The Surgical Management of Structural Facial Disharmony: A Self-Instructional Package. Washington, DC: American Academy of Otolaryngology–Head and Neck Surgery; 1985:17. Reprinted with permission.) A patient with a post-traumatic deformity may have had a preinjury malocclusion. Although often difficult to delineate, the preinjury malocclusion can sometimes be determined from flat surfaces on the teeth caused by occlusal contact, termed wear facets. Radiographs and intra-operative visualization may also aid in evaluating preinjury relationships. However, as the secondary post-traumatic deformity ages, new wear facets form and skeletal deformities remodel, making it even more difficult to determine the preinjury state. In some instances it may be possible and desirable to correct preinjury malocclusion, which must be planned in conjunction with correction of the post-traumatic deformity. Once the concepts of occlusion have been grasped, it is important to understand that any combination of these occlusal relationships can occur in the post-traumatic deformity as a result of malunion or nonunion. Maxillary and mandibular position can be excessive, deficient, or simply malaligned in the sagittal, transverse, and/or vertical dimension. These deformities must be thoroughly analyzed and characterized to determine the appropriate means of correcting the post-traumatic deformity. Successful management of post-traumatic facial deformities begins with a comprehensive pretreatment assessment followed by a well-organized treatment plan, which may include orthodontics and multiple staged procedures. Diagnosis begins with a history of the mechanism of injury, any previous attempted repairs, and any subsequent complications. Insight into the condition of the tissues involved in the deformity is important because fibrosis of surrounding soft tissue from scar contraction limits skeletal movements and the success of bone grafts.2 During physical examination, skeletal abnormalities and classification of occlusion are evaluated. In particular, temporomandibular joint function should be documented, including interincisal opening distance, translation of the joint, and crepitus or pain in the joint. Any cranial nerve or vision dysfunction should also be documented.1 Anthropometric measurements should be obtained to provide quantitative analysis of specific facial structures and their relationships with each other.4 Pre- and postinjury photographs are helpful both as a baseline record and in treatment planning. Radiographic studies provide the definitive analysis of skeletal abnormalities. A panoramic radiograph provides excellent information about the craniofacial skeleton. Lateral cephalograms are crucial in assessing skeletal and occlusal relationships, and anteroposterior cephalograms are required for any asymmetry. There are multiple cephalometric analysis systems described in the literature, each with its own strengths and weaknesses (Fig. 5.6).5 The surgeon must choose a system with which he or she is comfortable and become very familiar with its particular normative data as well as its strengths and weaknesses. Some of the typical cephalometric angular measurements are listed in Table 5.1
Occlusion and Classification of Malocclusion

Pretreatment Assessment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


