Purpose
To survey the anatomic structures seen in the posterior vitreous using a newly developed technique, dynamic focusing and windowed averaging swept source optical coherence tomography.
Design
A cross-sectional study of subjects without a history of eye disease or posterior vitreous detachment.
Methods
A focused illumination beam was swept through the scan depth during 96 successive B-scans and the corresponding most highly resolved portion of each scan was used to make an averaged composite image. The main outcome measures were the frequency and interconnectedness of anatomic features visualized.
Results
There were 44 eyes of 25 subjects, who ranged in age from 23 to 62. An optically empty space was seen above the macula in all eyes, and corresponded to the premacular bursa. Above the optic nerve head was a conical space corresponding to the area of Martegiani. The 2 areas were interconnected in 25 cases (56.8%). Anterior to the premacular bursa was another lacuna, named the supramacular bursa, that was separate from the premacular bursa in horizontal scans centered on the fovea and was found in 38 eyes (86.4%). Both the supramacular and premacular bursae coursed anteriorly and in 21 of the 38 eyes (55.3%) were seen to interconnect.
Conclusions
The anatomic arrangement of the vitreous is consistent in living eyes with no posterior vitreous detachment, and does not correspond precisely to that described from dissection studies of autopsy specimens. The constancy of the specific findings suggests there may be some beneficial effect from the architectural structure of the vitreous that enhances evolutionary fitness.
The vitreous is the largest structure inside of the eye and fills a space between the lens and the retina. It is a composite material with water as the main component (accounting for almost 99% of the weight of the vitreous) and a sparse network of collagen fibers. Interspersed between the fibers, and acting as a shock absorber, are mucopolysaccharides, most notably hyaluran, a molecule capable of binding thousands of water molecules. The structure of the vitreous extends to larger scales beyond the molecular. Various authors have proposed that the transparent configuration of the vitreous has a complex architecture. Possibly because the vitreous is difficult to visualize, the details advocated in these proposals differ greatly.
Eisner examined living and autopsy eyes and determined that the vitreous in young people was a uniform matrix but with increasing years specific condensations of the vitreous, which he called tracts, occurred in an onion-skin pattern in the vitreous body ( Figure 1 ). In the autopsy eyes the sclera, choroid, and retina were dissected from the vitreous, which was suspended in saline solution. The vitreous of humans was considered to have a low density, so animals with a high-density homogeneous vitreous, bovines and sheep, were used to study rarefactions in the vitreous extending centripetally inward from retinal vessels. Eisner thought the Cloquet canal did not exist after regression of the hyaloidal artery and only a “hyaloid tract” remained. Worst also dissected fresh specimens and removed the sclera, choroid, and retina. Because the vitreous ordinarily has firm attachments to regions such as the vitreous base, optic nerve head, and macula, these areas are prone to damage from the dissection. Therefore Worst allowed the specimens to undergo autolysis to soften the attachments. Although he stated that “all of the enveloping structures will become putrid” by this process, the “vitreous framework is not severely affected.” Worst did not state how he knew this to be true. Once the enveloping material could be removed, specimens were injected with ink at various points inside of the vitreous body and cavities became visible, which he called either cisterns or bursae.
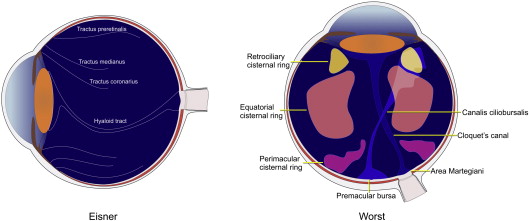
While Eisner did not describe any internal cavities in the vitreous cavity, Worst found plenty. These were arranged in a specific configuration, according to Worst; there were 72 small cisterns located behind the ciliary body, 36 medium-sized cisterns at the equator, and approximately 12 more in the posterior pole. In addition there was a large pouch-like lacuna overlying the macula, the premacular bursa. This bursa continued anteriorly through a narrow tube-like structure called the canalis ciliobursale. Over the optic nerve was an absence of formed vitreous called the area of Martegiani. Worst thought remnants of the Cloquet canal could persist after regression of the hyaloid artery that continued anteriorly from the area of Martegiani through the vitreous cavity. The premacular bursa was separated from the area of Martegiani by the “septum papillo-maculare.” All cisterns and bursae had the potential to intercommunicate in the central vitreous by an undisclosed architecture. Kishi and Shimizu fixed autopsy eyes, bisected them, and then dropped fluorescein dye onto the bisected eyes. After rinsing the vitreous, they examined the results. They identified a premacular bursa in all 48 of eyes examined with no posterior vitreous detachment, some of which were as young as 2 years old. They also reevaluated the pathophysiology of tractional states on the macula based on this information and renamed the bursa the posterior precortical vitreous pocket. Sebag and Balazs emphasized the fibrillar nature of the vitreous in their work. They dissected autopsy eyes and many of their examples show a large premacular hole with posterior herniation of vitreous fibers. They did not demonstrate cisterns, bursa, or Cloquet canal in the posterior portion of the vitreous.
