The Vibrant Soundbridge is the world’s most often implanted active middle ear implant or hearing aid. During the last few years, the device indications have expanded from sensorineural hearing loss to conductive and mixed hearing loss. Titanium couplers have led to improved contact of the floating mass transducer with the middle ear structures. The resulting hearing gain is satisfying for most patients, but so far, there is no clear audiologic advantage over conventional hearing aids. Currently, the indications are mainly related to intolerance of conventional hearing aids (eg, chronic otitis externa), severe mixed hearing loss with a destructed middle ear and certain medical diagnosis (eg, congenital atresia).
Key points
- •
There is growing evidence for the effectiveness and safety of the VSB in patients with conductive and mixed hearing loss.
- •
The indications for implantation of a VSB are primarily related to intolerance of a CHA.
- •
A wide range of FMT coupling methods have been developed, which may result in similar acoustic outcomes.
- •
Complications are rare and mainly related to insufficient functional hearing gain with the need to reposition the FMT in the round window niche.
- •
Studies indicate that the VSB can provide functional hearing gains at least as good as those achieved with CHA.
Introduction
The Vibrant Soundbridge (VSB; Med-El, Innsbruck, Austria) is a partially implantable active middle ear transducer system. Since its introduction into clinical practice about 15 years ago it has become the world’s most often used active middle ear implant. The outer component of the VSB, comprised of a microphone, audio processor, battery, transmitter coil, and magnet, processes incoming acoustical signals to an amplitude-modulated signal and delivers these transcutaneously to the inner VSB component. The inner component, or vibrating ossicular prosthesis (VORP), is comprised of an antimagnet, receiver unit, conductor link, and the floating mass transducer (FMT). The inner component is manufactured with a left- and right-sided version. After the signal is received and demodulated, it is sent to the FMT via the conductor link. The FMT is the core technology and key component of the VSB. It consists of a titanium housing with a coil and a magnet in close physical proximity to one another. In a set of biasing elements, the magnet and housing vibrate relative to one another, thus causing vibrations in direct response to the externally generated electric signal. When the FMT is attached to a mobile structure (ossicles, inner ear window) these vibrations can be transferred and the target organ (cochlea) is stimulated. Hence, instead of acoustic energy, the VSB delivers mechanical energy to the cochlea, stimulating the inner ear fluids.
The VSB was originally designed in the late 1990s solely for patients with sensorineural hearing loss. For this purpose, the FMT is coupled to the incus’ long process via a small titanium clip. Analyzing the audiometric results of the first clinical trial it was found that the VSB could “also be used to treat conductive hearing loss.” The versatile possibilities of the surgical placement of the device because of its single anchor point attachment to the middle ear helped to explore alternative coupling methods for the FMT (length of 2.3 mm, diameter of 1.6 mm, mass weight of 25 mg), and with these, the application of the VSB has expanded to patients with conductive and mixed hearing loss.
Introduction
The Vibrant Soundbridge (VSB; Med-El, Innsbruck, Austria) is a partially implantable active middle ear transducer system. Since its introduction into clinical practice about 15 years ago it has become the world’s most often used active middle ear implant. The outer component of the VSB, comprised of a microphone, audio processor, battery, transmitter coil, and magnet, processes incoming acoustical signals to an amplitude-modulated signal and delivers these transcutaneously to the inner VSB component. The inner component, or vibrating ossicular prosthesis (VORP), is comprised of an antimagnet, receiver unit, conductor link, and the floating mass transducer (FMT). The inner component is manufactured with a left- and right-sided version. After the signal is received and demodulated, it is sent to the FMT via the conductor link. The FMT is the core technology and key component of the VSB. It consists of a titanium housing with a coil and a magnet in close physical proximity to one another. In a set of biasing elements, the magnet and housing vibrate relative to one another, thus causing vibrations in direct response to the externally generated electric signal. When the FMT is attached to a mobile structure (ossicles, inner ear window) these vibrations can be transferred and the target organ (cochlea) is stimulated. Hence, instead of acoustic energy, the VSB delivers mechanical energy to the cochlea, stimulating the inner ear fluids.
