Purpose
To describe the pathogenesis, clinical characteristics, management, and outcomes of patients in whom vitreomacular traction evolved pursuant to treatment of choroidal melanoma with transpupillary thermotherapy.
Design
Retrospective, uncontrolled, observational, interventional case series.
Methods
Vitreomacular traction with macular distortion, macular edema, and vision loss developed in 6 eyes of 6 patients after successful transpupillary thermotherapy for choroidal melanoma. Clinical examination, fluorescein angiography, fundus photography, and spectral-domain optical coherence tomography were performed. Symptomatic patients underwent pars plana vitrectomy (PPV). Primary outcome measures include visual acuity and resolution of macular distortion by clinical examination, spectral-domain optical coherence tomography, or both.
Results
In all 6 patients, the malignant lesions were treated successfully. The posterior hyaloid was attached in all eyes before transpupillary thermotherapy. All eyes demonstrated focal hyaloidal contraction and vitreomacular traction between the transpupillary thermotherapy scar and the macula. Mean time from transpupillary thermotherapy to PPV for treatment of vitreomacular traction was 23 ± 18 months. Mean length of follow-up was 11 months. Mean logarithm of the minimal angle of resolution visual acuity before transpupillary thermotherapy was 0.23 ± 0.38. Mean visual acuity after transpupillary thermotherapy was 0.53 ± 0.42. Mean visual acuity before membrane peel was 0.65 ± 0.34. Mean visual acuity after membrane peel was 0.44 ± 0.21. All patients undergoing PPV showed visual improvement.
Conclusions
Hyaloidal contraction can occur after transpupillary thermotherapy and is a reversible cause of vision loss. The mechanism of vision loss resulting from hyaloidal contraction is flat vitreomacular traction. PPV and membrane peeling are effective in improving macular anatomic features and visual function.
Vitreomacular traction has been recognized and documented in many different forms since Jaffe first described it in 1967. In the most common form, vitreomacular traction is the result of separation of the vitreous from the peripheral retina, but not the posterior pole. Persistence of posterior hyaloidal attachment may be focal, multifocal, or broad. The anatomic consequences of the various types of hyaloidal attachment include focal retinal cavitation, retinal distortion, diffuse cystoid macular edema, or a combination thereof. Johnson described a series of patients with a subtle and unusual form of focal vitreomacular traction at the fovea resulting in tractional cystoid macular edema. The most widely accepted cause of vitreomacular traction is thought to be partial posterior vitreous detachment. The resulting vision loss is at least partly reversible with either spontaneous or surgical release of the traction.
Posterior hyaloidal contraction is a special case of vitreomacular traction in which traction occurs along an expanse of attached posterior hyaloid, with the hyaloid broadly or completely attached. Posterior hyaloidal contraction occurs in a number of clinical conditions, including diabetes (some cases of diabetic macular edema, as well as proliferative diabetic retinopathy), proliferative vitreoretinopathy, and in pediatric vasoproliferative disorders such as retinopathy of prematurity and familial exudative vitreoretinopathy, among others. Anteroposterior traction has little role in posterior hyaloidal contraction because of the lack of posterior vitreous detachment in the peripheral retina. More likely, tractional forces in posterior hyaloidal contraction occur as a consequence of cellular proliferation along the hyaloidal surface or within the posterior hyaloidal cortex with subsequent contraction. Herein, we describe hyaloidal contraction after transpupillary thermotherapy for presumed choroidal malignant melanoma in the posterior pole.
Methods
Setting
This is a retrospective, uncontrolled, observational, interventional case series of consecutive patients in whom symptomatic metamorphopsia, vision loss, or both developed after transpupillary thermotherapy treatment. The study was conducted at a large tertiary referral vitreoretinal practice. Institutional review board approval for a retrospective chart review was obtained from Western Institutional Review Board, Olympia, Washington, USA. Medical records and images were reviewed with institutional review board approval and in accordance with the Health Insurance Portability and Accountability Act of 1996. This study adhered to the conventions of the Declaration of Helsinki and all relevant state and federal laws. Collectively, the cohort of patients were examined and treated between 2003 and 2012.
