Infections of the Ear
John Hill
Introduction
Infections of the external and middle ear have similar presentations. A good history, coupled with examination of the ear under magnification after cleaning out the ear canal, is necessary to achieve the diagnosis. Significant vital structures crowded in a small area, proximity to the intracranial compartment and the variety of infectious syndromes makes this a challenging aspect of ENT practice.
Infections of the pinna
Pre-auricular sinuses are commonly asymptomatic and require no treatment. They appear as small pits or dimples anterior to the root of the antihelix. More extensive sinuses will collect squamous debris and can become infected. Incision and drainage will be needed if an acute abscess develops but formal excision of the tract is necessary to prevent recurrence (4.1).
Sebaceous cysts occur in the lobule of the ear and can become infected, but most infections in this area are secondary to ear piercing. Abscesses will require incision and drainage (4.2).
Infection of the perichondrium of the pinna can be secondary to an infected wound on the pinna or an otitis externa. The pinna becomes thickened, erythematous, and tender (4.3). Treatment should be prompt with broad-spectrum intravenous antibiotics initially. If untreated, the infection leads to a loss of cartilage and a cauliflower ear appearance.
Infections of the external ear canal
The squamous epithelium of the tympanic membrane and ear canal is migratory in nature. The squamous epithelium over the drum is very thin and is only one cell thick. The skin
becomes progressively more stratified towards the meatus of the ear canal but remains thin throughout the external ear. The confined space of the ear canal means that it is not possible to have a desquamating stratified squamous epithelium on the drum or the ear canal. If this were the case the desquamated cells would collect in the ear canal and lead to a build up of debris. The migratory nature of the epithelium avoids this problem. The squamous epithelium grows out radially across the surface of the drum until it reaches the annulus and then grows out laterally along the ear canal. The ceruminous glands, which produce the wax, are only located in the outer third of the ear canal. As a result, in a normal ear, the skin gradually migrates out towards the meatus taking excess wax with it. The normal ear is self-cleansing and the antiseptic, hydrophobic nature of wax keeps the medial end of the external ear canal relatively clean with only scanty growths of commensals present. Typically these are Staphylococcus epidermidis, Corynebacterium spp., Staphylococcus aureus, and Streptococcus viridans.
becomes progressively more stratified towards the meatus of the ear canal but remains thin throughout the external ear. The confined space of the ear canal means that it is not possible to have a desquamating stratified squamous epithelium on the drum or the ear canal. If this were the case the desquamated cells would collect in the ear canal and lead to a build up of debris. The migratory nature of the epithelium avoids this problem. The squamous epithelium grows out radially across the surface of the drum until it reaches the annulus and then grows out laterally along the ear canal. The ceruminous glands, which produce the wax, are only located in the outer third of the ear canal. As a result, in a normal ear, the skin gradually migrates out towards the meatus taking excess wax with it. The normal ear is self-cleansing and the antiseptic, hydrophobic nature of wax keeps the medial end of the external ear canal relatively clean with only scanty growths of commensals present. Typically these are Staphylococcus epidermidis, Corynebacterium spp., Staphylococcus aureus, and Streptococcus viridans.
 4.1 Pre-auricular abscess in front of the pre-auricular pit (arrowed). |
 4.2 Infected sebaceous cyst. |
 4.3 Perichondritis secondary to otitis externa. |
FURUNCULOSIS
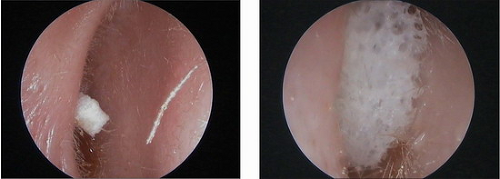
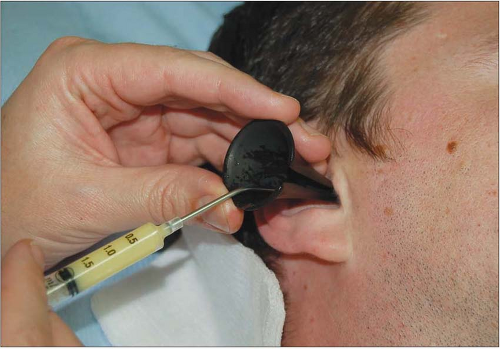
The outer third of the ear canal contains hair bearing skin and furunculosis is an infection of a hair follicle. It gives rise to a very tender localized swelling. Oedema in a confined area gives rise to severe pain. There may be little in the way of pus present. Infections are usually caused by Staphylo coccus aureus. The principle of treatment is to reduce the swelling in the ear canal using impregnated wicks. These are strips of ribbon gauze that can be soaked in topical agents. They need to be replaced or removed after 24-48 hours. For furunculosis, a wick soaked in ichthammol glycerin is the treatment of choice (4.4, 4.5). Wicks soaked with creams containing steroid and antibiotic may also be effective. Additional oral anti-staphylo coccal antibiotics are of value if there is erythema visible on the pinna. The swelling is caused by local oedema and very little pus and so surgical drainage is rarely effective.
