Purpose
To evaluate the effect of vitrectomy timing on outcomes for patients with crystalline retained lens fragments receiving vitrectomy 3+ days after cataract surgery.
Design
Systematic review and meta-analysis of retrospective interventional cases series.
Methods
Searches of MEDLINE (English, 1/1/85 through 7/30/2010) and article reference lists. Articles were screened for patients with crystalline retained lens fragments after surgery for age-related cataracts, discussion of vitrectomy timing, and, for the meta-analysis, patient totals for at least 1 outcome and multiple time periods, 10+ patients, and mean follow-up ≥3 months. Outcomes included visual acuity, retinal detachment, increased intraocular pressure, intraocular infection/inflammation, cystoid macular edema, and corneal edema. Data extraction was performed twice and quality assessed. Logistic regression estimated study-level odds ratios for each additional 1-week vitrectomy delay. Meta-analysis estimated summary odds ratios using random-effects models.
Results
Of 257 articles identified, there were 43 unique studies (53 articles) for the systematic review, including 27 (31 articles) for the meta-analysis. Early vitrectomies were statistically significantly associated with better outcomes for not good visual acuity (odds ratio: 1.13; 95% CI: 1.04–1.22, P = .005); bad visual acuity (odds ratio: 1.05; 95% CI: 1.01–1.09, P = .009); previtrectomy retinal detachment (odds ratio: 1.29; 95% CI: 1.01–1.65, P = .038); postvitrectomy retinal detachment (odds ratio: 1.13; 95% CI: 1.02–1.26, P = .024); increased intraocular pressure (odds ratio: 1.23; 95% CI: 1.07–1.41, P = .003); and intraocular infection/inflammation (odds ratio: 1.20; 95% CI: 1.01–1.42, P = .041). Results were robust to sensitivity analyses.
Conclusions
This systematic review and meta-analysis found significantly better outcomes (visual acuity, retinal detachment, increased intraocular pressure, intraocular infection/inflammation) with earlier vitrectomy for retained lens fragments. Reduced vitrectomy delays may yield better patient outcomes.
Intravitreal retained lens fragments, with an incidence rate between 0.1% and 1.6%, are a rare but potentially serious complication of cataract surgery, which can result in poor visual acuity (VA) and other serious ocular complications. Patients are often referred to a vitreoretinal surgeon for treatment, usually including a pars plana vitrectomy (PPV) to improve visual acuity and reduce intraocular inflammation and pressure, but some are treated medically. Optimal vitrectomy timing is unknown, and the effect of timing on outcomes is controversial. Some favor early vitrectomy within a week or two of, or even the same day as, cataract surgery. Others prefer to wait and see, performing an early PPV only when clinically indicated—for example, if the patient had increased intraocular pressure (IOP) unresponsive to medication and/or a severe inflammatory response. However, many avoid the first few days after cataract surgery to permit the eye to recover.
The literature contains mixed results: some studies show statistically significant results indicating early vitrectomy leads to better outcomes, while other studies do not, but many show a nonsignificant trend favoring early vitrectomy. In addition, it is likely that selection bias has confounded these results, since patients with more serious ocular complications were more likely to receive an early vitrectomy. If meta-analysis indicated that outcomes were better with early vitrectomy, despite selection bias favoring later vitrectomy, a hypothesis that early vitrectomy might result in better outcomes seems reasonable.
Most studies reported visual acuity results in 3 categories: good VA (≥/> 0.5 or 20/40), moderate VA (0.5–0.1 or 20/40 to 20/200), and bad VA (≤/< 0.1 or 20/200). Retinal detachment (RD), IOP/glaucoma, intraocular inflammation/infection, cystoid macular edema (CME), and corneal edema are ocular complications of retained lens fragments that often result in visual loss. These were the outcomes for this systematic review and meta-analysis. All were assessed postvitrectomy or final, except RD, which was analyzed separately for pre- and post-PPV. This study explored the effects of vitrectomy timing on outcomes, for patients with retained lens fragments managed surgically, after an initial wait for the eye to recover from cataract surgery.
