Purpose
To assess the efficacy of scanning laser ophthalmoscopy in the retro mode, employing a new dark-field aperture, for detecting laser spots created by subthreshold diode laser micropulse photocoagulation.
Design
Interventional case series.
Methods
setting: Institutional. patients: Eight consecutive patients (8 eyes) with clinically significant diabetic macular edema and 1 patient (1 eye) with macular edema attributable to branch vein occlusion underwent subthreshold diode laser micropulse photocoagulation. Scanning laser ophthalmoscopy images were obtained before and immediately after subthreshold laser photocoagulation. Application of the laser was done under 3 different sets of conditions with a 15% duty cycle for 0.2 seconds in the micropulse mode: condition I was 200-μm spots at 200% of the threshold power in the continuous wave mode, condition II was 200-μm spots at 300%, and condition III was 125-μm spots at 250% or 300%. The laser-treated area was monitored on both color images and by scanning laser ophthalmoscopy (F-10, NIDEK, Gamagori, Japan).
Results
Immediately after subthreshold laser photocoagulation, there were no obvious laser scars affecting the treated area in any of the patients on color images. Scanning laser ophthalmoscopy with a diode laser in the retro mode showed no obvious changes after treatment under condition I. However, conditions II and III resulted in dark spots at the sites where the laser had been applied in 5 out of 7 patients.
Conclusions
Scanning laser ophthalmoscopy in the retro mode is useful to detect sites of subthreshold micropulse laser application. The dark spots detected by retro mode scanning laser ophthalmoscopy are probably related to swelling of the pigment epithelium after laser application. This method is useful to confirm the invisible spots created by subthreshold diode laser micropulse photocoagulation.
Diabetic macular edema is one of the most important causes of impaired vision and legal blindness. In 1985, the Early Treatment of Diabetic Retinopathy Study showed that macular focal laser photocoagulation could significantly improve moderate visual loss attributable to macular edema. However, complications such as progressive enlargement of laser scars, subretinal fibrosis, and subretinal neovascular membrane have been reported, resulting in the occurrence of scotoma and loss of color vision. Therefore, a less invasive treatment strategy has been advocated in order to reduce the laser energy applied and avoid tissue damage.
In 1997, Friberg and associates first reported on the clinical application of subthreshold diode laser micropulse photocoagulation for diabetic macular edema. This method is designed to target the retinal pigment epithelium, while having a minimal effect on the sensory retina and choroid. Accordingly, frequent short laser pulses of subthreshold intensity are applied to the region of the retina affected by macular edema. Several clinical studies have subsequently demonstrated the efficacy of this method. One of the difficulties with performing this treatment is the inability to see the laser lesions that are created, which means surgeons are unable to confirm whether or not treatment is adequate. Optical coherence tomography (OCT) is a method that can be employed to assess the outcome of this treatment, but the change in macular thickness is only detectable several weeks after laser therapy. Therefore, a technique for visualizing laser spots immediately after treatment is needed.
In 2002, Framme and associates reported that spots created by subthreshold diode laser micropulse photocoagulation showed increased fundus autofluorescence. Accordingly, this study was performed to investigate whether retro mode imaging with a new SLO machine (F10) was able to detect subthreshold diode laser micropulse photocoagulation laser spots.
Patients and Methods
Nine patients were treated with subthreshold diode laser micropulse photocoagulation after informed consent was obtained.
Inclusion criteria were mild or moderate nonproliferative diabetic retinopathy or early proliferative diabetic retinopathy with clinically significant macular edema (ETDRS criteria) involving the center of the macula, or macular edema associated with branch vein occlusion.
Exclusion criteria were as follows: a foveal thickness of more than 600 μm; best-corrected Snellen visual acuity (BCVA) of less than 0.1; subfoveal hard exudates; prior vitrectomy; cataract surgery or intraocular surgery within 3 months before this study; and intravitreal injection of triamcinolone acetate or macular laser photocoagulation within 6 months before this study. Patients on hemodialysis were also excluded.
All treatments were performed by a single surgeon. An 810-nanometer diode laser photocoagulation device (Iris Medical OcuLight Slx; Iridex Corporation, Mountain View, California, USA) was used in the MicroPulse operating mode.
Laser light was delivered via a slit-lamp adapter. Micropulse laser photocoagulation was performed with a 3-mirror contact lens and the region of thickened macula that showed diffuse fluorescein leakage was treated. The subthreshold laser power was determined in each patient by creating a threshold burn with the lowest energy required to make a visible “test burn” at a site without retinal edema outside the vascular arcade. Subthreshold burns were then applied at a lower energy level in the micropulse mode, with application of confluent laser spots up to 500 μm from the center of the fovea. Closure of microaneurysms was not attempted.