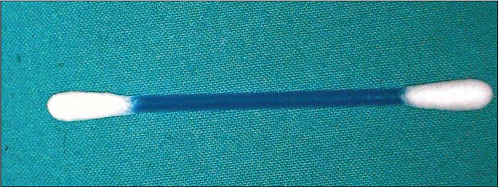
 4.4 Glycerine and ichthammol ribbon gauze wick. |
 4.5 Insertion of a wick. |
ACUTE OTITIS EXTERNA
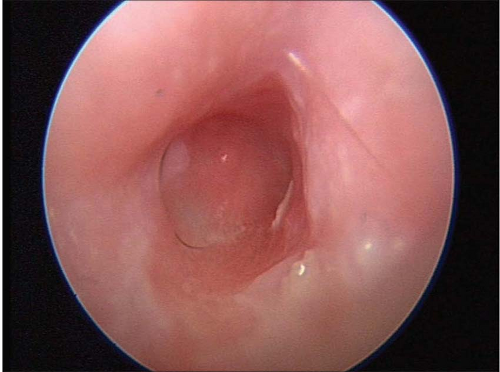
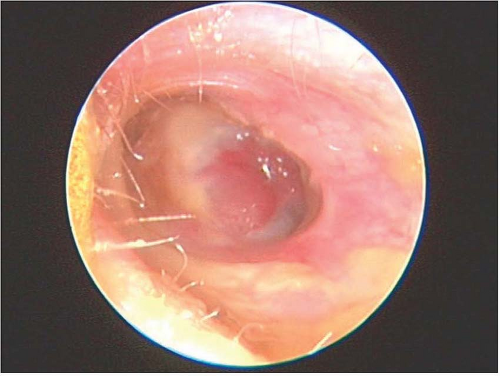
Acute infection of the ear canal presents as a painful ear which may be accompanied by a blocked feeling. Even gentle traction on the patient’s pinna exacerbates pain. In mild cases the ear canal will appear red and in more severe cases there will be acute oedema of the ear canal with narrowing of the meatus and a variable amount of debris in the canal. The aetiology of acute otitis externa may be idiopathic, traumatic due to scratching of the ear canal or injudicious use of cotton buds or related to water with an accompanying history of water getting into the ear as a result of swimming or syringing.
Treatment will vary depending on the degree of oedema. If the canal is inflamed and there is no evidence of debris, topical antibiotic drops or sprays containing broad-spectrum antibiotics and steroids may be all that is required (4.6). Cases where there is significant oedema will be very tender and will require gentle microsuction of any debris (4.7, 4.8). This is followed by the introduction of wicks to remove the oedema of the ear canal. These can be ribbon gauze wicks impregnated with ichthammol glycerin or steroid and antibiotic creams (4.9). Inserting a dessicated expandable ear wick followed by addition of a topical antibiotic drop preparation can also be effective (4.10,4.11 and 4.12). If the patient is toxic or there is associated erythema of the pinna or face then additional systemic antibiotics are required. In early acute otitis externa the infecting organisms are likely to be staphylococcal or streptococcal in nature, but with time the organisms soon change to those seen in chronic otitis externa.
As the ear responds to treatment, further suction clearance to clear the build up of any further debris may be necessary. Frequency of microsuction is highly variable. Wicks tend to dry out in 24-48 hours and therefore need to be changed every 24-48 hours. As the oedema settles, the ear canal widens and progressively longer/larger wicks can be inserted.
 4.6 Otitis externa with mild oedema and erythema but no debris. |
 4.7 Otitis externa with severe oedema and slit-like meatus. |
 4.8 Microsuction to remove debris in otitis externa. |
 4.9 Ribbon gauze soaked in combination steroid and antibiotic cream. |
 4.10 Dessicated expandable ear wick. |
CHRONIC OTITIS EXTERNA
Chronic otitis externa is as much an inflammatory as an infective process. The common reasons for persistence of the condition are:
Continuing trauma.
Secondary bacterial overgrowth: swabs taken from ears with chronic otitis externa will produce cultures of a large variety of pathogens. Pseudomonas spp. are the commonest, but Proteus spp., coliforms, and Staphylococcus aureus are frequently found in mixed growths.
Underlying skin conditions: eczema, seborrhoeic dermatitis, and psoriasis.
Chemical irritation: hair preparations and agents in antibiotic drops can become irritative.