Patients and Methods
The medline database was searched electronically and additional articles identified from reference lists. Search strategy details may be found in the Appendix (see Supplemental Material, available at AJO.com ). All study designs were considered, and no previous systematic review or meta-analysis on this topic was found. Articles passed the initial screen if at least 80% of patients (or identifiable subgroups) had intravitreal crystalline retained lens fragments from cataract surgery for an age-related cataract or if the article contained the same patients as another included article. The meta-analysis required counts for at least 1 outcome, 2 time periods (cataract surgery to vitrectomy), 10 patients, and 3 months mean follow-up.
Data were extracted twice, about 3 months apart, and discrepancies were resolved by reexamination of the article. For each study/outcome combination, the number of patients who had received a vitrectomy was recorded, separately for those who did and did not experience that outcome, for each time period. Data were eliminated for patients who received a vitrectomy before day 3 post cataract surgery or any group of patients whose average vitrectomy time post cataract surgery was less than 3 days.
Using SAS for Windows, version 9.2 (TS Level 1MO, 2006; SAS Institute Inc, Cary, North Carolina, USA), exact logistic regression was used to estimate the odds ratio, one for each study/outcome combination, for each additional 1-week vitrectomy delay (after day 3 post cataract surgery). All odds ratios (from the individual studies) for each outcome were then used to estimate a summary odds ratio for that outcome, using Comprehensive Meta Analysis, version 2.2 (Biostat Inc, Englewood, New Jersey, USA). Random-effects models were fit because of differences in the case-mix and clinical practices of the surgeons who authored the studies and the goal of the meta-analysis, which was to generalize the estimated summary effects to other patient populations.
Study quality was assessed using a checklist adapted from validated sources and a method proposed by Minckler. Reporting and publication biases were assessed using “trim & fill” and “fail safe N” analyses. Heterogeneity was assessed for all significant effects if the I statistic was greater than 0. A subgroup analysis assessed how the results differed between studies that included patients with only nuclear fragments from studies that also included patients with cortical fragments. Sensitivity analyses were performed to assess the effects of: 1) setting the cutoff for vitrectomies at day 3 post cataract surgery, 2) removing 1 study at a time, and 3) assuming that all significant effects were at the low end of their confidence intervals.
Results
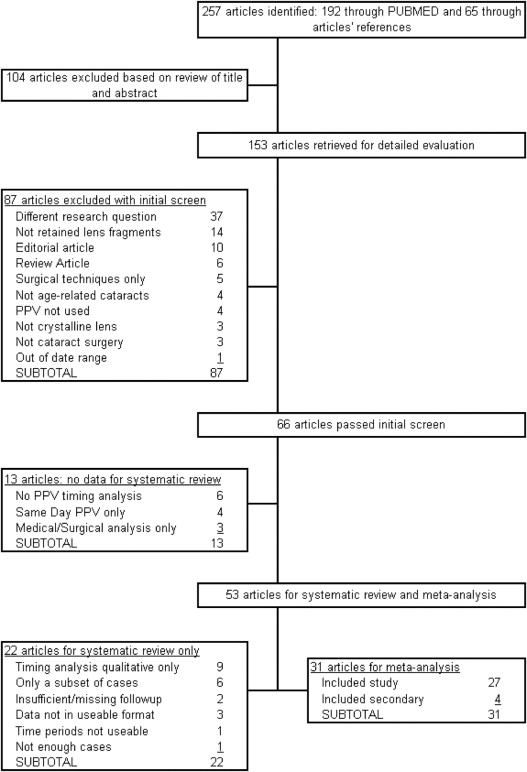
A total of 257 articles were identified, with 104 eliminated by reading the title and abstract. Full text of the remaining 153 articles was retrieved and reviewed. A total of 66 articles, comprising 56 unique study (patient) cohorts, passed the initial screen, but 13 did not report or discuss results for different vitrectomy timings (3+ days after cataract surgery). The remaining 53 articles, comprising 43 unique cohorts, were included in the systematic review, and 31 articles, comprising 27 unique cohorts, provided data for the meta-analysis. Figure 1 provides a summary of the search results.
