Vascular Hamartomas, Hyperplasia, and Neoplasms
This chapter includes an array of vascular tumors resulting from new formation of vessels, proliferation of tissue components of the vessel wall, and hyperplasia of cellular elements ordinarily concerned with the genesis of vascular tissue. These vasculogenic lesions comprise the largest group of primary orbital tumors in our survey. We realize that, in the past, two of the groups (capillary and cavernous hemangiomas) have been considered as phases of the same tumor, the former being a predecessor for the latter. However, on the basis of their differing ultrastructural makeup and their distinctive clinical aspects, it is now obvious that they should be considered separate tumors, a format not followed in prior editions of this text. The literature has not been as active in this area of orbital tumefaction as in other areas; however, there have been some noteworthy publications. Harris (1999), writing on behalf of the Orbital Society, framed the issue of “vascular malformations” on the basis of their hemodynamic features. This is particularly germane to lymphangiomas and varices, which will be considered later in this chapter. The vascular malformations, which are tumefactions based on established vascular channels, will be reviewed in the next chapter.
Capillary Hemangioma
Synonyms for this cellular tumor are infantile hemangioma, hypertrophic hemangioma, cellular hemangioma, juvenile hemangioma, angioblastic hemangioma, and benign hemangioendothelioma. There is strong evidence that some are hamartomatous because of their presence at birth and their association with an enlarged orbit. These signs indicate their perinatal development. This hamartogenesis could reasonably be extended to the orbital lesions that so commonly commence in the first 2 months of life. However, those capillary hemangiomas, surgically verified in older children and adolescents, are more likely to be true neoplasms. Regardless of how these are classified, there have been two interesting papers regarding pathogenesis with reference to the placenta. Burton et al. (1995) noted that there was a threefold higher incidence of hemangiomas in a group of infants exposed to transcervical chorionic villus sampling when compared to the incidence in the amniocentesis group, which approximated the incidence in the general population. From the group of 432 returned questionnaires it was found that all the hemangiomas were cutaneous with the exception of one laryngeal hemangioma. It was not readily apparent why this was so. The life cycle of an infantile hemangioma was noted to have similarities to a placenta in that there is a perinatal presentation, rapid growth, and eventual involution. (North et al., 2002) discovered similarities involving the vasculature and the tissue-specific markers between an infantile hemangioma and a placenta. The authors postulated two potential mechanisms for a placenta-hemangioma connection. The first was a somatic mutation or abnormal local inductive influence, giving rise to the hemangioma but the second more intriguing hypothesis was that placental tissue might embolize and give rise to the hemangioma. This might also serve as an explanation for a higher incidence of hemangioma after chorionic villus sampling as described in the preceding text.
Incidence
First, we should emphasize that our series of 34 capillary hemangiomas were located, all or in part, posterior to the orbital septum. Therefore, our incidence data will differ from other surveys that follow the common practice of analyzing adnexal (eyelids, caruncle, and upper face) and orbital capillary hemangiomas together. We will note in the following text some of the features that distinguish the orbital lesion from the kindred tumors that are solely confined to the eyelids and upper face.
Tables 3.1, 3.2, 3.3 and 3.4 record the data pertinent to orbital capillary hemangioma. This tumor comprises 1.9% (34 out of 1,795 cases) of our total series in which the sex incidence and the laterality are equal. It is not only the most common tumor in the first decade but also in the first year of life. In the patient population aged 15 years or less, it is the third most common tumor (30 out of 213 cases, 12.7%). The age of onset is 2 months of age or less in 26 out of 34 cases, 76%, including 8 neonates (24% of the total) with tumors present at birth. Of the eight patients, who are older than 2 months of age at the time of onset, the age range is 4 months to 26 months. The age of presentation in this group varied greatly, reflecting the rapidity of growth and the degree of parental concern. In 27 out of 34 patients (79%), the tumor was palpable in the anterior orbit with or without some extension into the substance of the eyelid. In the seven remaining cases (21%), the tumor was located in the retrobulbar space and could not be palpated. In 8 out of 34 cases (24%), the tumors were located in one of the inferior quadrants of the orbit; in the others they were located in one of the superior orbital quadrants.
Two other surveys of this subject should also be noted (Haik et al., 1979, 1994). In the earlier paper, the authors had studied the clinical records of 101 patients with capillary hemangiomas of the eyelid, upper face, and eyebrow in addition to orbital lesions. The general thrust of their incidence data was similar to our series except for the sex ratio. In their series, there was a preponderance of women in a ratio of 3:2, whereas in our series the ratio was equal. Other publications based on a smaller number of cases also stress the prevalence in girls. Inclusion of hemangiomas in nonorbital sites such as the eyelid, eyebrow, and upper face in the reports of Haik et al. (1979) and others may account for the slight difference in the above sex ratios. The second paper (Haik et al., 1994) was an extensive literature review that does not change any of the comments mentioned in the preceding text.
Clinical Features
The principal presenting feature of capillary hemangioma in the anterior orbit of an infant is a unilateral, enlarging, painless, compressible swelling of the overlying eyelid associated with displacement of the eye in a direction opposite to the position of the lesion. The swelling conceals a mass with indistinct borders behind the orbital septum. The mass becomes more distinct as it pushes forward into the eyelid (see Fig. 10.1). The swelling is bluish in color but may be purplish red if the hemangioma involves the subcutaneous tissue of the affected eyelid also. There is no proptosis as a rule. Almost invariably, the parents have noticed that the mass increases in size, and the bluish overtones become more vivid when the child cries (see Fig. 10.2). As the problem progresses, the swollen upper eyelid begins to cover the visual axis and displacement of the eye increases. The growth of the tumor may be so rapid and the soft tissue swelling so great that the eye is hidden by the time the infant is seen in consultation (Fig. 1.6).
