Vitrectomy Techniques and Technology for Anterior Segment Problems
 Although developed for posterior vitreoretinal surgery, the vitrectomy instrument has widespread application to anterior segment surgery (1, 2, 3, 4, 5, 6, 7, 8). Every anterior segment microsurgeon must have vitrectomy techniques and equipment at his or her fingertips to manage vitreous loss during cataract surgery and other common problems. The anterior segment microsurgeon with extensive knowledge of corneal physiology, aqueous dynamics, intraocular lenses (IOLs), cataract complications, and microsurgical techniques need not rely on a posterior segment surgeon to manage all anterior segment vitreous problems. Similarly, an anterior segment surgeon should not delve into complex vitreoretinal problems just because the technology is available. The demands are so complex that it is a very unique individual who is an expert in both arenas. Perhaps the most important issue to convey to anterior segment surgeons is that proper management of vitreous is critical for the prevention of postoperative retinal detachments.
Although developed for posterior vitreoretinal surgery, the vitrectomy instrument has widespread application to anterior segment surgery (1, 2, 3, 4, 5, 6, 7, 8). Every anterior segment microsurgeon must have vitrectomy techniques and equipment at his or her fingertips to manage vitreous loss during cataract surgery and other common problems. The anterior segment microsurgeon with extensive knowledge of corneal physiology, aqueous dynamics, intraocular lenses (IOLs), cataract complications, and microsurgical techniques need not rely on a posterior segment surgeon to manage all anterior segment vitreous problems. Similarly, an anterior segment surgeon should not delve into complex vitreoretinal problems just because the technology is available. The demands are so complex that it is a very unique individual who is an expert in both arenas. Perhaps the most important issue to convey to anterior segment surgeons is that proper management of vitreous is critical for the prevention of postoperative retinal detachments.VITRECTOMY INSTRUMENT CHOICE
The large size and fluid flow characteristics of full function probes make them as inappropriate for anterior segment surgery as they are for posterior segment surgery. Disposable, small, lightweight, pneumatic, 23- or 25-gauge cutters, high-speed cutting, and fast proportional (linear) suction control are a necessity for anterior segment surgery, just as they are for vitreoretinal procedures (Chapter 2).
INFUSION SYSTEMS FOR ANTERIOR VITRECTOMY
Infusion can be provided by the infusion sleeve (9), which slips over the vitrectomy instrument through a limbal incision for a one-incision technique (Chapter 2). This method is easy to use but results in a return to the turbulent fluid flow observed with full function probes (Fig. 7.1). Use of the infusion sleeve should be limited to vitrectomy in soft eyes with no sideport, a rare situation.
A bimanual approach (10) with a blunt 30-degree bent infusion cannula as the infusion device is used if the pars plana cannot be seen, as well as for retinopathy of prematurity (ROP) (5). This technique allows the independently movable infusion to hydrate and mobilize the lens material for aspiration. By using 25-gauge infusion, the infusion needle can be interchanged with a cutter to provide better access to the posterior chamber and periphery.
The authors encourage anterior segment surgeons to develop bimanual surgery dexterity by using bimanual irrigation and aspiration techniques for lens cortex removal. The surgeon can use the bimanual I/A irrigation tip during anterior vitrectomy as well. If this instrument is used, the decrease in caliber (and irrigation flow capacity) should be compensated by decreasing the aspiration flow limit of the vitrectomy system, otherwise collapse of the anterior chamber can occur during surgery.
Unsupported butterfly needles or silicone tubing should not be used for anterior chamber infusion because they may damage the endothelium and offer no help in accessing the posterior chamber for manipulation of cortex. Sew-on corneal infusion cannulas do not permit changing the active instrument from one hand to the other and can cause corneal damage via mechanical trauma or fluid directed against endothelium.
ULTRASONIC FRAGMENTATION
Aspirating ultrasonic fragmenters such as the Alcon Accurus four-crystal device and the Constellation permit 20-gauge
incisions to be used for relatively dense cataracts (11,12). The 20-gauge aspirating fragmenters require a separate infusion cannula identical to modern vitrectomy systems. The phacoemulsifier is analogous to the full function vitrectomy approach and similarly requires a larger incision and creates more turbulence.
incisions to be used for relatively dense cataracts (11,12). The 20-gauge aspirating fragmenters require a separate infusion cannula identical to modern vitrectomy systems. The phacoemulsifier is analogous to the full function vitrectomy approach and similarly requires a larger incision and creates more turbulence.