To do a capture-recapture assessment of the search’s thoroughness, reference lists of all 66 articles were searched, and the Web of Science was searched for all articles (N = 228) that referenced any of these. It estimated the total relevant articles at 66 (95% CI, 62–70), indicating that, at most, 4 articles might have been missed.
Systematic Review of the Literature
Table 1 contains details for the 53 systematic review articles, published from 1986 through 2010. Geographic distribution was 28 in the United States/Canada, 16 in Europe, 8 in Asia, and 1 in Australia. Patients were treated from 1977 through 2008, with a mean of 6.0 years of elapsed time between the earliest and latest vitrectomies included in the article (range, 1–23 years). The 43 unique studies tended to be small, with 37 (86.0%) including fewer than 100 patients (range, 2–343) with data for 2380 eyes (mean = 55.3 eyes per study). Of these, 2323 (97.6%) received a PPV and 57 (2.4%) received medical management. Patient age averaged 73.8 years, and 54.1% (1078/1994) were female. Average time between cataract surgery and vitrectomy was just over 3 weeks, and average follow-up was estimated at 15.6 months. For studies with available data, Table 2 shows, for each outcome, whether early or later vitrectomy seemed better. The literature clearly contained more results, albeit many not statistically significant, favoring early vitrectomy.
| Study No. a | Study Use | Study ID b | Study Location (#L) | IPY-FPY (Inclusive) | # Eyes | # PPV (PPV %) | Patients’ Ages M/Md/Min/Max | Days CS to PPV M/Md/Min/Max | Follow-up (Months) M/Md/Min/Max |
|---|---|---|---|---|---|---|---|---|---|
| 1 | MA | Fastenberg 1991 | New York (1) | — | 13 | 11 (85) | —/—/27/88 | —/—/—/— | —/—/7/30 |
| 2 | MA | Blodi 1992 | Florida, Iowa, Illinois (3) | 1981-1990 | 36 | 32 (89) | —/—/—/— | —/—/—/— | 14/—/1/60 |
| 2a | SR | Flynn 1986 | Florida (1) | 1980-1983 | 2 | 2 (100) | —/81/75/86 | —/50/45/55 | —/5/—/— |
| 2b | SR | Smiddy 1996 | Florida (1) | 1981-1992 | 6 | 6 (100) | —/—/—/— | —/14/2/480 | 23/—/6/50 |
| 3 | MA | Gilliland 1992 | Texas (1) | 1979-1991 | 65 | 56 (86) | 73/—/40/90 | —/—/—/— | 20/—/—/— |
| 4 | MA | Pollet 1995 | Belgium (1) | 1991-1994 | 21 | 21 (100) | 68/—/39/86 | —/20/0/10950 | 10/—/—/— |
| 5 | MA | Tommila 1995 | Finland (1) | 1991-1994 | 23 | 23 (100) | 75/—/56/89 | —/7/0/53 | 11/—/3/20 |
| 6 | MA | Borne 1996 | Pennsylvania (1) | 1991-1994 | 121 | 121 (100) | 75/—/43/92 | 19/30/0/120 | 17/—/3/— |