The test burn was done with continuous-wave laser energy (100% duty cycle) for 0.1 second at a diameter of 200 μm. Then laser spots were applied with a 15% duty cycle in the micropulse mode at 200% or 300% of threshold energy (520-1000 mW) for 0.2 seconds.
The following 3 protocols for laser energy application were tested: condition I was 200-μm spots at 200% of threshold energy, condition II was 200-μm spots at 300% of threshold, and condition III was 125-μm spots at 250% or 300% of threshold. The total energy was calculated as follows: E(J) = P(W)×T(sec) = P(W)×0.1 sec. Subthreshold energy was P(W)×200%×0.2×15% = P(W)×0.06 under condition I and P(W)×300%×0.2×15% = P(W)×0.09 under condition II. Therefore, the total energy applied was 60% of the threshold level under condition I and 90% of threshold under condition II. Accordingly, the subthreshold energy was P(W)×250%×0.2×15% = P(W)×0.075 and P(W)×300%×0.2×15% = P(W)×0.09 under condition III. Since the spot size was smaller (125 μm), the energy was adjusted in proportion to spot size, so the total energy was respectively 192% or 230.4% under condition III.
Color pictures were taken before and immediately after laser micropulse photocoagulation with a fundus camera (Topcon, Japan). Scanning laser ophthalmoscopy (SLO) images were obtained with an F-10 (Nidek Co, Gamagori, Japan) at baseline, immediately after laser therapy, and 1 week afterward. SLO pictures and fundus autofluorescence images were taken with a fundus camera (F-10 SLO; Nidek Co) before laser treatment and soon after treatment.
The F-10 is a new SLO apparatus that obtains images of the deeper retinal layers with a 790-nm infrared laser. This machine has 4 different wavelengths and 8 apertures (5 stops), including a new retro mode aperture, which is a laterally oriented oval-shaped opening with a central stop ( Figure 1 ). It is a modification of the dark-field (indirect) mode, which can detect multiple reflections of scattered light from retinal tissue through a ring-shaped aperture ( Figure 1 ). With a conventional ring aperture, the fundus camera receives light from multiple directions. In contrast, the retro mode detects scattered light from only 1 direction through the laterally oriented opening and the other side of the light pathway is blocked. This blocking of the back reflection creates a shadow-like image. The scattered light that passes through the laterally oriented aperture not only allows deeper retinal structure to be visualized, but also creates shadows and thus produces a pseudo-3-dimensional image.

In this study, imaging in the retro mode was done via 2 different apertures, which were directed to the right or left side of the apparatus. Changes of macular findings in the treated area were monitored on both color fundus photographs and images obtained with the F-10.
Foveal macular thickness and macular volume were measured by optical coherence tomography using an OCT 3000 (Zeiss Humphrey Instruments, Dublin, California, USA).
Results
Demographic Data and Baseline Characteristics
Eight patients (9 eyes) with type II diabetes and clinically significant macular edema and 1 patient (1 eye) with macular edema attributable to branch vein occlusion were treated with subthreshold diode laser micropulse photocoagulation. There were 7 men (8 eyes) and 1 woman (1 eye), aged from 37 to 74 years (average: 60.2 years).