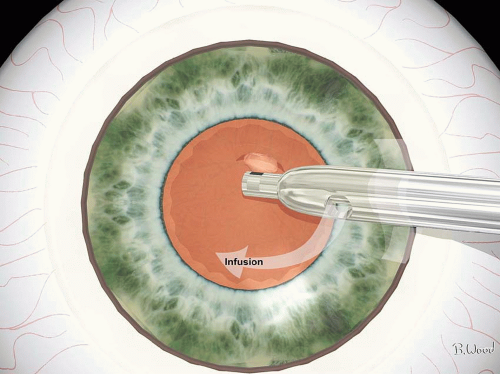 Figure 7.1 ▪ Infusion sleeves increase infusion fluid turbulence, resulting in endothelial cell damage. |
Current 25- and 23-gauge vitrectomy systems lack a fragmenter in both gauge diameters. The only available fragmenter at the time of this writing is 20 gauge. On the other hand, modern fluidics in both 25- and 23-gauge systems allow removal of soft nuclei with the vitrectomy probe alone. Only harder nuclei require the creation of a 20-gauge wound to introduce the fragmenter.
Infusion Sources
Infusion can be accomplished with the same options used with the vitrectomy instrument: bimanual, with 20-gauge, 30-degree bent, blunt cannula, infusion sleeve, sew-on infusion cannula or 25-gauge trocar-cannula system.
The metal infusion sleeve, which has the potential of dampening the sonic energy, is not intended for use with the fragmenter. Bimanual infusion with the angulated, blunt cannula can be kept away from the suction port, decreasing turbulence, and may be used for selective mobilization and hydration of lens material in certain cases.
Vacuum Sources
Syringes, peristaltic pumps, or venturi-based systems can provide suction for the vitrectomy probe or aspirating fragmenter. For the reasons discussed in Chapter 2, venturi-based vacuum systems are far superior to the other approaches because they reduce vitreoretinal traction and ocular collapse. A vitrectomy system with proportional (linear) suction control of a venturi source offers the most precise control over suction level currently available.
Leaving the fragmenter lumen open to the atmosphere (incorrectly called “passive egress”) is inappropriate because precision, foot control, and reflux capability are lost. The tubing can be squeezed to create reflux if the iris or retina becomes impacted in the port. Certain vitrectomy systems (Accurus and Constellation Vision System) offer foot pedal-controlled reflux. Foot pedal control is also available with the vitrectomy mode of phaco systems such as the Alcon Legacy and Infinity.
Modern phaco technique(s) utilizing high suction and limited flow rates are not used with current fragmenters because of the 20-gauge needle configuration.
Intermittent Versus Continuous Sonification and Aspiration
Bursts of intermittent sonification alternated with aspiration have been recommended for fragmenter use, but they prolong the procedure and cause unnecessary heating of the sclera (13). Aspiration without sonification is ineffective and time consuming. Luminal fluid flow is the most effective means of dissipating frictional heat generated by the fragmenter in the wound. Squirting fluid on the needle shank externally does not cool the internal scleral wound. By combining continuous sonification with continuous aspiration, a safe and rapid lensectomy can be performed using the continual luminal fluid flow for scleral cooling.
Limbal Versus Pars Plana Approach for Anterior Vitrectomy
Elective anterior vitrectomy during routine cataract removal should be reserved only for selected pediatric cataracts or for those cases in which the anterior vitreous cortex and an opaque posterior capsule resistant to polishing are firmly adherent. Complete posterior capsulectomy from the limbal approach almost always results in anterior vitrectomy because of the approach angle and posterior displacement of the posterior capsule from the infusion system.
While the limbal approach to anterior vitrectomy is more comfortable for the anterior segment surgeon, it creates more endothelial and iris trauma than pars plana surgery. Limbal anterior vitrectomy should be reserved for intraoperative cataract surgery complications if the surgeon is not comfortable with sideport infusion combined with pars plana vitrectomy. Peripheral anterior synechia frequently form at the limbal wounds postoperatively. The pars plana approach allows more complete removal of peripheral membranes and vitreous without iris trauma (see “Pupillary Membranes”). If conversion to posterior vitrectomy becomes necessary, the limbal approach is inappropriate because the angulated instruments cause striate keratopathy. Most pupillary or retro-IOL membranectomies should be done through the pars plana. Translimbal bimanual lensectomy should be used for radiation cataracts in retinoblastoma patients and in some cases of severe iris-retinal adherence when pars plana entry is unsafe.