Study Population
The clinical database of a tertiary vitreoretinal referral service was searched by billing codes for patients with choroidal melanoma, vitreomacular traction, and epiretinal membrane (Ophthalmology Evaluation and Management Codes 190.6, 379.27, and 362.56, respectively). All patients underwent slit-lamp biomicroscopy, indirect ophthalmoscopy, fluorescein angiography, fundus photography, and B-scan ultrasonography at baseline for evaluation of choroidal melanoma. Clinical examination included slit-lamp examination using a 90-diopter or 78-diopter indirect lens. Subsequent examinations were performed at the discretion of the examining physician and with 1 or more of the imaging methods described. Epiretinal membrane was defined as the cellophane appearance of the macula that usually was accompanied by distortion of the macular vessels and retina. Vitreomacular traction resulting from posterior hyaloidal contraction was diagnosed by the presence of opacified hyaloid or vitreous condensation overlying an area of retina with underlying distortion of vessels or retinal tissue.
Intervention
Transpupillary thermotherapy was performed using a diode laser (IRIS Medical Oculight; Iridex Corp, Mountain View, California, USA) with settings adjusted to obtain bright white spots on the target lesion. Usually these settings were as follows: spot size, 1800 μm; duration, 40 to 60 seconds; and power, 1 W. Settings were adjusted based on the lesion size, fundus pigmentation, and lesion pigmentation. As many applications as necessary were made to cover the entire lesion and a 100- to 200-μm margin around the lesion. Pars plana vitrectomy (PPV) was performed using a 23- or 25-gauge vitrectomy system (Alcon Constellation Systems; Alcon, Fort Worth, Texas, USA) with or without use of adjunct procedures, including indocyanine green for internal limiting membrane peeling, fluid–air exchange, air–gas exchange, and intravitreal triamcinolone injection. The decision for surgical intervention was based on clinical presentation, including progressive vision loss and distortion of macular architecture on clinical examination and optical coherence tomography.
Outcome Measures
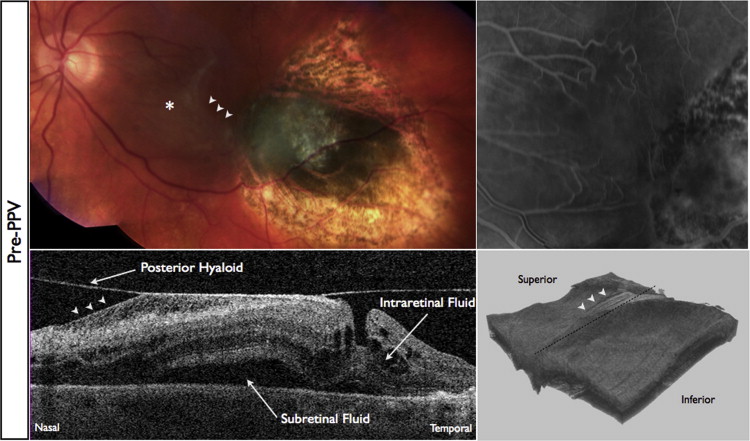
Spectral-domain optical coherence tomography (SD OCT) was performed through a dilated pupil by a certified ophthalmic photographer using the commercially available Cirrus SD OCT (Carl Zeiss Meditec, Dublin, California, USA). The SD OCT study was a standard high-density volume scan of the macula in a 6 × 6-mm area centered on the fovea. In some cases, high-volume scans of the peripheral macula or retina were obtained to visualize the anatomic features at the boundary of the transpupillary thermotherapy site and normal retina, to visualize the presence of subretinal fluid, and to visualize the overlying hyaloid. Three-dimensional reconstructions of the volume scans were performed with commercially available reconstruction software available with the Cirrus device.