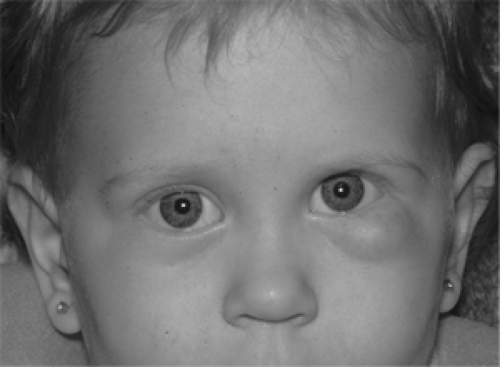 Figure 10.1 A well-demarcated, bluish capillary hemangioma in the left lower eyelid of a 17-month-old girl that was first noted at 2 months of age. Intralesional corticosteroid injections were administered at 4 months of age and 7 months of age with temporary arrest followed by regrowth of tumor. Note upward displacement of left eye due to additional tumor in left inferior orbit, confirmed by computed tomography. (See Color image.) |
The orbital teratoma is another tumor that may grow rapidly in the neonatal period. In teratoma, the eye is proptosed by the enlarging mass, but in capillary hemangioma, the eye is pushed to one side and the tumor protrudes. In the retrobulbar hemangioma of older infants and younger children, a differential diagnosis involving rhabdomyosarcoma and metastatic neuroblastoma must also be considered. The child with metastatic neuroblastoma whines and is irritable and sick. A runny nose may be present. The examination procedure annoys them, and they tend to cling to their parents possibly because of malaise and aching bones. Ecchymotic splotches are frequent in the eyelid overlying the protruding mass (Fig. 1.12).
The rhabdomyosarcoma poses a more difficult differential. The children affected by the same appear in good health, and there are no systemic or external clues that might suggest a lurking malignancy of the orbit. However, the parents often blame some putative injury for the child’s puzzling proptosis. Neither the mass nor the puffy eyelid tends to enlarge with the Valsalva maneuver. The skin of
the affected eyelid takes on a dusky red hue after several weeks’ growth of tumor, rather than the bluish tinge of the eyelid that conceals an orbital hemangioma (Fig. 1.2B) The computed tomography (CT) scans of the two tumors have similar features except that some bone erosion may be present if the rhabdomyosarcoma is localized along a bone surface. A capillary hemangioma opacifies rapidly and more profusely than rhabdomyosarcoma because of a more direct expanded arterial supply. Haik et al. (1994) mentioned that arteriography can be helpful though not in diagnosis but in managing exceptional hemangiomas by identifying the feeding and draining vessels, should ligation ever become a consideration.
the affected eyelid takes on a dusky red hue after several weeks’ growth of tumor, rather than the bluish tinge of the eyelid that conceals an orbital hemangioma (Fig. 1.2B) The computed tomography (CT) scans of the two tumors have similar features except that some bone erosion may be present if the rhabdomyosarcoma is localized along a bone surface. A capillary hemangioma opacifies rapidly and more profusely than rhabdomyosarcoma because of a more direct expanded arterial supply. Haik et al. (1994) mentioned that arteriography can be helpful though not in diagnosis but in managing exceptional hemangiomas by identifying the feeding and draining vessels, should ligation ever become a consideration.
 Figure 10.2 Capillary hemangioma in upper nasal quadrant of right orbit and eyelid in an 11-month-old girl. Crying causes the tumor to increase in size and cover eye as eyelid swells. Swelling of the right cheek reflects enlarged blood supply through external carotid system. |
Further examination of an eye displaced by an orbital capillary hemangioma will usually show a significant astigmatism when compared to the unaffected eye. The pressure of the hemangioma steepens the corneal curvature in a direction perpendicular to the axis of the astigmatism (Robb, 1977; Stigmar et al., 1978). In the older child, where some quantitative assessment of vision is possible, the visual acuity of the affected eye will be reduced. Ophthalmoscopy of such eyes, however, does not show any consistent feature that contributes to the diagnosis of orbital hemangioma.
For some reason, the capillary hemangioma of the orbit is associated less often with hemangiomatosis when compared to the hemangiomas of the eyelid and face. The infant with a hemangioma of the eyelid is prone to strawberry hemangiomas on the trunk, extremities, or scalp. We do not know of any orbital hemangiomas associated with visceral hemangiomatosis (Kasabach-Merritt syndrome) unless there is also a large facial hemangioma. In this syndrome, thrombocytopenia and bleeding are the results of entrapment of platelets within the hemangioma of the viscera (Jakobiec and Jones, 1979).
The course of these tumors of the orbit is one of growth that merges into a plateau of inactivity (arrest) followed by regression. However, the rate of growth, the maximum size attained by the tumor, the period of arrest, the degree of regression, and the final age of resolution are unpredictable. Reports analyzing these factors vary greatly. Our own series is of little help in quantifying these factors because it is skewed toward the lesions that continue to grow, the tumors that resist therapy, and those hemangiomas that do not involute.
The presenting pattern of an older child with a capillary hemangioma in the retrobulbar space differs from that described in the preceding text. Here, the course of events is more benign. The growth of tumor is slower; the lesion is more circumscribed; proptosis rather than displacement of the eye is common; and no mass is palpable. As the situation progresses, diplopia develops owing to restricted movement of the eye toward the site of the tumor. Gradually, secondary displacement of the proptotic eye appears, visual blurring occurs secondary to the mass effect of the lesion, and enlargement of the orbit is seen on radiography. In brief, the course is similar to the growth pattern of a cavernous hemangioma in the same location.
An unusual case with a growth pattern of the latter type was reported by Lyness and Williams (1986) in a 23-year-old woman. For many years, a small, translucent, and painless “blister” had been present overlying the patient’s left lateral rectus muscle. Onset of discomfort brought her for consultation. Six millimeters of proptosis was found, and with computed tomography a large soft tissue mass occupied most of the length of the affected muscle. Partial excision of a bluish tumor in the substance of the muscle was performed. The histopathologic diagnosis was intramuscular hemangioma of the small vessel (capillary) type. In retrospect, it is likely that this hemangioma had been slowly expanding over a period of many years.
We saw one patient with biopsy proved intramuscular hemangioma. A 26-year-old woman noted gradual but slow progressive proptosis of the right eye. A few years later, she developed hyperthyroidism and she was treated with antithyroid medication. The medication was subsequently stopped and the thyroid function normalized with no additional therapy required. We examined her at the age of 36 years for thyroid-related ophthalmopathy. The course of her disease had been gradually progressive over the 10 years since onset. There was no pain, diplopia nor any changes with Valsalva maneuver; however, the globe did seem subjectively “irritated”. The vision was normal and 5 mm proptosis was measured. The CT scan showed an abnormality confined to the medial rectus muscle. (see Fig. 10.3). At surgery, the gross appearance of the muscle
was purple-red with visible vessels. Retrobulbar triamcinolone injections reduced the irritation for 9 years at which time another injection was given with satisfactory results.
was purple-red with visible vessels. Retrobulbar triamcinolone injections reduced the irritation for 9 years at which time another injection was given with satisfactory results.