The VSB was originally designed in the late 1990s solely for patients with sensorineural hearing loss. For this purpose, the FMT is coupled to the incus’ long process via a small titanium clip. Analyzing the audiometric results of the first clinical trial it was found that the VSB could “also be used to treat conductive hearing loss.” The versatile possibilities of the surgical placement of the device because of its single anchor point attachment to the middle ear helped to explore alternative coupling methods for the FMT (length of 2.3 mm, diameter of 1.6 mm, mass weight of 25 mg), and with these, the application of the VSB has expanded to patients with conductive and mixed hearing loss.
Candidacy for surgery
The first implantation of a VSB for sensorineural hearing loss was performed in 1996. After alternative coupling methods were discovered, the VSB is now also used to rehabilitate patients with conductive and mixed hearing loss.
Currently, there is no clear evidence that the VSB is superior to conventional hearing aids (CHA) in functional qualities, such as hearing gain or threshold improvement. Furthermore, there is large variance in the functional gain obtained in different patients, suggesting high variability in the effectiveness of the FMT coupling. Hence, the implantation of a VSB cannot be indicated solely from the audiometric results, and currently the indications are mainly of a medical or cosmetic nature. Thus, if a patient has an indication for a CHA, but the application of this is not possible because of medical reasons, such as chronic external otitis or intolerance of an ear mold, then the VSB is a recommendable option for hearing rehabilitation.
In most cases of conductive hearing loss, a VSB is implanted into patients with a history of chronic otitis media with or without cholesteatoma. Normally, the VSB is only considered after conventional tympanoplasty and ossiculoplasty with a partial or total middle ear prosthesis has failed (ie, if application of a conventional middle ear prosthesis has not led to a satisfactory hearing result).
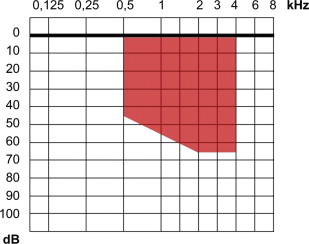
Although not a decisive indication parameter, audiologic prerequisites do exist for VSB candidates. For patients with conductive or mixed hearing loss, the bone conduction should not be worse than 45 to 65 dB within the frequencies 500 to 4000 Hz as recommended by the Med-El company ( Fig. 1 ). There is not a speech discrimination criterion for the implantation of a VSB, but functional hearing outcome depends on this parameter. Although patients with a poor preoperative discrimination score of less than 40% (unaided) may show improvement with the VSB, patients with a discrimination score of 50% to 70% and higher are likely better candidates and long-term performance is likely to be better. If there is a near normal hearing threshold on the contralateral ear, then this may influence the acceptance of a VSB, because some of these patients will not report a high subjective benefit. Hence, the indication of a VSB for unilateral hearing loss should be discussed individually.
Whether or not a VSB should be implanted in children, is open for debate. Since 2009, the VSB has approval in Europe for patients younger than 18 years. Following a statement by an international consensus paper the VSB has already been implanted in newborns. Because the middle ear structures are fully developed at the time of birth and because the VSB uses a single-point attachment in the middle ear, patient growth is not expected to change the VSB performance over time. However, the limitations for a postimplant magnetic resonance imaging (MRI) scan are more restrictive in children, and it is recommended to carefully weigh the pros and cons of the VSB against all alternative therapies before implantation in children. Preconditions for VSB implantation as recommended by the authors are listed in Table 1 .
| Preconditions for VSB Implantation | Comment |
|---|---|
| Suitable audiometric performance with bone conduction within the designated zone (see Fig. 1 ) | Indication zone is different for patients with sensorineural hearing loss |
| Stable inner ear function | Definition unclear |
| Either no benefit from CHA or no possibility to wear these | Severe malformations of the outer ear, recurrent external otitis and otorrhea, intolerance of the ear mold, and so forth |
| Exclusion of cholesteatoma; no signs of acute inflammation in the middle ear | Risk for labyrinthitis, risk for revision surgery, and so forth |
| Magnetic resonance imaging of the brain (optional) | Scan for cerebral pathologies before surgery because application of this imaging technique is limited after VSB implantation |
| High-resolution computed tomography of the temporal bone (optional) | Scan for cholesteatoma presence or signs of malformations |
| Acceptable language skills | Important for accommodation and tuning of audio processor |
| Realistic expectations of the hearing benefits | Final hearing result is not predictable |
| Psychological and emotional stability |
The VSB has been implanted in patients with congenital microtia or ear canal atresia. It is wise to not combine VSB implantation with reconstructive surgery of the auricle or the external ear canal at the same time because the latter suffers from a significant rate of complications, which may harm the functionality of the VSB. However, for those patients suffering from pure conductive hearing loss, bone-anchored hearing aids are the first option because they are easier to apply, not putting the middle ear structures and inner ear function at risk during implantation and because they yield similar functional results.