| 7 | MA | Ross 1996 | British Columbia (1) | 1990-1994 | 54 | 46 (85) | 74/—/41/94 | —/—/0/— | 14/—/6/48 |
| 7a | MA | Ross 1993 | British Columbia (1) | — | 12 | 10 (83) | 77/76/53/94 | 20/12/0/93 | 16/16/6/26 |
| 8 | MA | Margherio 1997 | Michigan (1) | 1986-1996 | 126 | 126 (100) | 77/—/24/96 | —/—/—/— | 19/—/6/— |
| 9 | MA | Stilma 1997 | Netherlands (11) | 1988-1994 | 70 | 63 (90) | 75/—/47/88 | —/—/0/— | —/—/3/— |
| 10 | MA | Bessant 1998 | England (1) | 1991-1995 | 44 | 34 (77) | 68/—/20/87 | —/—/0/105 | 7/—/1/26 |
| 11 | MA | Stenkula 1998 | Sweden (2) | 1994-1994 | 19 | 19 (100) | 76/79/58/89 | 21/20/0/60 | 11/8/0/24 |
| 12 | MA | Watts 2000 | Wales (1) | 1995-1998 | 18 | 18 (100) | 74/76/62/87 | 10/5/0/77 | 14/12/6/34 |
| 13 | MA | Al-Khaier 2001 | England (1) | 1993-1998 | 89 | 89 (100) | 77/—/47/94 | —/15/0/357 | 6/—/1/60 |
| 13a | MA | Wong 1997 | England (1) | 1993-1994 | 19 | 19 (100) | 64/—/—/— | 29/20/2/192 | —/—/2/— |
| 14 | MA | Oruc 2001 | Missouri (1) | 1990-1998 | 85 | 85 (100) | 74/—/—/— | —/—/—/— | 10/—/2/72 |
| 15 | MA | Hansson 2002 | Sweden (1) | 1997-2000 | 66 | 66 (100) | —/80/41/94 | —/3/0/255 | —/8/0/30 |
| 16 | MA | Yang 2002 | Taiwan (2) | 1992-1998 | 25 | 24 (96) | 70/72/40/90 | 25/17/0/97 | 10/6/3/44 |
| 17 | MA | Scott 2003 | Florida (1) | 1990-2001 | 343 | 343 (100) | —/76/24/100 | —/12/0/— | —/8/1/96 |
| 17a | MA | Moore 2003 | Florida (1) | 1990-2001 | 343 | 343 (100) | —/76/24/100 | —/13/0/— | —/8/1/96 |
| 17b | MA | Kim 1994 | Florida (1) | 1990-1992 | 62 | 62 (100) | 75/—/51/91 | —/—/0/365 | —/—/—/— |
| 17c | SR | Vilar 1997 | Florida (1) | 1993-1995 | 126 | 126 (100) | 74/—/40/94 | —/—/0/225 | 12/—/1/36 |
| 17d | SR | Smiddy 2003 | Florida (1) | 1994-2001 | 101 | 101 (100) | 76/—/—/— | 22/8/0/366 | 14/9/3/82 |
| 17e | SR | Irvine 1992 | Florida (1) | 1991-1991 | 4 | 4 (100) | —/81/74/90 | —/103/50/368 | —/5/2/8 |
| 17f | SR | Kim 1996 | Florida (1) | 1990-1994 | 5 | 5 (100) | —/77/73/84 | —/17/5/198 | —/10/3/21 |
| 18 | MA | Stefaniotou 2003 | Greece (1) | — | 26 | 26 (100) | 67/—/59/90 | —/—/—/— | —/—/3/9 |
| 19 | MA | van der Meulen 2004 | Netherlands (1) | 1996-2000 | 13 | 13 (100) | 77/77/63/84 | 14/9/2/50 | 29/28/3/69 |
| 20 | MA | Ruiz-Moreno 2006 | Spain (1) | — | 18 | 18 (100) | 71/71/58/87 | 8/7/0/24 | 34/45/6/53 |
| 21 | MA | Ho SF 2007 | England (1) | 2000-2006 | 82 | 82 (100) | —/78/48/85 | —/—/—/— | —/27/4/48 |
