This article presents disorders of periodic occurrence of laryngeal obstruction (POLO) resulting in noisy breathing and dyspnea and a variety of secondary symptoms. Included in this classification are glottic disorders, such as paradoxic vocal fold movement and vocal cord dysfunction. The supraglottic disorder, termed, intermittent arytenoid region prolapse or laryngomalacia , is also reviewed. Three categories of POLO are defined as irritant, exertional, and psychological.
A historical perspective
Periodic occurrence of laryngeal obstruction (POLO) was first described in an 1842 medical textbook by Dunglison, who noted a disorder of the laryngeal muscles in hysteric females that he termed, hysteric croup . In the textbook, Principles and Practice of Medicine, Austin Flint described a similar syndrome in two male adults and termed the condition, laryngismus stridulus . MacKenzie, however, reported the first evidence of abnormal vocal fold motion visualized by laryngoscopy in 1869. He noted paradoxic closure of the vocal folds with inspiration in hysteric patients. Sir William Osler, in the 1902 edition of The Principles and Practice of Medicine, further expanded on this syndrome as he described “spasm of the muscles may occur with violent inspiratory efforts and great distress, and may even lead to cyanosis . . . Extraordinary cries may be produced, either inspiratory or expiratory.” Little additional information was published until the 1970s when Patterson and colleagues described a 33-year-old woman with 15 hospital admissions for what they named, Munchausen’s stridor . Since then, more than 70 different terms have been coined over the past 30 years to describe abnormal movement of the true vocal folds. Many of these terms have been used primarily to describe abnormal vocal fold movement in the absence of other medical diseases ( Table 1 ).
| Term | Author | Year |
|---|---|---|
| Munchausen’s stridor | Patterson R | 1974 |
| Pseudoasthma | Dailey RH | 1976 |
| Nonorganic upper airway obstruction | Cormier YF | 1980 |
| Functional upper airway obstruction | Appelblatt NH | 1981 |
| Factitious asthma | Downing ET | 1982 |
| Vocal cord dysfunction | Christopher KL | 1983 |
| Spasmodic croup | Collett PW | 1983 |
| Emotional laryngeal wheezing | Rodenstein DO | 1983 |
| Psychogenic upper airway obstruction | Barnes SD | 1986 |
| Episodic laryngeal dyskinesia | Ramirez JR | 1986 |
| Exercise-induced laryngospasm | Liistro G | 1990 |
| Functional laryngeal obstruction | Pitchenik AE | 1991 |
| Psychogenic stridor | Lund DS | 1993 |
| Functional laryngeal stridor | Smith ME | 1993 |
| Episodic paroxysmal laryngospasm | Gallivan GJ | 1996 |
| Irritable larynx syndrome | Morrison M | 1999 |
| Paradoxic vocal fold motion | Patel NJ | 2004 |
There are several proposals to categorize VCD more fully and essentially classify all glottic movement disorders into one definition. Andrianopoulos and colleagues equated paradoxic vocal fold motion, paroxysmal VCD, episodic paroxysmal laryngospasm, and irritable larynx syndrome as the same entity. A distinction was made between differing associated causes, such as gastroesophageal reflux disease, primary dystonias, psychogenic causes, and disorders of central nervous system affecting the vocal folds. The use of the term, irritable larynx syndrome , by Morrison and colleagues proposed a unifying hypothesis of VCD and laryngospasm in the presence of a sensory trigger. This definition, however, eliminates an identifiable psychiatric diagnosis as the cause. Additionally, the hypothesis of solely an irritable or hyperresponsive state is contrary to recent data demonstrating reduced laryngeal irritability with sensory stimuli in the presence of laryngopharyngeal reflux. It is apparent that neither of these classifications adequately describes the full-spectrum episodes of laryngeal dysfunction.