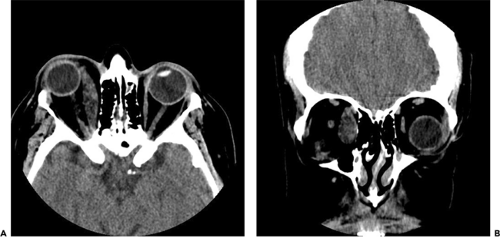 Figure 10.3 Axial (A) and coronal (B) computed tomography scan (unenhanced) in a 36-year-old woman with intramuscular hemangioma of right medial rectus muscle. Axial scan demonstrates that the entire length of the muscle is involved. The muscle is thickened with inhomogeneous consistency. Coronal computed tomography scan shows tear drop shaped enlargement of medial rectus muscle. |
Imaging Aspects
CT scan demonstrates many of the expected features of the capillary hemangioma. Often, the orbit is enlarged and this is evident on the scan. Use of contrast shows vivid enhancement, confirming the lesion’s vascularity and its infiltrative nature. The lesion can have irregular borders if located either in the eyelids or retrobulbar space, but appears somewhat circumscribed when squeezed between the resistant eyeball and orbital wall (see Fig. 10.4). As a rule, the younger the child, the greater is the enhancement (Sklar et al., 1986). Small phleboliths are occasionally seen in these lesions. Magnetic resonance imaging (MRI) of this tumor is illustrated in Figure 10.5. Ultrasonography in the hands of a trained echographer is a useful method for diagnosis in the infant age-group. The ultrasonogram shows a variable pattern mix of high and low reflectivity (see Fig. 10.6) owing to the irregular, intrinsic makeup of the tumor lobules of tumor containing closely packed lumens of differing diameter cordoned by fibrous septa of variable width that contain dilated vessels. Doppler analysis confirms the profuse blood supply of these tumors.
Pathology
The principal event that has occurred in this field since our discussion in the previous edition has been the study of Iwamoto and Jakobiec (1979). They examined, by transmission electron microscopy, three tissue specimens of capillary hemangiomas in children and four tissue specimens of cavernous hemangiomas in adults. Their work established a pathologic basis for classifying capillary hemangioma and cavernous hemangioma as separate
nosologic entities. Previously, many observers either had regarded one tumor as a precursor of the other or both tumors as modulations of each other. Iwamoto and Jakobiec demonstrated definite ultrastructural differences in the two tumors. The principal difference was a mantle of pericytes serving a support function for the endothelial cells of capillary hemangioma, whereas multiple layers of smooth muscle cells provided support for the endothelial lined spaces of cavernous hemangioma. The endothelial cells in both tumors were separated from these support tissues by basement membrane material.
nosologic entities. Previously, many observers either had regarded one tumor as a precursor of the other or both tumors as modulations of each other. Iwamoto and Jakobiec demonstrated definite ultrastructural differences in the two tumors. The principal difference was a mantle of pericytes serving a support function for the endothelial cells of capillary hemangioma, whereas multiple layers of smooth muscle cells provided support for the endothelial lined spaces of cavernous hemangioma. The endothelial cells in both tumors were separated from these support tissues by basement membrane material.
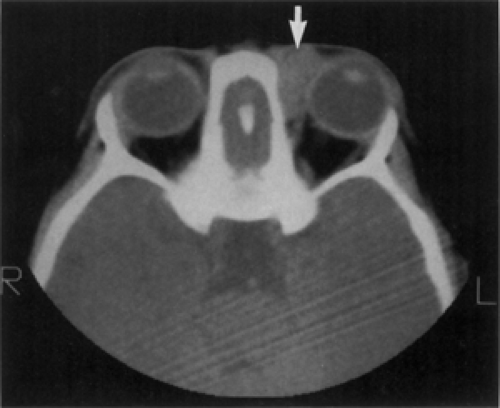 Figure 10.4 Axial computed tomography scan of a capillary hemangioma in an 8-month-old boy shows a homogeneous, enhancing mass in anteromedial left orbit (arrow) overlying medial rectus muscle with lateral displacement of the eye. Mass tends to conform to the surfaces of adjacent bone and eyeball indicating a compressible morphology. No bone erosion. Fullness of superonasal eyelid had been present for four months. |
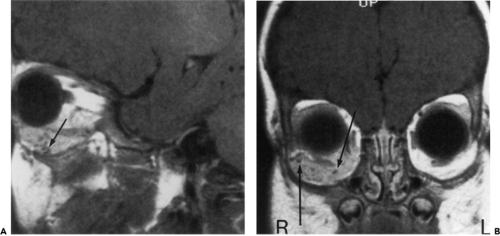 Figure 10.5 Magnetic resonance images at TR = 600 ms and TE = 17 ms of surgically verified capillary hemangioma in the right inferior orbit of a 5-month-old boy. A: Sagittal view: The lesion engulfs the inferior rectus muscle and has poorly defined margins. The tortuous, hypointense area (arrow) represents a tiny blood vessel. B: Coronal view: Shows minimal but homogeneous enhancement. The mass is hypointense compared to the orbital fat in the other orbit. The right orbit is slightly enlarged. The tiny circular voids (arrows) represent vascular spaces. |
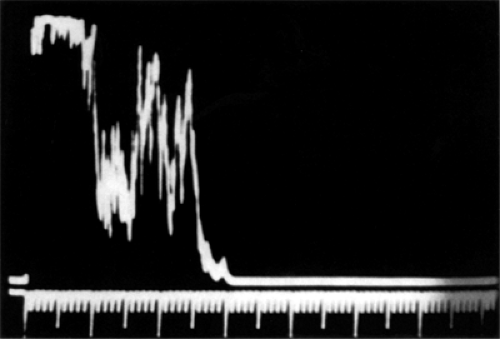 Figure 10.6 Paraocular A-mode echography of capillary hemangioma showing a variable pattern of reflectivity. Compare to Figure. 10.10. (From Sklar EL, Quencer RM, Bryne SF, et al. Correlative study of the computed tomographic, ultrasonographic, and pathologic characteristics of cavernous versus capillary hemangiomas of the orbit. J Clin Neuroophthalmol. 1986;6:14–21 . By permission.) |
By light microscopy, the makeup of capillary hemangioma is essentially similar in all cases. In the most immature stage, the proliferating endothelial cells are so profuse that, under low power, the variable-sized lobules of cells look like a solid tumor. The lobules of tumor are separated by distinct but unevenly arranged septal connective tissue. Under higher power, some mitosis is evident, but the cells, although large, are uniform in appearance. The nuclei are irregularly oval and resemble the nuclei of primitive fibroblasts, except for lack of nucleoli. The borders of the tumor are indistinct and infiltrative. The lumens of the primitive capillaries are narrow and do not seem capable of any circulatory function.