PARS PLANA LENSECTOMY
Indications
Pars plana lensectomy (PPL) is not indicated for elective cataract removal unless the lens is subluxated or dislocated. The obligatory interruption of the anterior vitreous cortex increases retinal complications (cystoid macular edema [CME] and retinal detachment), and it is not compatible with endocapsular IOL implantation. The principal role of PPL is in combination with indicated pars plana vitrectomy (PPV).
Many phakic, proliferative vitreoretinopathy (PVR) (Chapter 9) and giant break (Chapter 10) cases often require PPL even if the lens is clear. Many trauma cases require removal of the lens because of associated lens damage or ciliary body damage.
Aphakic eyes allow better visualization, better approach to the anterior vitreous cortex and peripheral vitreous, and easier fluid-air or fluid-gas exchange; eliminate the substrate for cyclitic membrane formation; and allow faster egress of cells, protein, fibrin, fibronectin, hemorrhage, and growth factors. Clear lenses should not be removed in a vitrectomy performed for proliferative diabetic retinopathy (PDR) because of the increased risk of neovascular glaucoma unless there is fibrin syndrome, there is a high probability of postoperative bleeding, or silicone is used for large retinectomies. It is thought that the anterior vitreous cortex and the lens act as a barrier to diffusion of vascular endothelial growth factor (VEGF) to the anterior segment; VEGF causes neovascularization of the iris and trabecular meshwork. For this theoretical reason and to reduce posterior subcapsular cataract rates, the anterior vitreous cortex should be avoided in diabetic vitrectomies in which the lens is left in place, unless it is opaque. The indications for elective clear lens and anterior vitreous cortex removal without IOL implantation in the diabetic patient will be explained in a subsequent chapter.
Development of Pars Plana Lensectomy
The development of vitrectomy and phacoemulsification has an intertwined and interesting history. The first vitrectomy infusion, suction cutter was patented by Anton Banko in 1969 in response to vitreous complications of early phacoemulsification. Banko had learned of the need for a vitreous cutter because he developed the fluidics for Kelman’s early phacoemulsifier. Machemer developed the trans-PPV procedure in 1970 and shortly thereafter performed lensectomy with the vitreous suction cutter (VISC). It was soon discovered that the vitreous cutter would not handle significant nuclear sclerosis. Girard developed the fragmenter with Sparta in 1972 as a phacoemulsifier alternative without the coaxial infusion sleeve. One of the authors (S.C.) was the first advocate of PPL using the Girard fragmenter with aspiration. Girard advocated vitrectomy with his unit and later recommended using the fragmenter for routine cataract surgery. The author believes that ultrasonic vitrectomy and PPL for routine cataract surgery are unsafe. Shock adapted a dental unit to cataract surgery just as Kelman had done at an earlier date but, like Girard, could not use a coaxial infusion sleeve, which had been patented by Kelman. The Shock technique required a large, intentionally leaky wound and was used with infusion through the fragmenter needle rather than suction. Machemer used the Shock system with a large, leaky pars plana incision for cases with nuclear sclerosis too great for the VISC.
Conventional Fragmenter Techniques
Current practice for PPL with the fragmenter begins after standard 25-, 23-, or 20-gauge port placement. The surgeon may attempt lensectomy with the vitreous cutter if the lens does not appear too dense. Once a decision to perform lensectomy with a 20-gauge fragmenter is done, the conjunctiva and sclera should be opened as described in the 20-gauge wound construction chapter.
The next step in conventional lensectomy is to incise the equatorial lens capsule with the microvitreoretinal (MVR) blade. The author used the fragmenter to incise the lens capsule before endocapsular lensectomy was developed. The fragmenter method was initiated to avoid the stress that capsular incision with the MVR blade creates on the zonules. Many surgeons advocate penetration of the nucleus with the MVR blade. This step is unnecessary if the nucleus is soft and creates excessive stress on the zonules if the nucleus is hard.
After incising the lens capsule, the fragmenter is used in what phaco surgeons would call a sculpting mode to remove lens material. The author has advocated sculpting in a plane parallel to the iris, starting on the temporal side adjacent to
the entry site. An initial thick sheet of cortex and nucleus is removed while being careful to avoid the cortex near the anterior and posterior lens capsules. The posterior capsule is much weaker than the anterior capsule and is usually not intact by the time the posterior cortex has been removed.
the entry site. An initial thick sheet of cortex and nucleus is removed while being careful to avoid the cortex near the anterior and posterior lens capsules. The posterior capsule is much weaker than the anterior capsule and is usually not intact by the time the posterior cortex has been removed.