The two terms most frequently encountered in the literature and used extensively in clinical practice are paradoxic vocal fold motion (PVFM) and vocal cord dysfunction (VCD) (discussed later). PVFM is most likely to be selected by otolaryngologists and speech pathologists. In contrast, pulmonologists, allergists, psychiatrists, and psychologists are generally drawn to VCD. Do these terms represent exactly the same disorder with one common origin? Are different terms used simply because of different specialty educational paths? Alternatively, is the endoscope used to visualize a limited number of end-organ laryngeal responses without fully understanding a spectrum of causes that are literally hidden from sight? Addressing these and other important issues calls for an interdisciplinary team approach. Scientists prefer to answer the questions by being “splitters” rather than “lumpers.” It may be beneficial, however, to engage in a two-step process: first lumping, then splitting.
Focusing on the big picture
A reasonable first step might be to lump VCD, PVFM, and other similarly presenting disorders into an umbrella classification based on the presence of POLO. Inclusion would be based on unifying chief complaints resulting from episodes of laryngeal obstruction, endoscopic findings, and general commonalities in the characteristics of the clinical presentation. Speculation regarding specific cause would likely bog down the process of classification at this level, and the authors recommend that the issue is best addressed at the second step, the splitting stage. That general grouping, as outlined, may improve understanding of what should be “in the box.” As a wise colleague once stated, “…if you don’t think about it, you can’t diagnose it.” Similarly, grouping should not be overly inclusive. Thinking too much “out of the box” and pulling in diseases and disorders that do not fit will keep involved clinicians in Babylon, perpetually mumbling about disjointed terms and concepts. As with the splitting second step, the umbrella level of the classification system should be dynamic—changing as the collaborative knowledge base expands.
To get the process off the ground, the authors propose that VCD, PVFM, and intermittent arytenoid region prolapse (IARP) have clinical similarities and can be justifiably lumped into an umbrella classification. The authors have selected the term, IARP , rather than laryngomalacia based on the observations of Bittleman. The term, laryngomalacia , was avoided due to potential confusion with the neonate and infant population with presumed congenital abnormalities.
The authors conclude that VCD, PVFM, and IARP can be lumped into a classification of POLO manifested by chief complaints of noisy breathing and dyspnea. Secondary symptoms including, but not limited to, cough, chest tightness, throat tightness, and changes in voice may be present. Limitations of current diagnostic technology (eg, pulmonary function testing and diagnostic radiology) make endoscopic examination the gold standard for documenting the presence and characteristics of the laryngeal obstruction. A fixed obstructive airway lesion should be excluded. One or more recurring precipitating factors are usually identifiable by history; interrelationships between multiple precipitating factors in a given patient can be perplexing. Patients are predominately, but not exclusively, female; adolescent and young adult age groups seem to be predisposed. Periodic symptoms have often occurred over many months to years, and complaints have been refractory to prior prescribed medical therapy (eg, asthma medications and hyposensitization). During a symptomatic period, a patient’s noisy breathing is usually reported on physical examination as “stridor” or “wheeze” (which may not be accurate). Physical examination documentation is often sparse regarding how stridor or wheeze relates to the breathing cycle. Close attention by experienced ears frequently raises suspicion that the noisy breathing is generated at the level of the larynx. Patients may present across the spectrum from appearing to be in extremis during an episode; alternatively, they may have complaints out of proportion to objective findings. Because repetitive episodes are characteristically transient or self-limiting in nature, acute symptoms and physical examination findings should resolve when the POLO resolves. Endoscopy during an asymptomatic period usually assists by confirming the periodic nature of the laryngeal obstruction. Similarly, a more complete and comprehensive endoscopic examination can be performed when patients are asymptomatic, facilitating exclusion of some disorders that otherwise are in the differential diagnosis. Additionally, identification of more subtle endoscopic findings (eg, consistent with gastroesophageal reflux disease, laryngopharyngeal reflux, and rhinogenic disorders) can facilitate the transition to the second phase (the splitting phase) where specific causes and associated disorders can be pursued.
The features (discussed previously) are generally characteristic among the three entities in the umbrella classification. POLO can be at the level of the glottis, supraglottic area, or both. Glottic disorders in this proposed POLO classification are VCD and PVFM. IARP is presented as a supraglottic disorder.