This appearance quickly changes as the tumor rapidly enlarges. It loses its solid look, capillary-sized channels appear, intraluminal clumps of erythrocytes are evident, and the individual endothelial cells become smaller but more distinct (see Fig. 10.7). At this stage, the tumor margins are slightly more circumscribed, and the feeding and draining vessels traveling along the connective tissue syncytium are prominent. Reticular stains at this stage clearly outline the basement membrane that compartmentalizes individual capillary units.
Eventually, involution, either spontaneous or therapeutically induced, sets in. The connective tissue septa thicken;
they are less vascularized, and more fibrosed. The endothelial cells tend to flatten, capillary lumens become ectatic and enlarged, intralesional fat deposition is evident, and occasional interstitial macrophages may appear (see Fig. 10.8). This sclerosing stage resembles the appearance, in miniature, of a cavernous hemangioma in an adult and is responsible for the incorrect diagnosis, in past years, of cavernous hemangioma in children.
they are less vascularized, and more fibrosed. The endothelial cells tend to flatten, capillary lumens become ectatic and enlarged, intralesional fat deposition is evident, and occasional interstitial macrophages may appear (see Fig. 10.8). This sclerosing stage resembles the appearance, in miniature, of a cavernous hemangioma in an adult and is responsible for the incorrect diagnosis, in past years, of cavernous hemangioma in children.
 Figure 10.7 Capillary hemangioma: Capillary-size channels are lined with endothelial cells and contain intraluminal erythrocytes (hematoxylin and eosin; × 300). |
Treatment and Prognosis
The current popular remedy is an intralesional injection of a combination of synthetic corticosteroids. The combination is usually a mixture of a long-acting and rapid-acting corticosteroid such as triamcinolone and bethamethasone sodium phosphate. The treatment is easily administered and can be repeated. There is an ever increasing volume of literature on this subject since it was introduced by Kushner (1979). These reports generally recount the location and technique of administration and the clinical response of the treated tumor. The injections are usually confined to eyelid tumors. Therefore, information on the use of this remedy in orbital lesions is sparse.
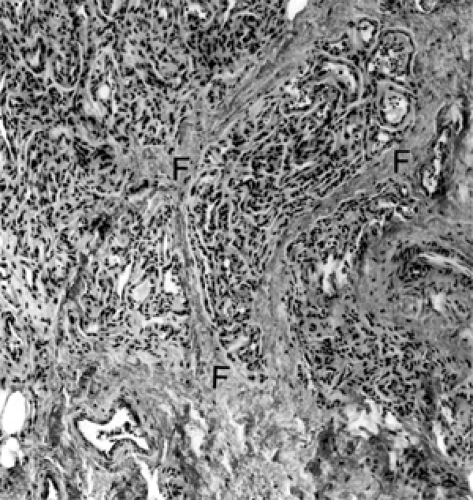 Figure 10.8 Sclerosing capillary hemangioma: Lobules of tumor are separated by fibrous tissue bands (F) (× 100). |
There is a natural reluctance of many clinicians to thrust a needle into a suspected hemangioma posterior to the orbital septum chiefly because of possible uncontrolled bleeding or worrisome hematoma. Other drawbacks are whether the injection can be properly localized to the mass and the ever present risk of ocular embolism from an inadvertent arterial injection (Shorr and Seiff, 1986). Finally, many clinicians disapprove of any intraorbital injection without a preliminary biopsy.
There are several options for handling these situations where the tumor is entirely intraorbital. One consideration applicable to hemangiomas in the anterior orbit is to perform the injection with ultrasonic-assisted guidance such as described for fine-needle orbital biopsy in Chapter 2. Another option is to proceed with an orbitotomy and, with the lesion exposed, proceed with an intralesional injection with or without preliminary biopsy. We have also used this opportunity to apply bipolar cautery to the exposed lesion on occasion. Lastly, other than simple observation, one could consider treatment with systemically administered corticosteroids or subcutaneous interferon α-2b.
For those orbital hemangiomas that extend into the substance of the eyelid, both the superficial and deep components can be injected; alternatively the eyelid component can receive the injection and the orbital extension can be treated with systemic corticosteroids. All of these options have probably been used in the treatment of capillary hemangioma, but there are an insufficient number of orbital cases treated by any one method to report any meaningful data.
Systemic corticosteroid therapy has been used for both orbital and adnexal hemangiomas since 1970 (de Venecia and Lobeck, 1970). Most such cases have been infants, and the drug dosage has been managed by a pediatrician. The initial response to such therapy has been favorable in a large number of cases but marred by the annoying “rebound” growth of tumor in a significant subset of patients after the drug is discontinued. Hastings et al. (1997), while reviewing their experience with interferon α-2b, noted that the literature estimates a favorable response in 60% of patients treated with oral steroids. The response rate to intralesional steroids was approximately 80%. O’Keefe et al. (2003) reported that intralesional injections are a safe and effective treatment although skin atrophy and eyelid necrosis have been reported (Sutula et al., 1987; Townshend and Buckley, 1990). Of course, the
corticosteroids can again be administered over another several weeks or months until such time as the volume of tumor subsides to the desired level. If the tumor continues to regrow after each series of treatment or arrest of tumor cannot be accomplished with low-dose maintenance therapy, the patient, the physician, and the parents soon become corticosteroid-dependent although only one of the triumvirate is receiving the drug. Such a prolonged treatment then becomes no better than if no treatment had been given initially and, instead, the infant is simply observed. In short, the maximum amount of drug to achieve arrest of tumor growth should be determined initially. If the lesion has not responded or continues its rebound behavior when that goal is reached, another therapy should be tried.
corticosteroids can again be administered over another several weeks or months until such time as the volume of tumor subsides to the desired level. If the tumor continues to regrow after each series of treatment or arrest of tumor cannot be accomplished with low-dose maintenance therapy, the patient, the physician, and the parents soon become corticosteroid-dependent although only one of the triumvirate is receiving the drug. Such a prolonged treatment then becomes no better than if no treatment had been given initially and, instead, the infant is simply observed. In short, the maximum amount of drug to achieve arrest of tumor growth should be determined initially. If the lesion has not responded or continues its rebound behavior when that goal is reached, another therapy should be tried.