While dissection has been the mainstay of obtaining anatomic information for millennia, there was a lack of a way to independently confirm dissection studies of a structure that is very delicate or potentially prone to change while surrounding structures become “putrid.” It is possible that a noninvasive imaging modality would avoid the high likelihood of artifactual damage to the vitreous structure during dissection. Contact B-scan ultrasonography can visualize some aspects of the vitreous cavity, but ocular ultrasonography has low resolution. Optical coherence tomography (OCT) has much greater resolution but faces several important limitations in imaging the vitreous. A method to improve visualization of the vitreous using a technique based on swept source (SS) OCT has been developed that uses dynamic focusing and windowed averaging. This method provides a longer range of vitreous imaging than previously used methods and allows undisturbed visualization of the vitreous anatomy in vivo. In this study swept source OCT with dynamic focusing and windowed averaging obtained novel views of the vitreous in healthy subjects, and the findings appear to have important consequences.
Methods
Derivation of Technique
SS OCT is inherently suited for vitreous imaging because the sensitivity roll-off is much lower than comparable spectral-domain OCT instruments. Therefore a high sensitivity can be maintained across a larger range. There are still problems to contend with in vitreous imaging, even with SS OCT. The illumination beam of the OCT instrument is relatively defocused in the vitreous cavity, the signal produced by the vitreous is low, and the ratio of signal produced by the vitreous is very small in proportion to that produced by the retina, making the display of both in a grayscale image difficult. In crafting a solution to the problem of vitreous imaging, each of these elements will be discussed in turn.
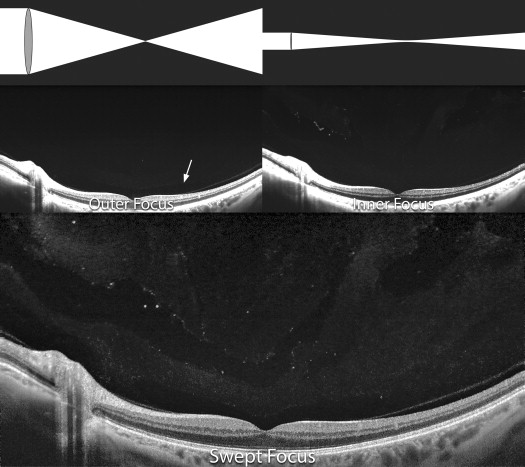
The smallest spot produced by an illumination system is inversely related to its numerical aperture; large numerical aperture systems can focus light to a smaller spot than low numerical aperture systems ( Figure 2 ). Having a smaller spot increases the potential lateral resolution, but because of the cone angle the scan depth that can be imaged is limited and the working distance is reduced. The illumination systems of OCT instruments have a fairly low numerical aperture. This produces a narrow beam over a long range, but the beam does not focus to a sharp point. Lateral resolution is sacrificed in order to gain increased working depth. Even so, the diameter of the beam is larger at the top and bottom of the scan range than it is in the center. The narrowest part of the illuminating beam is typically placed near the center of the scan, a location where the vitreoretinal interface is often imaged. The vitreous anterior to this is illuminated by a relatively defocused part of the beam and consequently provides a less detailed image ( Figure 2 ). In addition, the amount of light any particle in the beam of light reflects back to the detector is related to the proportion of area of the illuminating beam the particle occupies. Consequently a particle reflects less light back when placed in the defocused beam in the anterior vitreous, as compared with a similar-sized particle at the center of the scan width. If the beam could be focused on the more anterior vitreous, the signal strength and resolution would be improved there. This would come at the price of decreased resolution of the preretinal vitreous and structures further posterior. However, if the beam could be dynamically focused successively in planes through the eye, each zone would be selectively visualized in an optimized way. Since the location of the best beam focus is known, that portion of the image could be selected to produce a final image that relies on averaging to improve the signal-to-noise ratio. In the current implementation the beam is actively focused and a limited region, or window, of the scanned region from 96 scans is selected to construct the image. This is called dynamic focusing with windowed averaging. Since swept source OCT is very fast, the whole process can be accomplished in a fraction of a second. This process is analogous to focus stacking used in microscopy, but it is accomplished automatically in a fraction of a second during the OCT scanning process.