Focusing on the big picture
A reasonable first step might be to lump VCD, PVFM, and other similarly presenting disorders into an umbrella classification based on the presence of POLO. Inclusion would be based on unifying chief complaints resulting from episodes of laryngeal obstruction, endoscopic findings, and general commonalities in the characteristics of the clinical presentation. Speculation regarding specific cause would likely bog down the process of classification at this level, and the authors recommend that the issue is best addressed at the second step, the splitting stage. That general grouping, as outlined, may improve understanding of what should be “in the box.” As a wise colleague once stated, “…if you don’t think about it, you can’t diagnose it.” Similarly, grouping should not be overly inclusive. Thinking too much “out of the box” and pulling in diseases and disorders that do not fit will keep involved clinicians in Babylon, perpetually mumbling about disjointed terms and concepts. As with the splitting second step, the umbrella level of the classification system should be dynamic—changing as the collaborative knowledge base expands.
To get the process off the ground, the authors propose that VCD, PVFM, and intermittent arytenoid region prolapse (IARP) have clinical similarities and can be justifiably lumped into an umbrella classification. The authors have selected the term, IARP , rather than laryngomalacia based on the observations of Bittleman. The term, laryngomalacia , was avoided due to potential confusion with the neonate and infant population with presumed congenital abnormalities.
The authors conclude that VCD, PVFM, and IARP can be lumped into a classification of POLO manifested by chief complaints of noisy breathing and dyspnea. Secondary symptoms including, but not limited to, cough, chest tightness, throat tightness, and changes in voice may be present. Limitations of current diagnostic technology (eg, pulmonary function testing and diagnostic radiology) make endoscopic examination the gold standard for documenting the presence and characteristics of the laryngeal obstruction. A fixed obstructive airway lesion should be excluded. One or more recurring precipitating factors are usually identifiable by history; interrelationships between multiple precipitating factors in a given patient can be perplexing. Patients are predominately, but not exclusively, female; adolescent and young adult age groups seem to be predisposed. Periodic symptoms have often occurred over many months to years, and complaints have been refractory to prior prescribed medical therapy (eg, asthma medications and hyposensitization). During a symptomatic period, a patient’s noisy breathing is usually reported on physical examination as “stridor” or “wheeze” (which may not be accurate). Physical examination documentation is often sparse regarding how stridor or wheeze relates to the breathing cycle. Close attention by experienced ears frequently raises suspicion that the noisy breathing is generated at the level of the larynx. Patients may present across the spectrum from appearing to be in extremis during an episode; alternatively, they may have complaints out of proportion to objective findings. Because repetitive episodes are characteristically transient or self-limiting in nature, acute symptoms and physical examination findings should resolve when the POLO resolves. Endoscopy during an asymptomatic period usually assists by confirming the periodic nature of the laryngeal obstruction. Similarly, a more complete and comprehensive endoscopic examination can be performed when patients are asymptomatic, facilitating exclusion of some disorders that otherwise are in the differential diagnosis. Additionally, identification of more subtle endoscopic findings (eg, consistent with gastroesophageal reflux disease, laryngopharyngeal reflux, and rhinogenic disorders) can facilitate the transition to the second phase (the splitting phase) where specific causes and associated disorders can be pursued.
The features (discussed previously) are generally characteristic among the three entities in the umbrella classification. POLO can be at the level of the glottis, supraglottic area, or both. Glottic disorders in this proposed POLO classification are VCD and PVFM. IARP is presented as a supraglottic disorder.
What diagnoses are in the differential?
Any pulmonary disorder that presents with periodic noisy breathing, dyspnea, and secondary complaints, such as cough, could be considered in the differential diagnosis. Asthma has historically been at the top of the list. Chevalier Jackson’s axiom is often quoted : “not all that wheezes is asthma.” Even after his death in 1958, the hunt for asthma masqueraders marches onward. Today, use of the statement that “all that wheezes is not POLO” is avoided; however, VCD, PVFM, and IARP should rank somewhere below asthma in the differential diagnosis for dyspnea and wheezing, particularly with regard to similarities to asthma in clinical presentation.
It is recognized by the pulmonary and allergy communities that too many patients are diagnosed with asthma without objective lung function testing by spirometry. Unfortunately, this can be a double-edged sword. Under specific circumstances, pulmonary diagnostic tools may confuse more than assist in excluding asthma; this can occur initially or when evaluating for coexistent disease after one of the POLO disorders is confirmed. These pitfalls are discussed later.