Another systemic therapy, interferon α-2b, is an option. This drug is given as a daily subcutaneous injection for 3 months, and it is thought to interfere with some of the many growth factors identified in capillary hemangiomas during the proliferative growth phase (Hastings et al., 1997). Loughnan et al. (1992) first reported their successful experience in a 4-month-old girl with a massive orbital capillary hemangioma. The lesion had been resistant to both oral and intravenous corticosteroid treatment. Hastings et al. (1997) later reported results from a group of 40 patients followed up. Sixteen patients had ocular dysfunction from the hemangioma and 15 patients completed the treatment. On average, tumor volume decreased by 82%. The authors noted that the drug was well tolerated with no significant side effects although neutropenia and elevated liver function tests were common.
Other Therapies
Over the 40-year period covered by our collection of tumors, the authors have participated in all the therapeutic modalities, which at one time or another, were considered appropriate. Therapies of earlier years such as sclerosing solutions, cryotherapy, surgical diathermy, and applications of radium plaques no longer need be considered.
Surgery
Thirty-five to 40 years ago, surgical excision was the procedure of choice frequently. It was performed through an anterior orbitotomy. Although hemorrhage during the surgery was always a problem, the surgeon usually managed removal of a sufficient portion of the tumor to hasten its involution (Pasyk et al., 1984). However, postoperatively, there followed such a trail of cicatrix that permanent functional or cosmetic impairment of the eye was the rule. There followed a period in which radiotherapy was the principal therapeutic mode (see subsequent text).
The localization and image visualization of hemangiomas by CT has renewed interest in their surgical removal in the past 15 years. This, combined with present-day surgical techniques, has reduced the complications attributed to surgical intervention. Today, surgical excision is a reasonable treatment option when other therapies have failed. It is the treatment of choice when a rhabdomyosarcoma rather than a hemangioma is suspected. It can also be recommended as the primary treatment for hemangiomas in the retrobulbar space, particularly in older children. An anterior orbitotomy is also an attractive option as a preliminary to intralesional injection of those accessible hemangiomas in the anterior orbit. One could also consider combining a surgical exposure with the use of the carbon dioxide laser for those massive, diffuse hemangiomas that overwhelm the contents of the orbit by their size. Intralesional laser therapy probably represents an evolutionary step in the management of this tumor. Burnstein et al. (2000) treated 100 pediatric patients with capillary/cavernous hemangiomas. An incision was placed into the skin overlying the tumor and the laser fiber was introduced into the tumor. Both the neodymium-doped yttrium-argon-garnet (Nd:YAG) and potassium-titanyl phosphate (KTP) lasers were used with no difference detected between the two types. Two patients with midface lesions had facial nerve weakness and 20 patients had superficial necrosis of the hemangioma with ulceration. Although this treatment may be helpful with extremely large, disfiguring tumors, the orbital region may not be an optimal location for this treatment modality.
Radiotherapy
Radiotherapy, in the form of intracavitary radon seed implantation, was the principal therapy for anteriorly positioned tumors in the period 1951 to 1970. Eleven of the 30 patients in our series were so managed. We used relatively weak seeds, 0.22 to 0.3 mc strength. One to three seeds were placed to encompass the assumed area of the lesion. If multiple seeds were necessary, they were positioned so that the principal radius of γ-radiation of each seed would not overlap the other. The amount of radiation reaching the nearest periphery of the lens was considered the critical measurement. This dosage was in the range of 172 to 744 γ-roentgens. Four of these patients have been followed up for 10, 12, 17, and 21 years. None of the four showed any sign of cataract although we did examine a patient treated elsewhere with radon seeds and who developed extensive basal cell carcinomas of the eyelid.
Two more patients were treated with external beam orthovoltage radiation. One received a total of 480 R to one orbit and the other patient received 1,000 R. The last named has been followed up for 40 years. These patients have neither cataract nor malignancy. These patients did not have the serious cicatricial complications that were seen in the group treated with surgical excision. However, the percentage of patients who developed some degree of amblyopia was about the same in the two groups.
Our experience in this small group tends to refute the dangers frequently attributed in the literature to radiotherapy in infants. We suspect that the misuse of high doses of radiation so common in the decades 1930 to 1960
was responsible for reports of radiation damage and sarcoma. Such complications were not an uncommon event in the long-term follow-up of patients with retinoblastoma who had been so managed.
was responsible for reports of radiation damage and sarcoma. Such complications were not an uncommon event in the long-term follow-up of patients with retinoblastoma who had been so managed.
Embolization
A well-documented resume of this modality is the report of Kennedy (1978) of a 14-month-old girl with a large orbital hemangioma that had resisted numerous therapies since the age of 4 months. Angiography demonstrated three areas of hemangioma in the right orbit with extension into the superior portion of right maxillary sinus. The tumor received its vascular supply from both the internal carotid and external carotid systems. First, transcatheter arterial embolization was performed with tiny silicone pellets through the right internal maxillary and external carotid system. Next, the external carotid artery was ligated. Five days later a clipping of the right ophthalmic artery was performed. At 3½ years of age, an extensive resection of larger tumor residues was performed.
No Therapy
A management scheme of “watchful waiting” or “intelligent neglect” is probably the best of all, except that this ideal is compromised by the wish to halt the shoving and pushing of the tumor on the eye, the need to alleviate obstruction of the visual axis by a closed eyelid, and the urgency of parents to “do something.” The parents can sometimes be mollified by the suggestion of a second opinion from their pediatrician, if neither of the first two factors is in play. It is the need to try to prevent some degree of amblyopia that prompts most clinicians to alleviate the struggling eye. At this point, there is a choice of any or all of the above therapies. Even so, once treatment is deemed necessary, the parents must be warned that a few of these tumors—owing to their contrary, perverse, obstinate, and stubborn character—will always defy and resist involution no matter what treatment is attempted.