Some surgeons recommend alternating aspiration and sonification. Unlike the phacoemulsifier, the fragmenter has no infusion sleeve and must rely on fluid flow through the lumen for cooling. The needle has approximately 0.003 inches of longitudinal movement and generates significant frictional heat. By contrast, the author has always recommended continuous and simultaneous sonification and aspiration. The constant fluid flow cools the needle and therefore the sclera. If white, particulate matter (lens milk) appears at the needle tip, the surgeon must release the foot pedal immediately to avoid scleral burns. If the needle becomes clogged, it should be back flushed with a syringe filled with balanced salt solution (BSS) with the ultrasound activated after double-checking to determine that the needle is outside the eye. Aspiration of saline from a cup is never effective, nor is it necessary to clean the needle with a stylet or replace the needle if it becomes plugged.
Infusion Options
Many surgeons recommend placing a separate infusion into the lens rather than using the pars plana infusion cannula. If the lens is soft, infusion directly into the lens is not necessary. If the lens is hard, infusion into the lens will not reach the temporal side where the sculpting must begin. Infusion into the lens tends to force lens material through ever-present defects in the posterior capsule. For this reason, the authors use only the pars plana infusion cannula for lensectomy cases except during hydrodissection.
Lens Capsule Removal
In the presence of anterior PVR or severe intraocular inflammation, placement of an IOL should not be performed and complete capsulectomy is recommended to decrease postoperative inflammation and remove the substrate for cyclitic membrane formation. Most surgeons use the vitreous cutter to remove the capsule. The senior author has recommended end-opening forceps to remove the capsule since the late 1970s. The author has used the diamond-coated forceps developed with Grieshaber since they became available in the late 1980s. Zonulorhexis is performed in a circular motion identical to capsulorhexis. Care must be taken to avoid engaging the vitreous so as to prevent undue force on the retina. Using the vitreous cutter to remove lens capsule frequently damages the iris, causes miosis, prolongs operating time, may cause bleeding, and leaves residual lens material. Residual capsule and lens material cause inflammation and may lead to cyclitic membranes and closure of peripheral iridectomies, especially the inferior peripheral iridectomy necessary in aphakic silicone oil cases.
 Figure 7.2 ▪ Alcon Constellation fragmenter and phaco probes. |
Fragmenter Performance
The original fragmenter handpieces sold by Berkley Bioengineering, Coopervision, Sparta, Fibrasonics, MidLabs, Storz, and Alcon were all made by Fibrasonics. These fragmenters were useful but had less power than the phacoemulsifier and hence more difficulty with dense nuclear sclerosis. Alcon introduced a four-crystal fragmenter in the early 1990s that uses the same ultrasonics as the Legacy and Infinity phacoemulsifiers. The Alcon Accurus and Constellation fragmenters (Fig. 7.2) will handle dense nuclear sclerosis just as well as the phacoemulsifier.
Phacoemulsification with Pars Plana Vitrectomy
As both phacoemulsification and vitrectomy techniques have become more sophisticated, performing safe combined phaco-vitrectomy technique is a possibility for select patients. This issue is discussed further in Chapter 8.
Anterior Lens Capsule Retention and Lens Implantation in the Sulcus
The late Ron Michels was long an advocate of preserving the anterior lens capsule until the end of the vitrectomy to reduce damage to the endothelium and trabecular meshwork induced by erythrocytes, infusion fluid, and turbulence. Kokame and Blankenship reported retention of the anterior lens capsule to permit the implantation of posterior chamber lens in the ciliary sulcus at the end of the vitrectomy. They recommended performing an anterior capsulotomy after lens implantation. Some phaco surgeons have been critical of this procedure because endocapsular implantation has better results than ciliary sulcus placement in elective cataract surgery. The authors have had very good results with this method with no cases of decentration. Capsular fibrosis occurs rapidly if the capsule is in contact with silicone oil. The authors have found that polishing the capsule increases the chance of preserving a clear capsule. The authors use Acrysof three-piece foldable acrylic lens from Alcon through a 2.2-mm keratome, clear corneal incision with implantation in the sulcus, anterior to the retained anterior capsule after the vitrectomy. One should avoid the use of silicone lenses as they absorb silicone oil and have marked condensation problems during fluid-air (gas) exchange. Phaco-vitrectomy has virtually eliminated the need for this method.