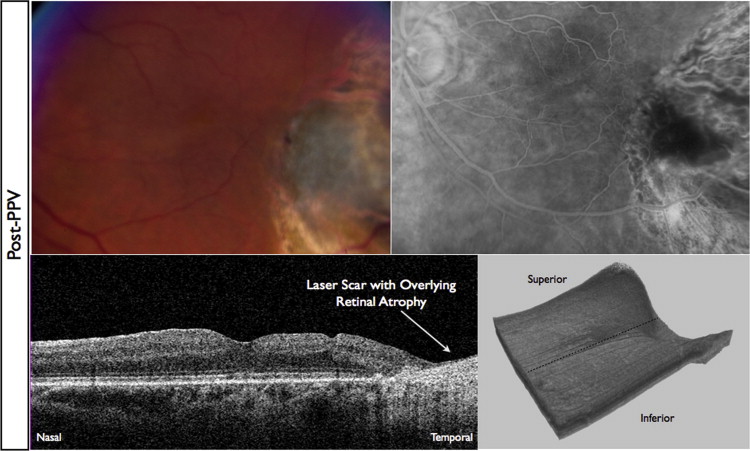
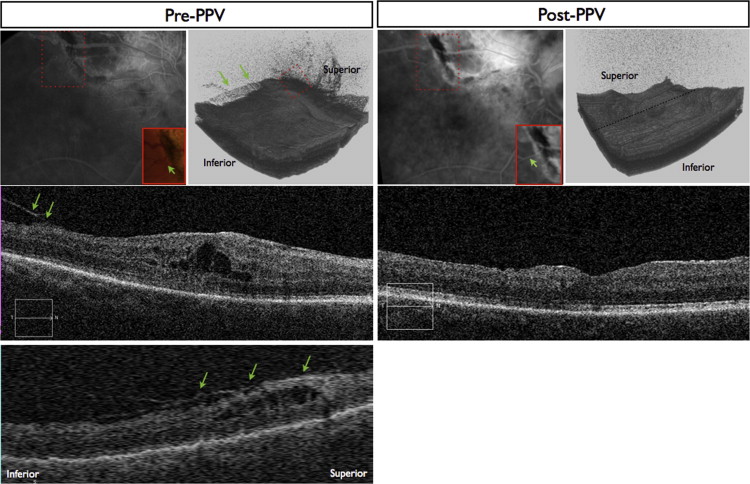
Hyaloidal contraction was identified on SD OCT as a hyperreflective layer that was evident slightly anterior to or confluent with the vitreoretinal interface on single line scans or a 3-dimensional hyperreflective sheet anterior to the retinal surface on 3-dimensional volume reconstruction. The identification of hyaloidal contraction was most evident on 3-dimensional reconstructions of the volume scan. Epiretinal membranes were identified as a hyperreflective feature located at the vitreoretinal interface and were most evident on individual line scans. Figures 1, 2, 3, and 4 illustrate these findings. Measurements of central subfield thickness and retinal volume also were obtained from the automated algorithms provided on the Cirrus device.
For statistical analysis, Snellen visual acuity was converted to a logarithmic scale (logarithm of the minimal angle of resolution) for each examination. Baseline examination was defined as the examination immediately before transpupillary thermotherapy therapy was instituted. The primary outcome was improvement of visual acuity. The secondary outcome was anatomic resolution of hyaloidal contraction by SD OCT. Statistical significance was determined using the paired Student t test where indicated.
Results
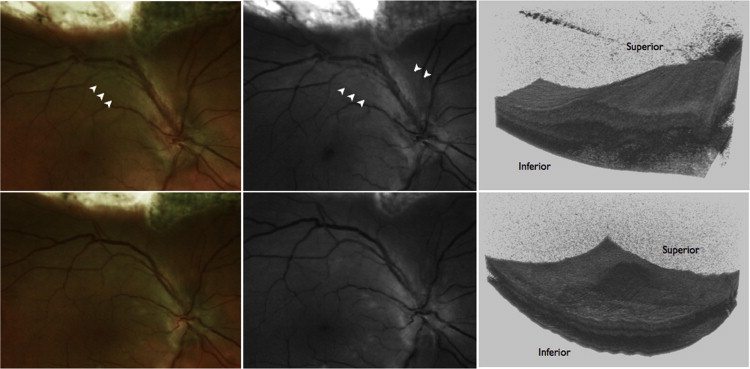
A total of 11 patients with small choroidal melanoma who had undergone transpupillary thermotherapy were identified in the database. Five of these 11 patients had posterior vitreous detachment at the time of transpupillary thermotherapy treatment and therefore were excluded from the results because there was no possibility of vitreomacular traction formation. The results of the remaining 6 patients without posterior vitreous detachment are reported here. All 6 of the patients without posterior vitreous detachment demonstrated vitreomacular traction after transpupillary thermotherapy. The Table summarizes the patient data. The mean patient age was 64 ± 9 years (range, 45 to 75 years). All choroidal lesions treated with transpupillary thermotherapy were located posterior to the equator. Of the 6 patients in the cohort, none (0%) had clinically evident or symptomatic vitreomacular traction before transpupillary thermotherapy. All patients (100%) demonstrated clinically significant vitreomacular traction resulting from posterior hyaloidal contraction after transpupillary thermotherapy. The etiology of visual loss was posterior hyaloidal contraction resulting in vitreomacular traction between 4 and 51 months after transpupillary thermotherapy treatment. Clinical examination in these patients demonstrated vitreous condensation overlying parts or all of the transpupillary thermotherapy lesion and extending toward the macular region. Figures 1, 2, 3, 4, and 5 illustrate 3 clinical examples of the vitreomacular traction resulting from hyaloidal contraction. Fluorescein angiography confirmed normal macular perfusion in all patients after transpupillary thermotherapy.