| 22 | MA | Merani 2007 | Australia (1) | 1998-2003 | 223 | 223 (100) | 76/78/53/93 | 10/4/0/132 | 21/15/0/66 |
| 23 | MA | Romero-Aroca 2007 | Spain (1) | 1997-2005 | 47 | 47 (100) | 73/—/57/86 | —/—/—/— | 63/—/12/106 |
| 24 | MA | Tajunisah 2007 | Malaya (1) | 2001-2005 | 22 | 22 (100) | 69/68/52/84 | 11/5/0/60 | 9/—/1/24 |
| 25 | MA | Chen 2008 | Taiwan (1) | 2000-2006 | 78 | 78 (100) | 70/—/24/92 | —/—/—/— | 14/—/5/47 |
| 26 | MA | Schaal 2009 | Kentucky (2) | 2000-2006 | 42 | 27 (64) | 71/—/59/85 | —/—/—/— | 12/12/12/12 |
| 27 | MA | Ho LY 2010 | Michigan (1) | 2005-2008 | 17 | 17 (100) | 73/—/58/85 | 7/—/2/17 | 5/—/1/16 |
| 28 | SR | Lambrou 1992 | Florida (1) | 1988-1990 | 8 | 8 (100) | 77/78/64/88 | 8/3/1/36 | 12/10/2/22 |
| 29 | SR | Greve 1993 | Louisiana (6) | 1989-1992 | 17 | 17 (100) | 74/—/56/91 | —/—/—/— | 13/—/0/8 |
| 30 | SR | Kapusta 1996 | Quebec (1) | 1991-1995 | 25 | 25 (100) | 77/—/60/94 | —/—/0/90 | —/6/2/— |
| 31 | SR | Terasaki 1997 | Japan (1) | 1995-1998 | 15 | 14 (93) | 74/76/56/86 | 3/3/0/7 | —/—/—/— |
| 32 | SR | Boscher 1998 | France (1) | 1993-1996 | 21 | 21 (100) | 75/—/45/96 | 15/—/1/120 | 21/—/7/37 |
| 33 | SR | Joondeph 1999 | Michigan (1) | — | 14 | 14 (100) | —/—/42/90 | —/—/1/56 | —/—/—/— |
| 34 | SR | Lu 1999 | China (—) | — | 3 | 3 (100) | —/—/—/— | —/—/—/3 | —/—/—/— |
| 35 | SR | Yeo 1999 | England (1) | 1995-1996 | 22 | 22 (100) | —/—/—/— | —/—/0/97 | —/—/3/9 |
| 36 | SR | Verma 2001 | India (1) | 1997-1999 | 24 | 24 (100) | 54/—/40/77 | 29/—/0/99 | —/—/3/— |
| 37 | SR | Wilkinson 2001 | Maryland (1) | 1977-1999 | 135 | 135 (100) | —/—/42/89 | —/—/0/6935 | —/—/—/— |
| 38 | SR | Kwok 2002 | Hong Kong (1) | 1993-1999 | 27 | 27 (100) | 74/—/54/85 | 10/—/0/70 | 31/—/3/60 |
| 39 | SR | Schwartz 2002 | Texas (2) | 1995-1999 | 26 | 26 (100) | —/—/—/— | —/6/1/77 | 6/6/6/6 |
| 40 | SR | Murat Uyar 2003 | Turkey (1) | 1998-2000 | 43 | 43 (100) | 65/—/46/79 | 15/—/0/90 | 8/—/2/27 |
| 41 | SR | Greven 2004 | North Carolina (2) | 1994-2000 | 42 | 42 (100) | 73/73/39/89 | —/—/—/— | 30/25/6/— |
| 42 | SR | Kiss 2008 | Massachusetts (1) | 2007-2007 | 6 | 6 (100) | —/—/—/— | 19/19/2/30 | —/—/—/— |
| 43 | SR | Ho LY 2009 | Pennsylvania (1) | 2001-2007 | 166 | 166 (100) | —/75/37/98 | —/4/0/139 | 20/—/3/69 |
a Patients in a study whose number includes a letter are a subset of the patients in the correspondingly numbered study (ie, patients in study 7a are also in study 7).