Allergic reaction: the antibiotics in drops such as neomycin, gentamicin, and framycetin can induce a contact dermatitis with prolonged use. Hearing aid moulds and antiseptic dressing used after ear surgery can also cause allergic reactions (4.13, 4.14).
Environmental exposure to water or humid conditions.
 4.13 Erythema in the conchal bowl due to allergy to a hearing aid mould. |
 4.14 Weeping erythema due to allergy to bismuth iodoform paraffin paste (BIPP) dressing used after middle ear surgery. |
 4.15 Trauma to ear canal: cotton buds. |
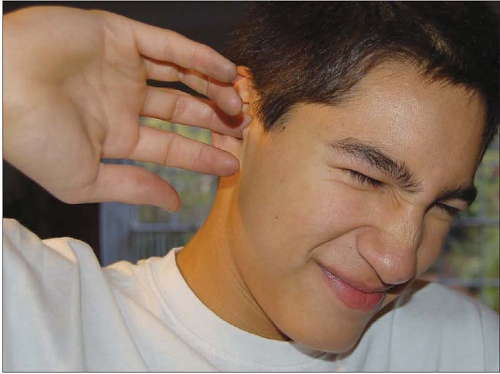
 4.16 Trauma to ear canal: finger nails. |
Although it may simply be a result of an acute otitis externa that is slow to resolve, in the majority of cases the failure of resolution is due to direct or indirect trauma (4.15,4.16 and 4.17). This condition is common in patients who have a tendency to eczema. The patient complains of an itching in the ear accompanied by variable amounts of discomfort and pain. The ear will tend to discharge and there will be a blocked feeling in the ear. In mild cases, the eczematous inflammation of the ear canal may be the only disease process (4.13). The inflamed skin loses its natural migratory ability and there is decreased wax production. There is a tendency for dry desquamated cells to collect in the ear canal. Treatment at this stage is gentle microsuction of any debris and use of steroid drops to settle the eczema and stop the itching.
Itching of the ear canal tempts the patient to use cotton buds, hair grips, pen tops, finger nails, and so on to rub or scratch the ear canal. A scratch inside the ear canal breaks the integumental layer of the skin and allows for infection to spread subcutaneously, giving rise to the classic appearance of a chronic infective otitis externa (4.18, 4.19, 4.20 and 4.21). The ear canal appears red with variable degrees of oedema and debris. The treatment is a ‘triple therapy’ approach as follows:
 4.17 Trauma to ear canal: rubbing. |
 4.18 Dry mildly eczematous ear canal with no wax. |
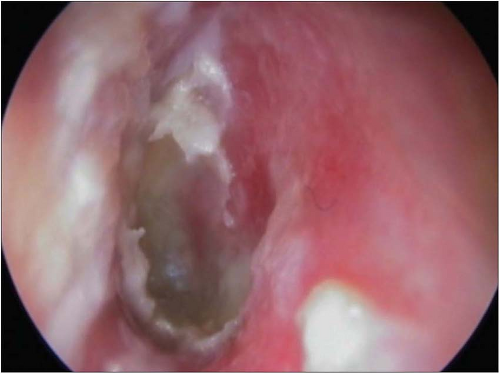 4.19 Chronic otitis externa: erythema, oedema, and debris. |
 4.20 Chronic otitis externa: erythema and oedema. |
 4.21 Chronic otitis externa: erythema, oedema and associated inflammation of the tympanic membrane (myringitis). |
Stop the patient rubbing, scratching, and poking the ear and keep the ear dry until the infection has settled.
Microsuction to remove the debris, which is a collection of desquamated skin cells, bacteria, and wax. This is likely to be required to be done repeatedly depending on the response to treatment.
Topical treatment using combinations of steroids and antibiotics. Milder cases will respond to simple drops and sprays, more severe cases benefit from insertion of steroid and antibiotic cream or ointment in the ear canal. Wicks can be used if there is significant oedema, but when the ear canal is reasonably open, insertion of cream or ointment into the ear canal using a 2 ml syringe with a plastic intravenous cannula attached is often easier (4.22). These treatments will often require to be repeated. Appearance of a normal ear canal with normal wax usually indicates that the problem has been solved. Oral antibiotics are rarely needed or helpful.
Patients will often complain of recurrent problems over many years. This is usually due to incomplete eradication of the initial infection. In chronic low-grade otitis externa it may be possible to gain control by using topical antiseptic solutions such as aluminium acetate or alcohol and acetic acid mixtures. These work by inhibiting bacterial growth by acidifying the ear canal.
 4.22 Filling the ear canal with combination steroid and antibiotic cream without a wick as treatment for chronic otitis externa.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|