Cavernous Hemangioma
A multitude of case reports, reviews, and surveys have been published concerning the vascular neoplasms of the orbit, particularly cavernous hemangioma. The latter is a common tumor. It is well known and is particularly suited for surgical removal. Probably, more has been written about this lesion than any other individual tumor mentioned in this text. It would be unusual to find an ophthalmologist who has not participated in the workup, supervised the care, or considered the differential diagnosis of a patient with an orbital cavernous hemangioma. Those clinicians particularly interested in the subject might well ask, “What can be said about this tumor that already has not been said?” The answer is, “very little!” Therefore, we will treat the salient features in a more summary fashion and devote much of the discourse to those features of the tumor that may vary from its well-known clinical pattern.
Incidence
It is the most common benign neoplasm of the orbit in adults, a feature also noted in our prior texts. Its incidence in our present series (Table 3.3) is 4.3% (82 out of 1795) of the total. In the 1978 series its incidence was 4.7% (36 out of 764) of the total. This underlines its constant prevalence among orbital tumors over a period of time. Its incidence among primary orbital tumors is 14.1% (82 out of 574).
The sex incidence is slightly in favor of women, being 37 men and 44 women (Table 3.3). It occurs most frequently in the fifth decade (33 patients) (Table 3.4), with approximately 50% less in the fourth and sixth decades (18 and 13 patients, respectively). These three decades account for 81% (66 out of 81) of the total. The youngest in our series was a 24-year-old woman whereas the oldest was a 75-year-old woman. The tumor was unilateral in all cases, and there was no significant predilection for either orbit.
All patients have some degree of malposition of the eye, either proptosis or displacement. Proptosis is present in 92% and displacement is present in 25% of the 81 cases. The degree of proptosis averaged 5.2 mm and is approximately equal (5.3 mm in women, 5.1 mm in men) in the two sexes. The latter figures tend to refute a prior impression that men tend to have more proptosis than women because of a longer interval before presentation. However, the two patients who have a proptosis >10 mm are men.
A palpable mass was present in 34% of patients, with the majority in the inferior temporal quadrant. In the remaining 66%, the mass was in the retrobulbar space. We are rather dubious of the value of data pertaining to duration of symptoms prior to presentation. The patient’s memory is sometimes indefinite, and, on many occasions, a patient’s estimate does not jibe with the opinion of a spouse or relative. In 25% of our patients, the tumor, surprisingly, had been present for less than a year. In the remainder, with symptomatology of 1 year or longer, the duration of symptoms averaged 3.5 years.
The second most common symptom was some disturbance of vision and was present in 55% of our patients. It was usually manifest as a decrease in myopia or an increase in hyperopia. A few exceptions to this tumor-induced refractive error will be noted in the subsequent text. An ocular motility disturbance was noted in 35% of total patients.
The most common finding on ophthalmoscopy was choroidal folds (40%) followed in decreasing frequency by optic disk edema (22%), and either pallor or atrophy of the optic disk (8%). Although there was some correlation between choroidal folds and the induced hyperopia, the relationship was not absolute.
Increasingly, we have been seeing patients referred with an incidental orbital tumor. By definition, there is a lack of symptoms and the mass is found when performing cranial imaging for a myriad of reasons, none related to the eye/orbit. We have one patient in this category; however,
the examination revealed evidence of a swollen disk, despite a 20/20 vision. In this instance, we recommended surgery although as Orcutt et al. (1991) reported, we are currently following many patients with asymptomatic lesions.
the examination revealed evidence of a swollen disk, despite a 20/20 vision. In this instance, we recommended surgery although as Orcutt et al. (1991) reported, we are currently following many patients with asymptomatic lesions.
The only other collection of cases similar to our own is the in-depth study of Harris and Jakobiec (1978). They reviewed 66 surgically verified tumors spanning an interval of 39 years, 1937 to 1976. The incidence data of the two series is strikingly similar except for the following: The sex prevalence of the Harris and Jakobiec series favored women to men in a ratio of 7:3, whereas our ratio was 1:2:1. We do not have an explanation for this difference. In the Harris and Jakobiec study, 73% of patients had proptosis, whereas in our series the incidence was 92%. In the modalities of age range, the average proptosis, the duration of symptoms prior to presentation, and the frequency of visual disturbances, the data of the two studies was surprisingly close. This underscores the predictability of behavior of these neoplasms.
Clinical Features
The orbital cavernous hemangioma represents the classical and predictable presentation of a benign orbital neoplasm. The salient feature is a painless, unilateral, nonpulsatile, reasonably slow, progressive proptosis affecting either orbit of a patient in the middle age range. The eyelid will look normal except for slight puffiness, and the functional and anatomic relationship between the eye and eyelids is maintained. Sooner or later, if the tumor is located in the anterior orbit between the eye and nearby bony wall, displacement of the eye develops in approximately 40% of patients. The displacement is opposite to the position of the tumor if the lesion is located in the anterior orbit, but with the retrobulbar hemangioma, the eye will eventually be displaced forward (see Fig. 10.9).
The second most common feature in approximately 50% of patients was some decrease in vision owing to an increasing hyperopia or decreasing myopia induced by the growing tumor pressing on the back of the eye effectively shortening its axial length. This alteration of refraction was closely, but not absolutely, correlated with the appearance of choroidal folds. As a general rule, Friberg and Grove (1983) found that choroidal folds were more likely with greater amounts of exophthalmos or anteriorly located tumors and that the pattern of the folds generally reflected the location of the tumor within the orbit. The shift toward hyperopia was noted with intraconal tumors although extraconal tumors tended to have higher astigmatism. Edema, pallor, or atrophy of the optic disk in a lesser number of patients was usually a tip-off to a close approximation of the tumor to the optic nerve. These patients also have an afferent pupillary defect, some color vision insufficiency, and a visual field defect.
A palpable mass and some degree of ocular motility weakness usually correlate with the onset of displacement of the eye. The motility deficit was usually manifest when gaze was directed toward the position of the tumor. Retrobulbar lesions were seldom palpable.