Endocapsular Lensectomy Method
Conventional lensectomy, as described previously, has many of the attributes of endocapsular phaco except that it starts with a risky, equatorial capsular incision. This equatorial defect frequently leads to capsular tears that extend into the anterior capsule. Extension of capsular tears was a frequent problem in phaco surgery until the continuous capsulorhexis was developed. Cataract surgery has seen a progression from intracapsular to extracapsular surgery and, ultimately, phacoemulsification. Phaco has evolved from anterior chamber phaco to iris plane phaco to endocapsular surgery. Continuous capsulorhexis has dramatically reduced problems with capsular tears for the cataract surgeon.
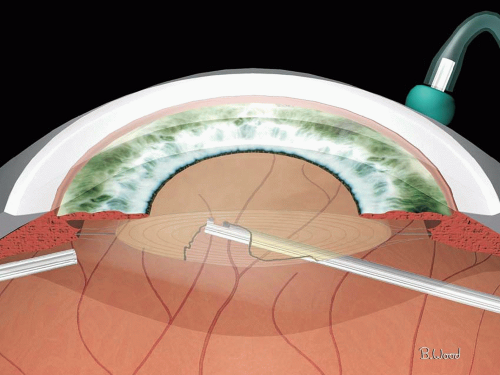 Figure 7.3 ▪ Posterior capsulorhexis is performed with the vitreous cutter after anterior vitrectomy to prevent engagement of vitreous in the fragmenter. |
Endocapsular Lensectomy Surgical Sequence
One of the authors (S.C.) has been using posterior capsulorhexis, cortical cleaving hydrodissection, and sculpting since 1994 and has found these techniques of great value in lensectomy. This approach is referred to as endocapsular lensectomy.
Endocapsular lensectomy begins with placement of the ports as described previously for conventional lensectomy. The endoilluminator is essential to stabilize the eye and provide a controllable red reflex. The endoilluminator can be touched to the lens capsule in various locations to aid in visualization without the light toxicity associated with retina-reflective red reflex methods. The sclerotomy for the fragmenter is made superotemporally for the capsulorhexis, hydrodissection, sculpting, and cortex-aspiration tools.
A central posterior capsulorhexis is made with vitreous cutter (Fig. 7.3) after a limited anterior vitrectomy. The vitrectomy is performed to prevent vitreoretinal traction from the fragmenter. Cortical cleaving hydrodissection is the next step. A blunt, 27-gauge cannula attached with a
short length of tubing to a 5-mL syringe operated by the assistant is used for this step (Fig. 7.4). If endocapsular lensectomy is attempted with the 25-gauge cutter without the fragmenter, hydrodissection can be performed with a 27-gauge needle advanced through the 25-gauge cannula to the edge of the posterior capsulectomy. Sculpting without nuclear cleaving or rotation is then initiated at the temporal margin of the nucleus to avoid damaging the capsule with the fragmenter. The Alcon 20-gauge, four-crystal fragmenter is used to sculpt the nucleus, epinucleus, and finally the cortex (Fig. 7.5). This fragmenter has the same ultrasonics as the Legacy. The anterior cortex is avoided to prevent
damaging the anterior capsule. The vitreous cutter is used for aspirating the remaining cortex. The vitreous cutter is better than classic irrigation/aspiration (I/A) tools because of the cutting capability that acts like chopping. The anterior capsule is polished after aspirating the cortex (Fig. 7.6). Almost any posterior chamber lens could theoretically be utilized, but foldable lenses offer the advantage of a smaller incision. The hydrophobic foldable acrylic multipiece lens (Alcon Acrysof) is currently being utilized because of the low incidence of capsular opacification. Scleral tunnel or clear cornea incisions can be used (Fig. 7.7), and the lens is positioned in the ciliary sulcus, over the intact anterior capsule. Silicone lenses, as previously stated, should not be used because they have severe condensation problems
during fluid-air exchange, have higher posterior capsular opacification rates, and absorb silicone oil. Multipiece (three-piece) foldable acrylic lenses are preferable in the sulcus to single-piece lenses, because the thickness of the haptics in the latter might rub against the posterior iris and cause postoperative iritis and pigment dispersion.