| Study No. b | Study ID c | VA | RD Pre | RD Post | IOP | IOI | CME | CE |
|---|---|---|---|---|---|---|---|---|
| 1 | Fastenberg 1991 | — | — | — | E-nSS | E-nSS | — | — |
| 2 | Blodi 1992 | no infl | — | no infl | E-SS | E-nSS | no infl | no infl |
| 3 | Gilliland 1992 | no infl | — | — | no infl | — | — | — |
| 4 | Pollet 1995 | — | — | — | E-nSS | — | — | — |
| 5 | Tommila 1995 | E-nSS | — | — | E-nSS | — | — | — |
| 6 | Borne 1996 | E-nSS | — | — | — | — | — | — |
| 7 | Ross 1996 | E-nSS | — | — | E-nSS | — | — | — |
| 7a | Ross 1993 | no infl | E-nSS | E-nSS | — | — | L-nSS | — |
| 8 | Margherio 1997 | E-nSS | E-nSS | no infl | E-nSS | no infl | L-nSS | no infl |
| 9 | Stilma 1997 | E-nSS | — | — | — | — | — | — |
| 10 | Bessant 1998 | E-nSS | — | E-nSS | L-nSS | — | — | — |
| 11 | Stenkula 1998 | E-nSS | — | — | no infl | no infl | — | — |
| 12 | Watts 2000 | E-nSS | — | — | E-nSS | E-nSS | — | — |
| 13 | Al-Khaier 2001 | E-SS | — | — | no infl | — | — | — |
| 13a | Wong 1997 | — | — | E-nSS | — | — | — | — |
| 14 | Oruc 2001 | M-nSS | — | — | — | — | — | — |
| 15 | Hansson 2002 | E-nSS | — | — | no infl | — | — | — |
| 16 | Yang 2002 | E-nSS | E-nSS | — | — | E-nSS | — | — |
| 17 | Scott 2003 | E-nSS | — | — | E-nSS | — | — | — |
| 17a | Moore 2003 | — | no infl | E-nSS | — | — | — | — |
| 17b | Kim 1994 | E-nSS | — | — | E-nSS | — | — | — |
| 17c | Vilar 1997 | no infl | — | E-nSS | no infl | — | — | — |
| 18 | Stefaniotou 2003 | E-nSS | E-nSS | E-nSS | E-nSS | no infl | — | — |
| 19 | van der Meulen 2004 | M-nSS | — | — | no infl | — | E-nSS | — |
| 20 | Ruiz-Moreno 2006 | no infl | — | no infl | E-nSS | — | — | — |
| 21 | Ho SF 2007 | E-SS | — | E-nSS | E-nSS | — | — | — |
| 22 | Merani 2007 | E-nSS | E-nSS | E-nSS | no infl | no infl | E-nSS | unclear |
| 23 | Romero-Aroca 2007 | E-SS | — | — | E-SS | — | E-SS | — |
| 24 | Tajunisah 2007 | no infl | — | — | — | — | — | — |
| 25 | Chen 2008 | E-SS | E-nSS | E-nSS | E-SS | no infl | E-nSS | — |
| 26 | Schaal 2009 | M-nSS | Excl | — | E-nSS | — | no infl | — |
| 27 | Ho LY 2010 | no infl | E-nSS | — | — | — | — | — |
| 28 | Lambrou 1992 | E-nSS | — | — | — | — | — | — |
| 29 | Greve 1993 | — | — | — | E-nSS | — | — | — |
| 30 | Kapusta 1996 | no infl | — | — | — | — | — | — |
| 31 | Terasaki 1997 | E-nSS | — | — | — | — | — | — |
| 32 | Boscher 1998 | L-nSS | — | — | — | — | — | — |
| 33 | Joondeph 1999 | — | — | — | E-nSS | — | — | — |
| 35 | Yeo 1999 | E-SS | — | — | E-SS | — | — | — |
| 36 | Verma 2001 | E-nSS | — | — | — | — | — | — |
| 38 | Kwok 2002 | no infl | — | — | no infl | — | — | — |
| 39 | Schwartz 2002 | E-nSS | — | — | — | — | — | — |
| 40 | Murat Uyar 2003 | no infl | — | — | no infl | — | — | — |
| 41 | Greven 2004 | no infl | — | — | — | — | — | — |
| 42 | Kiss 2008 | no infl | — | — | E-nSS | — | — | E-nSS |
| 43 | Ho LY 2009 | unclear | — | unclear | E-SS | — | unclear | — |
a P values are approximate and may be based on the article and/or logistic regression estimates (which were done for the meta-analysis).