The resultant image still has a great disparity between the signal strength from the vitreous as compared with the retina. Using conventional scaling of the image, if the vitreous were brightened to improve visualization the retina would be too bright; and if the grayscale range was selected to optimally display the retina, the vitreous would look very dark. The human visual system has a limited dynamic range in which grayscale values can be perceived. To compensate for this local contrast adjustment, algorithms can be employed. One of the more common types is adaptive histogram equalization. In this method, local regions of an image are transformed in brightness according to a selectable neighborhood of local pixel values. This constructs numerous histograms for 1 image; or to state it in another way, local image gain is varied according to the cumulative distribution function of the region. There are methods such as contrast-limited histogram equalization, which limits the maximal gain in darker regions to reduce the amount of noise produced in the image. Variations of this technique are used in image processing programs such as Adobe Photoshop (Adobe Photoshop cc, version 14.2; Adobe Systems Incorporated) and ImageJ (ImageJ version 1.48u National Institutes of Health with Contrast Limited Adaptive Histogram Equalization plug-in, available at http://rsb.info.nih.gov/ij/plugins/clahe/index.html ). With this technique the appearance of the retina and choroid are not substantively altered.
Patients and Scan Strategies
The eyes evaluated were all from normal subjects who volunteered to be imaged. All subjects signed a written informed consent about the imaging and the study participation and the study had institutional review board approval through the Western Institutional Review Board. Exclusionary criteria included any history of eye disease, myopia greater than 6 diopters of spherical equivalent, or any media opacity potentially obstructing proper visualization of the vitreous. The base instrument used, the Topcon DRI-1 (Topcon Medical Systems), is an OCT instrument in which the light source has a bandwidth of 100 nm and a center wavelength of 1050 nm, and performs 100 000 A-scans per second. The implemented dynamic focus function has a range that is selectable by the user but typically occupies the range of the scanned region, which is 2.6 mm. The averaging algorithm used by the DRI-1 does not work on an image solely of the vitreous, but works if there is about 0.5 mm of retina at the bottom of the image. This leaves slightly more than 2 mm of vitreous that can be imaged above the retina. This compares favorably with other instruments. For example, the Heidelberg Spectralis images 40 000 A-scans per second and the total scan depth is only 1.9 mm. To improve the signal-to-noise ratio the images are averaged on a selective basis. The resolution of the resultant OCT images is high, provided that structures do not move from 1 image to the next during the averaging sequence. Residual motion of the vitreous is evident as arcuate trails associated with bright points and a decrease in image sharpness.
Every patient had a horizontal and vertical 12 mm scan over the macula and an additional 12 mm vertical scan intersecting the fovea while the patient looked upward. Not every patient volunteered to have both eyes imaged. This scan was centered approximately at the superior arcades. The images were evaluated for the presence and anatomic arrangement of lacunae in the vitreous. In particular, the premacular bursa and the area of Martegiani were evaluated. A 12 mm vertical scan was used to identify a narrow hyporeflective structure consistent with the Cloquet canal. Additional bursae were catalogued when present. The resultant images were processed using local contrast enhancement techniques as described in the Derivation of Technique section. Data were analyzed with descriptive statistics, and to evaluate relationships between the vitreous anatomic findings and age, generalized estimating equations were used. A P value less than or equal to .05 was considered significant. The IBM SPSS version 21 statistical package was used (IBM Corporation).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