There are laryngotracheal mass lesions that may occasionally appear to be episodic at some point in their clinical course, but the obstruction does not resolve. As the progressive disease increases to critical airway occlusion, patients may experience cyclic increases in dyspnea and noisy breathing. For example, they may be in greater distress due to exertion, increased ventilatory requirements from any cause (eg, pneumonia), and airway inflammation. Cessation of exertion, reduction in ventilatory requirement, and treated airway infection or systemic disease flair (eg, relapsing polychondritis) may transiently improve symptoms. It is well recognized that airway-obstructing lesions may be benign by histology but malignant by course. An entity that requires special mention is idiopathic laryngotracheal stenosis, particularly because of its predilection, as with POLO disorders, for young- to middle-aged women and similar presentation with exertional dyspnea and noisy breathing.
Important categories of laryngeal manifestations of diseases and disorders that should be considered in the differential diagnosis are illustrated in Table 2 . The categories of neurogenic, vocal fold paresis and paralysis, and laryngospasm have different characteristics, presentations, and endoscopic findings from the POLO disorders. There are a variety of entities within each category. The conditions listed in Table 2 are discussed in articles elsewhere in this issue.
| Disorder | Examples of Conditions |
|---|---|
| Neurogenic | Brainstem compression Upper motor neuron injury Lower motor neuron injury Movement disorders Adductor laryngeal breathing dystonia |
| Vocal fold paralysis | Head and neck malignancy Chest surgery Idiopathic |
| Vocal fold paresis | Prolonged intubation |
| Laryngospasm | Intubation Airway manipulation Immunoglobulin E mediated Nocturnal aspiration |
How do we address cough?
As discussed previously, cough is a complaint in the overall POLO population. Unfortunately, the literature has been inherently limited by a paucity of adequate studies. Lack of agreement on terms and concepts, absence of a structured scientific approach, and small sample sizes have made clinical investigation difficult. The authors’ recent literature review (Morris MJ, MD and Christopher KL, MD, unpublished data, 2009), however, can offer insight regarding the overall prevalence of reported cough in the POLO population. Data are likely to be conservative as cough may have been present but not reported in the respective articles.
A total of 355 articles was reviewed (Morris MJ, MD and Christopher KL, MD, unpublished data, 2009); 67 articles were excluded that contained duplicate data or discussed laryngospasm, vocal cord paresis or paralysis, primary neurologic syndromes, or other glottic disorders that were not consistent with POLO. The final series of articles (n = 288) concerning POLO included 159 case reports, 37 retrospective studies, 21 prospective studies, 74 review articles, and 18 letters to the editor or editorials. In the few reports and collectively small numbers of patients with IARP, symptoms other than dyspnea and noisy breathing were not common; cough was rarely described. The review found symptoms (Morris MJ, MD and Christopher KL, MD, unpublished data, 2009) were reported in 1020 patients with VCD (64% of total); symptoms were chronic in 860 patients (85%) and acute in 151 patients (15%). Dyspnea was the predominant symptom in 73% of patients followed by wheeze (36%) and stridor (28%), with collective noisy breathing at 64%. Less common symptoms included cough (25%), chest tightness (25%), throat tightness (22%), and changes in voice (12%).
More than 3 years ago, Brugman reviewed the symptoms of patients identified as having VCD from the published literature and noted a higher prevalence of symptoms. Dyspnea (95%), wheeze (51%), stridor (51%), and cough (42%) were the predominant findings. In summary, with shortfalls of literature review in mind, in 85% of patients with VCD, symptoms were chronic, and cough was reported in 25%. In an earlier review of what could have been a slightly different population, cough was present in 42%. It would be reasonable to conclude that the conservative prevalence of cough is in the range of 25% to 42%. Further light may be shed on cough as the three POLO entities are split in terms of how they differ from each other.