short length of tubing to a 5-mL syringe operated by the assistant is used for this step (Fig. 7.4). If endocapsular lensectomy is attempted with the 25-gauge cutter without the fragmenter, hydrodissection can be performed with a 27-gauge needle advanced through the 25-gauge cannula to the edge of the posterior capsulectomy. Sculpting without nuclear cleaving or rotation is then initiated at the temporal margin of the nucleus to avoid damaging the capsule with the fragmenter. The Alcon 20-gauge, four-crystal fragmenter is used to sculpt the nucleus, epinucleus, and finally the cortex (Fig. 7.5). This fragmenter has the same ultrasonics as the Legacy. The anterior cortex is avoided to prevent
damaging the anterior capsule. The vitreous cutter is used for aspirating the remaining cortex. The vitreous cutter is better than classic irrigation/aspiration (I/A) tools because of the cutting capability that acts like chopping. The anterior capsule is polished after aspirating the cortex (Fig. 7.6). Almost any posterior chamber lens could theoretically be utilized, but foldable lenses offer the advantage of a smaller incision. The hydrophobic foldable acrylic multipiece lens (Alcon Acrysof) is currently being utilized because of the low incidence of capsular opacification. Scleral tunnel or clear cornea incisions can be used (Fig. 7.7), and the lens is positioned in the ciliary sulcus, over the intact anterior capsule. Silicone lenses, as previously stated, should not be used because they have severe condensation problems
during fluid-air exchange, have higher posterior capsular opacification rates, and absorb silicone oil. Multipiece (three-piece) foldable acrylic lenses are preferable in the sulcus to single-piece lenses, because the thickness of the haptics in the latter might rub against the posterior iris and cause postoperative iritis and pigment dispersion.
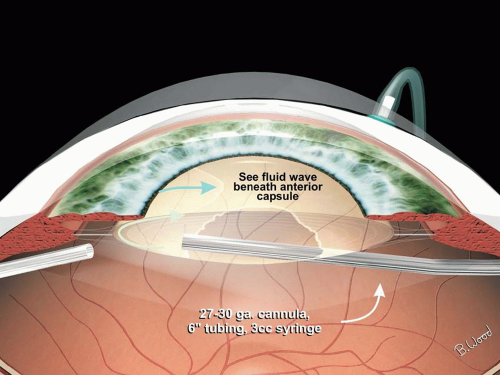 Figure 7.4 ▪ Cortical cleaving hydrodissection is performed with a blunt 27-gauge cannula attached to a 3- to 5-mL syringe via short length of tubing. |
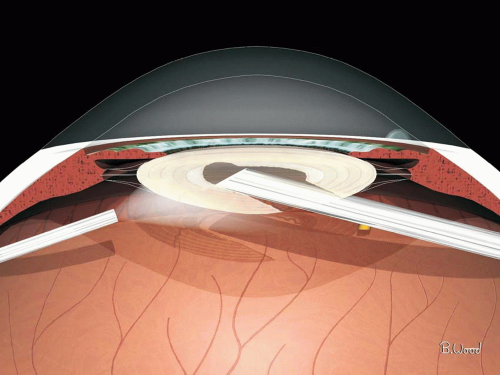 Figure 7.5 ▪ The nucleus, then epinucleus, and then cortex are sculpted with the fragmenter. |
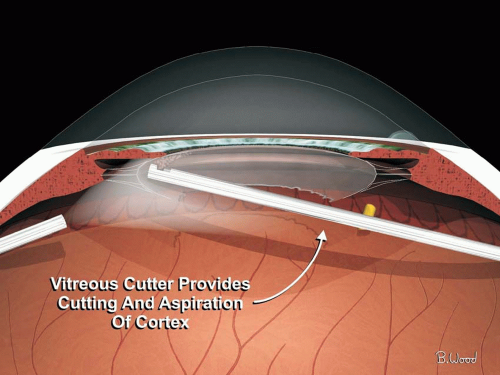 Figure 7.6 ▪ I/A is performed with the vitreous cutter so that cortex can be cut and aspirated after using gentle suction to remove from capsular bag. |
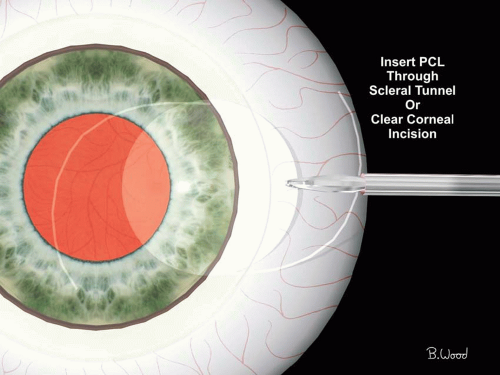 Figure 7.7 ▪ A foldable Acrysof IOL is inserted through a clear corneal or scleral tunnel incision. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