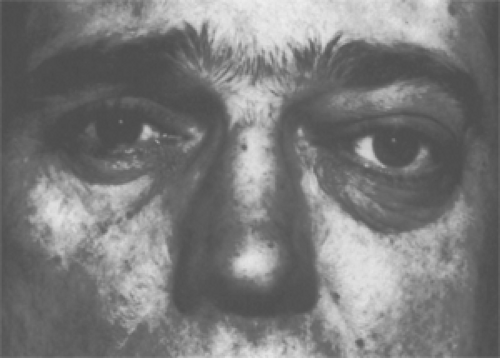 Figure 10.9 A 43-year-old man with several presenting features of a retrobulbar cavernous hemangioma of the orbit of 1-year duration. The left eye was proptosed 8 mm with downward and slight lateral displacement due to tumor in orbital apex medial to optic nerve. Choroidal folds were present, but there was no visual disturbance. (From Henderson JW, Farrow GM, Garrity JA. Clinical course of an incompletely removed cavernous hemangioma of the orbit. Ophthalmology. 1990;97:625–628 , with by permission.) |
Some exceptions and interesting variables in the above pattern should also be mentioned. The eye is not always white. An epibulbar red spot, slight dilation of the epibulbar vessels, or a bluish tinge overlying the tendinous insertion of an extraocular muscle is occasionally seen. Three of our patients had recurring subconjunctival hemorrhage at irregular intervals. In one patient, this cosmetic embarrassment prompted the decision to proceed with surgical removal of the tumor.
Amaurosis fugax was observed in three patients in some positions of extreme gaze. This gaze-evoked amaurosis was transient with recovery of vision when the eye was redirected to primary gaze. The phenomenon is probably an ischemia of the optic nerve as it impinges on the retrobulbar mass in the course of the eye’s excursion (Orcutt et al., 1987). We suspect it is related more to the proximity of the nerve to the surface of the tumor rather than to the tumor size. Rootman and Graeb (1988) also observed transient visual obscurations in 2 of their 12 patients with cavernous hemangioma.
Exacerbation of symptoms with pregnancy has been reported by Zauberman and Feinsol (1970), Harris and Jakobiec (1978), and others and was present in three of our series.
A disturbing feature was the mention of headache by ten of our patients. It was not well localized (“rather deep”) and not well defined in character or severity. However, it seemed sufficiently persistent to warrant its inclusion in the anamnesis. Perhaps it was related to the degree of resistance encountered by the tumor in its area of growth.
This seemed to be the factor in two women reported by Costa e Silva and Symon (1984). In both, severe headache was localized to the temporal area of their affected orbit owing to a cavernous hemangioma expanding within the optic canal. Neither of these patients had proptosis, because the tumor did not extend into the orbital cavity. From the 21 patients included from the 1988 to 1997 interval, there were three patients with prominent but vague peri-orbital headaches. Two of the three had a past history of migraines; two of the three had swollen discs; and two of the three had no proptosis. The headaches either resolved or markedly improved following surgery.
This seemed to be the factor in two women reported by Costa e Silva and Symon (1984). In both, severe headache was localized to the temporal area of their affected orbit owing to a cavernous hemangioma expanding within the optic canal. Neither of these patients had proptosis, because the tumor did not extend into the orbital cavity. From the 21 patients included from the 1988 to 1997 interval, there were three patients with prominent but vague peri-orbital headaches. Two of the three had a past history of migraines; two of the three had swollen discs; and two of the three had no proptosis. The headaches either resolved or markedly improved following surgery.
Of more grave concern were four patients with 20/200 or less vision in the affected eye at time of presentation, associated with a large central scotoma, some degree of optic disk pallor, and an afferent pupillary defect. The duration of their orbital problem ranged from 4 to 14 years, and they were considered diagnostic puzzles until an orbitotomy revealed a cavernous hemangioma in the retrobulbar space. Had CT scan or MRI been available at the time they were first seen, permanent loss of vision would probably have been forestalled by earlier diagnosis and surgical intervention.
We have not encountered multiple cavernous hemangiomas as described by Harris and Jakobiec (1978) in one of their patients. Other reports of multiple tumors must be considered with considerable reserve. These might be examples of a cystic lymphangioma or venous angioma, the latter clustered around the periphery of an orbital vascular malformation.
The clinical features of the cavernous hemangioma of orbital bone will be noted in Chapter 6.
Imaging Aspects
In the years when plain film radiography was the principal imaging resource, slight enlargement of the orbit was noted in many cases. However, such enlargement was also seen in other benign orbital tumors of long duration and, therefore, did not contribute significantly to differential diagnosis. The enlargement of the orbit associated with cavernous hemangioma was never of striking degree when compared to that seen in capillary hemangioma. At present, orbital enlargement, as seen with newer imaging techniques, does not seem to have any prognostic relevance.
Reference has been made to the publication of Sklar et al. (1982) in Figure 10.6 of the prior subchapter, wherein the echographic features of capillary and cavernous hemangioma were contrasted. The pattern of cavernous hemangioma (see Fig. 10.10) is that of a well-marginated mass with uniformly high reflectivity on A-mode scan corresponding to the intralesional septa that separate the cavernous spaces filled with stagnant blood. Doppler analysis combined with A-mode sequences is more subdued when compared to capillary hemangioma because of the reduced blood supply of a cavernous hemangioma.
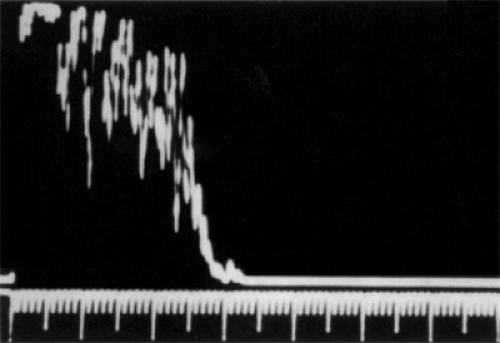 Figure 10.10 Paraocular A-mode echography of cavernous hemangioma showing uniformly high reflectivity corresponding to the intralesional septa that separate the cavernous spaces. Compare to Fig. 10.6. (From Sklar EL, Quencer RM, Bryne SF, et al. Correlative study of the computed tomographic, ultrasonographic, and pathologic characteristics of cavernous versus capillary hemangiomas of the orbit. J Clin Neuroophthalmol. 1986;6:14–21 , with permission.) |
On the CT scan this lesion is a well-demarcated, smoothly marginated, homogeneous mass of increased density (see Fig. 10.11). It may be round, ovoid, oblong, or even acorn-shaped, the latter configuration conforming to the contour of the posterior bony orbit. The tumor is usually slightly less dense than the extraocular muscles. The unenhanced image may show less dense intralesional areas, suggesting lobulation or compartmentalization. Contrast medium does not enter these tumors as easily as capillary hemangiomas and may be quite variable in degree (Savoiardo et al., 1983). There is a tendency to overstate the enhancement factor in the CT scan diagnosis of cavernous hemangioma. Hemangiopericytoma and neurilemmoma may also show many of the above features on CT scan. Therefore, a CT scan diagnosis is only presumptive. CT scan showed a phlebolith in the tumor of one of our patients.