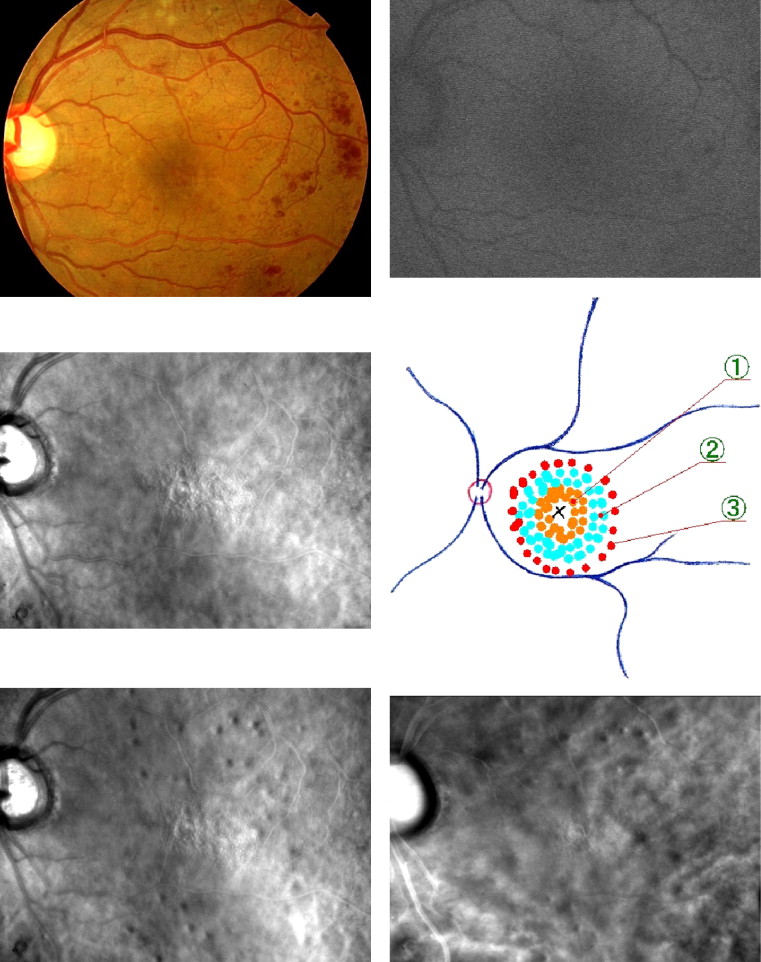
Immediately after laser treatment, there were no obvious laser scars at the treated sites in any of the patients on color images. There were no changes on fundus autofluorescence images after subthreshold diode laser micropulse photocoagulation under any of the 3 sets of conditions. SLO images also showed no changes with condition I. However, the retro mode revealed dark spots at sites where the laser had been applied in 5 out of 7 eyes with condition II. With condition III, dark spots were observed in 2 of 2 eyes. Using the left aperture, the dark spots revealed by retro mode imaging had a lighter zone on the left side and a darker zone on the right side, creating a shadow-like appearance. In contrast, the darker zone was on the left side and the lighter zone was on the right side when the aperture on the right was used ( Figure 2 ). After 1 week, dark spots were no longer observed in 2 patients.
Case Report
A 37-year-old man with a 7-year history of type II diabetes was referred for evaluation of diabetic retinopathy. Funduscopic examination showed very severe nonproliferative retinopathy, so panretinal photocoagulation was done for both eyes. Six months later, diffuse diabetic macular edema occurred in the left eye, so subthreshold diode laser micropulse photocoagulation was performed. Preoperative examination showed diffuse diabetic macular edema with mild cystoid macular edema. Fluorescein angiography revealed diffuse dye leakage with cystoid changes in the macular region and mild capillary dropout in the perifoveal area. OCT revealed a cystoid space at the foveal region and a small amount of subfoveal fluid. The patient’s foveal thickness was 538 μm and his visual acuity was 20/40.
Prior to surgery, color pictures and SLO images were obtained. In the retro mode numerous cystoid spaces were revealed. Fundus autofluorescence images were also obtained, as were SLO images with a standard confocal aperture. At 60 minutes after SLO, the region of macular edema was treated by subthreshold micropulse diode laser photocoagulation. The laser was applied with a 15% duty cycle and a 200-μm spot size for 0.2 seconds at 200% of threshold power (640 mW) in the continuous-wave mode, creating 2 circles of laser spots in the area surrounding the foveal region. Then a further 2 circles of 200-μm spots were created at 300% of threshold power (960 mW) outside this first treated area. Subsequently, 125-μm spots at 250% of threshold energy (800 mW) were applied outside the second treated area. At 18 minutes after laser ablation, color images and SLO images were obtained again. There were no obvious laser spots on any of the color photographs. There were also no changes and no laser spots on the fundus autofluorescence images. With the standard confocal aperture, SLO revealed no differences between before and after the laser procedure. However, images obtained in the retro mode revealed several dark spots at the sites where the laser had been applied. The dark spots were mainly seen at sites treated at 300% of threshold power or where 125-μm spots were created at 250% of threshold. The spots were composed of a dark crescent and a lighter part, and appeared to represent shadows cast by small swollen areas. The spots were more prominent with the left-sided opening than the right-sided one. One month after subthreshold micropulse diode laser photocoagulation, the foveal retinal thickness was decreased to 406 μm. No spots were seen on color images at 6 months after laser treatment. Visual acuity was maintained at 20/40 ( Figure 2 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