At the authors’ institution, children are initially offered a nonsurgical solution with a soft-band bone conduction hearing aid, which has proved its effectiveness. Currently, in adults, acceptance of bone-anchored hearing aids has improved after the introduction of a transcutaneous signal delivering (BoneBridge [Med-El, Innsbruck, Austria]), which renders the presence of a percutaneous fixture requiring daily cleaning and maintenance unnecessary.
Preoperative planning and preparation
Some precautions must be considered before a VSB implantation. Patients being considered for implantation of an active hearing implant should have stable bone- and air-conduction thresholds. However, a generally accepted definition for “stable auditory thresholds” does not exist. A bone-conduction threshold not having deteriorated more than 15 dB in two consecutive frequencies within 12 months before implantation is suggested by the authors.
Pure tone audiometry with appropriate masking and speech audiometry are highly recommended diagnostic tools before a VSB implantation. If the hearing performance cannot be determined with sufficient certainty by subjective audiometry, then objective audiometry (eg, auditory brainstem responses) is mandatory. Unlike the situation with passive middle ear prostheses for ossiculoplasty, tympanometry plays no key role for the VSB because its function is independent of the middle ear aeration. The testing of stapedial reflexes is reserved for specific cases, such as patients with otosclerosis where a VSB is implanted together with a stapes piston.
Before a VSB implantation, a high-resolution computed tomography of the temporal bone is recommended to check the correct position of the anatomic structures of the inner ear, middle ear, and mastoid and to estimate the thickness of the parietal skull bone. Normally, VSB implantation is preceded by some sort of middle ear surgery with surgical exploration of the ear, and thus the intraoperative status of the ear is known to the surgeon. In these cases a new computed tomography scan is normally not necessary. Because most of the patients underwent several previous middle ear surgeries, earlier procedures must be respected and prior surgery reports should be collected and studied beforehand.
Because an implanted VSB limits MRI of the brain, it might be advisable to scan for cerebral pathologies, if suspected, before VSB implantation. Although studies have shown that MRI examinations of up to 1.5 T likely do not present a serious risk of harm to the patient or damage to the VSB, a dislocation of the FMT is possible during MRI, and also image artifact will occur.
A VSB should only be implanted in ears with no active inflammation and no cholesteatoma. If cholesteatoma disease can be completely removed without concern of recurrence, then it is, in principle, possible to perform the eradication of the disease and the implantation of a VSB in one surgical session. However, a two-stage concept is probably used more often, where the initial cholesteatoma surgery with ossiculoplasty is done first. If this attempt fails because of insufficient hearing gain, and if CHA are not desired or tolerated, then active middle ear implants become a reasonable option.
Further preparations are similar to other middle ear and temporal bone surgery (eg, routine blood examination). Naturally, the patient should be thoroughly informed about the device, its mode of operation, visual nature, and its potentials and limitations. Informed consent must be obtained from the patient before surgery where additional to common risks at middle ear surgery, the points of dependence of an external component, possible technical failure of the device, insufficient hearing gain, and MRI limitations should be discussed.
Regarding the required materials, it is advisable to have a backup implant available for the operation, which can be used if the first implant turns out to be defective or damaged during surgery. All commercially available titanium couplers for the VSB (clip or bell coupler for the stapes, TORP, or oval window [OW] coupler and round window [RW] coupler) should be on hand for the surgery, even if their use is not expected.
A VSB may be implanted bilaterally, but it is recommended to verify the acceptance and functional gain at one side (preferably the ear with the worse hearing) first and then have the other ear implanted in a separate second surgery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