Fries and Char (1988) reported a bilateral cavernous hemangioma based on the CT scan and MRI of bilateral orbital masses in a 48-year-old man. A larger bilobed tumor was removed from the right orbit, and the diagnosis of cavernous hemangioma was histopathologically confirmed. However, the nature of the solitary tumor in the other orbit was not surgically confirmed. This mass could also be a neurilemmoma, a solitary neurofibroma, or a hemangiopericytoma on the basis of similar imaging characteristics of these neoplasms when compared to cavernous hemangioma.
Char and Norman (1985) observed that in almost all cases of large retrobulbar cavernous hemangiomas, CT scan will show sparing of a triangular space at the orbital apex. On the contrary, we have observed filling of the orbital apex by tumor in several instances. One such case is illustrated in Figure 10.12.
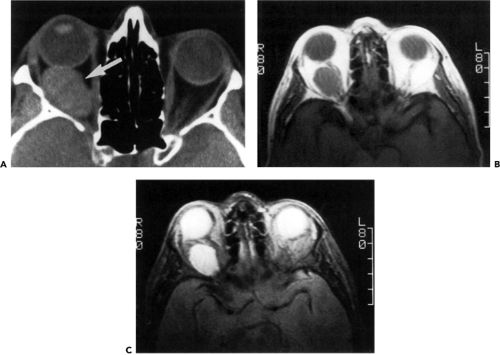 Figure 10.11 A: Axial computed tomography scan of a 51-year-old woman with an oval, well-circumscribed mass (arrow) in the retrobulbar space of right orbit causing proptosis. The mass is approximately 3 cm in greatest dimension and there appears to be a slight expansion of the orbital apex suggesting a tumor of long duration. Proptosis of 4 mm that was first noted 2 weeks previously. This underscores the difficulty of judging the inception of tumor growth on the basis of the patient’s history. The relationship of the mass to the optic nerve was not clear. Therefore a magnetic resonance scan also was suggested to aid in the differential of optic nerve sheath meningioma, cavernous hemangioma, and neurilemmoma. B: Magnetic resonance, T1-weighted sequence of the same tumor. The lesion is hypointense to the surrounding orbital fat, isointense with the nearby medial rectus muscle, and hyperintense to the vitreous. The optic nerve is separate from and displaced medially by the mass. This rules out optic nerve sheath meningioma. C: T2-weighted sequence showing hyperintense mass and adjacent optic nerve in more detail. Surgically verified cavernous hemangioma. |
The configuration, homogeneity, and circumscription of cavernous hemangioma are also well delineated on MRI (Char et al., 1985). The imaging response of the lesion on short and long signal sequences is illustrated in Figure 10.11. This figure also emphasizes the value of MRI in outlining the course of the optic nerve where it is obscured by the hyperdensity of the tumor on CT scan. Regardless of the imaging method employed, the scans also tell the clinician whether the lesion is intraconal or extraconal. Imaging was available for all the 21 patients just been added to our series. Only two patients had extraconal tumors (one above the superior rectus and the other in the inferior temporal quadrant).
Pathology
This neoplasm is the classical, encapsulated tumor of the orbit. The capsule, which is made up of fibrous tissue, is thick enough to provide a firm contour for the tumor, yet sufficiently compressible to permit firm but gentle dissection without rupture. The tumors vary in color from red to reddish blue to purple. They are almost always larger than the eye in their longest diameter (see Fig. 10.13). They may be round, oval, oblong, or even pyramidal in shape, and some portion of a larger retrobulbar tumor will often have a cone-like contour because its surfaces have been molded by contact with the posterior bony orbit.
The lesions usually have a smooth surface but occasionally will be bosselated. These bosselations may represent areas where the tumor is expanding into the host environs.
The lesions usually have a smooth surface but occasionally will be bosselated. These bosselations may represent areas where the tumor is expanding into the host environs.
 Figure 10.12 Axial computed tomography scan of a large retrobulbar cavernous hemangioma (arrow) that completely fills the apex of the left orbit. |
When bisected, the tumor has a sponge-like consistency (see Fig. 10.14), which reflects the numerous ectatic spaces that comprise the main components of the tumor. The large spaces are lined with flattened but not particularly attenuated endothelial cells. The lumens usually contain clumps of erythrocytes showing varying degrees of stasis, intraluminal thrombosis, fibroblastic replacement, and vascularized endothelial buds from the surrounding wall (see Fig. 10.15). A mantle of spindle-like cells of varying thickness encompasses the cavernous-like spaces. These smooth muscle-type cells may merge imperceptibly into the surrounding interstitium or collect into small bundles.
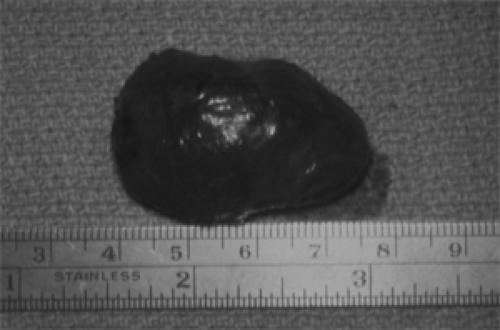 Figure 10.13 Dusky red, smooth-surfaced cavernous hemangioma measuring 35 × 25 × 20 mm that had caused reduced vision for 13 years and proptosis for 6 years in a 40-year-old woman. The pyramidal contour of the portion of the tumor (to the right) suggests molding by the bony contour of the posterior orbit. (See Color image.) |
 Figure 10.14 Cavernous hemangioma: Dilated, blood-filled channels impart a sponge-like appearance to the tumor. Compare to Figure 10.17.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|