b Patients in a study whose number includes a letter are a subset of the patients in the correspondingly numbered study (ie, patients in study 7a are also in study 7).
First week analysis
One issue is whether to attempt a vitrectomy on the same day as cataract surgery. While recommended by some, others stress that this precludes moving the patient or waiting until later the same day. However, some authors indicated that cataract surgery anesthesia may make a same-day vitrectomy more difficult, and another felt same-day vitrectomy was not necessary.
One author suggested vitrectomy the day after cataract surgery, but many suggested avoiding this time to wait until the eye recovers from cataract surgery (to clear ocular congestion, inflammation, and corneal edema). Emergent vitrectomy, within 3 days of cataract surgery, was associated with reduced visual acuity and retinal tears in 1 study and hypopyon and possible endophthalmitis in another. In a third study, of 3 patients who had a vitrectomy for retained lens fragments within 72 hours of cataract surgery, 1 patient had CME, another had choroidal detachment, and all 3 had moderate to severe inflammation.
The first few days after cataract surgery may not be optimal for a vitrectomy. This time might best be avoided, except in extraordinary circumstances, when any delay is impossible. Using individual patient data from studies (n = 12) that provided the exact day, post cataract surgery, of each patient’s vitrectomy, Table 3 shows visual acuity outcomes for each day of the first week. Rates changed for both good and bad visual acuity, with days 3 through 7 having more good and fewer bad results (Mantel-Haenszel χ 2 test for trend, P = .006). Table 3 also shows these data aggregated into days 0 through 2 and 3 through 7, which also indicated a significant trend toward better visual acuity outcomes for vitrectomies on days 3 through 7 (Mantel-Haenszel χ 2 test for trend, P = .004). Based on this analysis, days 0 through 2 were considered as recovery time, and the meta-analysis was limited to patients who received a vitrectomy 3 or more days (on average, for grouped data) after cataract surgery. The hypothesis of a constant odds ratio from one week to the next, for each additional 1 week of vitrectomy delay, would not have been valid if data for the eye’s recovery time remained in the analysis.
| Visual Acuity b | Day of Vitrectomy After Cataract Surgery | Aggregated | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | TOTAL | 0–2 | 3–7 | |
| Number of Patients | |||||||||||
| Good | 12 | 3 | 9 | 3 | 6 | 4 | 8 | 6 | 51 | 24 | 27 |
| Moderate | 4 | 2 | 6 | 4 | 2 | 1 | 1 | 2 | 22 | 12 | 10 |
| Bad | 7 | 4 | 7 | 1 | 0 | 1 | 1 | 0 | 21 | 18 | 3 |
| TOTAL | 23 | 9 | 22 | 8 | 8 | 6 | 10 | 8 | 94 | 54 | 40 |
| Percentage of Patients | |||||||||||
| Good | 52.2 | 33.3 | 40.9 | 37.5 | 75.0 | 66.7 | 80.0 | 75.0 | 44.4 | 67.5 | |
| Moderate | 17.4 | 22.2 | 27.3 | 50.0 | 25.0 | 16.7 | 10.0 | 25.0 | 22.2 | 25.0 | |
| Bad | 30.4 | 44.4 | 31.8 | 12.5 | 0.0 | 16.7 | 10.0 | 0.0 | 33.3 | 7.5 | |
a Data are from 12 articles that provided the necessary detailed individual patient data for this analysis.
b Visual acuity (VA) good = VA ≥/>0.5 or 20/40; VA moderate = VA 0.5 to 0.1 or 20/40 to 20/200; VA bad = VA ≤/<0.1 or 20/200.