Differences among periodic occurrence of laryngeal obstruction disorders
POLO disorders can be placed into the three separate categories ( Table 3 ). Furthermore, each of the three categories (psychogenic, exertional, and irritant) is composed of several entities. The irritant category is subdivided into extrinsic and intrinsic conditions.
| Category | Conditions |
|---|---|
| Irritant |
|
| Exertional |
|
| Psychological |
|
Because most agree that endoscopy is the diagnostic study of choice (Morris MJ, MD and Christopher KL, MD, unpublished data, 2009) for identifying POLO, how do descriptions differ between VCV, PVFM, and IARP? That information may assist in sorting out the three categories and their subcomponents in the future.
Endoscopic evaluation
Although characteristic endoscopic findings are discussed, it is difficult to determine relative frequency, as the literature review (Morris MJ, MD and Christopher KL, MD, unpublished data, 2009) demonstrates that endoscopy was not performed in 38% of patients. Inspiratory adduction was reported in 32% of those articles that described endoscopic findings. Descriptions were usually just the acknowledgment of “paradoxical vocal fold movement” or “vocal cord dysfunction” or referred to acronyms. Respiratory phase of the obstruction was frequently undefined (inspiratory, expiratory, or both). If inspiratory obstruction was noted (eg, PVFM), there was usually no statement as to whether or not expiratory findings were entirely normal.
The presence of inspiratory adduction is key to the diagnoses of PVFM and VCD. Additionally, concomitant expiratory obstruction can be seen in VCD. Inspiratory supraglottic obstruction is the major finding in IARP. For the purpose of this article, an overall concept of characteristic findings is constructed, drawing attention to key references when possible, and putting laryngoscopic findings in perspective based on the authors’ experiences.
For the long term, development of an interdisciplinary POLO endoscopic classification system integrating various clinical experiences (otolaryngology, pulmonary, allergy, and speech pathology) would be a worthwhile pursuit. Defined protocols and uniform descriptors and integration of additional endoscopic testing (eg, stroboscopy and exercise laryngoscopy) may facilitate the process of targeting POLO categories, conditions (see Table 3 ), and exclusions in the differential diagnosis (see Table 2 ).
Primary care clinicians must become better educated regarding the importance of flexible laryngoscopic examination in patients with suspected laryngeal disease. They need to be aware that, as with any procedure, trained professionals should perform flexible laryngoscopy. Additionally, flexible laryngoscopy is well tolerated with minimal risk when performed properly.
As discussed previously, the endoscopic examination of POLO subjects is frequently normal when patients are symptom-free. Patient maneuvers (eg, sniff and established phonatory tasks) performed during routine examination may confirm normal abductor and adductor function and voice, thus facilitating exclusion of some disorders listed in Table 2 . A forced expiratory vital capacity maneuver followed by a forced inspiratory vital capacity maneuver simulates generation of a flow-volume loop (FVL) and may be helpful. Pulmonary function and provocation testing are discussed later.
Ancillary endoscopic findings suggestive of a condition in the irritant category (see Table 3 ) are discussed in articles elsewhere in this issue. There still is much to learn about the origins in many conditions within each of the three POLO categories. A patient may present with conditions in more than one category. Co-existent but unrelated disorders must be objectively differentiated, and additional information in the presence of nonspecific endoscopic findings must be sought. The psychological category is the great imitator of conditions in the other two categories and is discussed.
What degree of obstruction is required with PVFM, VCD, or IARP? The critical obstruction (percent obstruction) required to produce symptoms in fixed obstructive lesions in a variety of “tubes” (eg, trachea and carotid artery) is easier to predict. Variable airway obstructions are more difficult to assess and depend on their timing relative to the breathing cycle. Inspiratory and expiratory glottic or supraglottic dynamic obstruction affects work of breathing and respiratory physiology in different ways.
Paradoxic vocal fold motion
In PVFM, the true vocal folds do not abduct in a normal fashion during inspiration. The true vocal folds paradoxically and symmetrically adduct toward the midline during inspiration, producing glottic obstruction. In those individuals with an isolated inspiratory abnormality, the endoscopic characterization is appropriate. PVFM, however, does not adequately describe glottic obstruction that also occurs on exhalation, as the true vocal folds normally adduct to some degree during quiet breathing. Abnormal expiratory adduction is not truly paradoxic because movement is not in the opposite direction of normal.