Power analysis
Many authors indicted that nonsignificant results might have been attributable to small samples and low power, but no author reported a power analysis. Each study’s power for comparing outcomes was estimated, and the results (mean = 23%, median = 13%) indicated that, indeed, many studies had low power.
Quality analysis
No study in the meta-analysis was prospective or randomized, but unbiased inclusion/exclusion criteria were clearly described. Data collection was not masked since all who assessed outcomes and risk factors were aware of treatment status, but all risk factors were recorded before outcomes occurred in medical records, which lack research biases. In 19 of 27 studies (70%), patients were a consecutive series (a representative sample), and 24 studies (89%) stated years of service. In 24 studies (89%), patients’ characteristics at presentation were reported, but only 7 studies (26%) reported pre-existing ocular comorbidities. In 25 studies (93%), all patients were accounted for, while reasons were given for all lost/excluded patients in 26 studies (96%), but in only 20 studies (74%) was information reported on all patients excluded for missing data or lost to follow-up. In 19 studies (70%), authors indicated their criteria for treatment choice and/or vitrectomy timing, but in only 13 studies (48%) was a standardized assessment of outcomes specified and actual probabilities reported.
Using the Minckler evidence-based rating system, for clinical importance 23 studies were rated A, 1 rated B, and 2 rated C; and for strength of evidence all were rated III (weak). One study reported data for all 8 outcomes, 2 for 6 outcomes, 3 for 5 outcomes, 5 for 4 outcomes, 4 for 3 outcomes, 9 for 2 outcomes, and 3 for 1 outcome. Three studies had an average follow-up time between 3 and 6 months, 11 between 6 and 12 months, 9 between 12 and 24 months, and 4 greater than 24 months.
Meta-Analysis
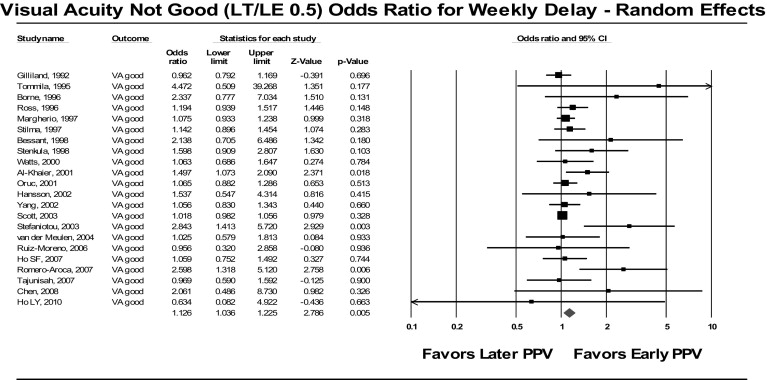
The 27 studies with data for the meta-analysis included 1730 vitrectomized eyes. Results indicated that earlier vitrectomy (day 3+ post cataract surgery) may be better for all outcomes, with significant effects for not good visual acuity (odds ratio: 1.13; 95% CI: 1.04–1.22; P = .005); bad visual acuity (odds ratio: 1.05; 95% CI: 1.01–1.09; P = .009); previtrectomy RD (odds ratio: 1.29; 95% CI: 1.01–1.65, P = .038); postvitrectomy RD (odds ratio: 1.13; 95% CI: 1.02–1.26; P = .024); increased IOP (odds ratio: 1.23; 95% CI: 1.07–1.41; P = .003); and intraocular inflammation/ infection (odds ratio: 1.20; 95% CI: 1.01–1.42; P = .041). Effects for CME (odds ratio: 1.05; 95% CI: 0.74–1.49; P = .770) and corneal edema (odds ratio: 1.09; 95% CI: 0.88–1.35; P = .434) were not significant. Figure 2 shows a sample forest plot summarizing the results of a meta-analysis.