The PVFM on inspiration first described in hysteric patients in 1869 by MacKenzie was a major finding. Furthermore, Osler added clinical insight by documenting that noisy breathing (“extraordinary cries”) and dyspnea (“great distress”) could be on inspiration and expiration. The term PVFM does not encompass POLO disorders that also occur on exhalation. Taken at face value, PVFM is a straightforward and literal endoscopic descriptor; however, its use usually implies additional meaning to an examiner. A significant problem arises when endoscopic diagnoses, such as PVFM and VCD, are bantered about in a cavalier fashion.
Vocal cord dysfunction
The comments made regarding the term PVFM should be underscored and amplified when discussing VCD. Similarly, taken at face value, VCD is the most endoscopically nondescript term in the POLO classification. When looking at the original description of VCD, however, it is defined in the context of a disorder presenting as asthma and defines more than one specific endoscopic abnormality. One author of this article (KLC) was the team leader and pulmonologist for the interdisciplinary team in that publication ; the team included an otolaryngologist, speech pathologist, pulmonary physiologist, and psychiatrist.
Clinical presentation and other diagnostic testing are discussed later. Endoscopic findings are shown in Fig. 1 . All subjects had normal laryngeal function and anatomy when laryngoscopy was performed during an asymptomatic period (see Fig. 1 A). During a typical episode (see Fig. 1 B) of complaints of dyspnea and noisy breathing, each had almost complete adduction of the true vocal folds; the glottis narrowed to a small posterior diamond-shaped chink. The false vocal folds bunched together, obscuring visualization of the laryngeal ventricles. The arytenoids tended to be maintained at a lateral position with failure to adduct. These abnormalities were seen on inspiration (see Fig. 1 B) and expiration (see Fig. 1 C.) The moderate expiratory obstruction (see Fig. 1 C) is contrasted to more severe expiratory obstruction (see Fig. 1 D).
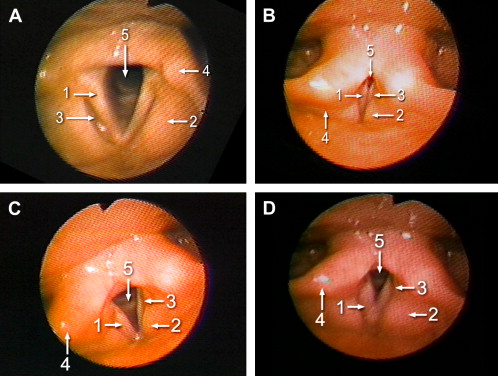
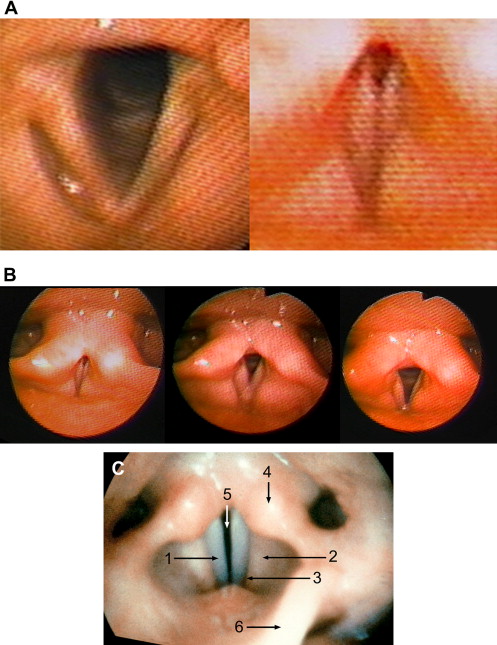
Fig. 2 A shows a side-by-side view of the inspiratory glottic aperture under asymptomatic conditions (see Fig. 1 A) and during symptoms (see Fig. 1 B). Similarly, Fig. 2 B illustrates a composite view from left to right comparing the inspiratory glottic aperture during symptoms (see Fig. 1 B), a pronounced expiratory reduction in glottic area (see Fig. 1 D), and a more moderate reduction in expiratory glottic aperture (see Fig. 1 C). Photographs were cropped similarly and then sized to approximately the same anteroposterior length at the level of the glottic opening. The approximate comparison provides a relative understanding of the magnitude of inspiratory and expiratory obstruction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


