Uveal Melanoma: Approaches to Management
Ernest Rand Simpson MD, FRCSC
Background
Choroidal melanoma is the most common primary human intraocular malignancy. The estimated incidence throughout North America is 6 to 7 cases per million per year. Mortality from melanoma typically results from metastatic spread to the liver. Metastases are often delayed in presentation by many years. Historically, the primary therapy for choroidal melanoma was enucleation. The failure of enucleation to prevent metastatic disease has led to the exploration of adjunct therapies. In addition, therapeutic alternatives to enucleation emerged because of a desire to develop globe- and potentially vision-sparing procedures. Evaluation of therapy for choroidal melanoma has proven difficult due to the relative rarity of the malignancy and the long time horizon for metastatic spread.
Collaborative Ocular Melanoma Study
Nearly 20 years ago, the Collaborative Ocular Melanoma Study (COMS) was launched to address the survival benefit of competing treatment options that, at the time, included enucleation and radiotherapy. The study addressed three clinical questions:
Does subtherapeutic external beam radiation prior to enucleation of large choroidal melanomas reduce metastases and mortality?
Is there a survival benefit to enucleation compared to radioactive I125 plaque application in patients with medium-sized choroidal melanoma?
What is the natural history of small choroidal melanomas?
For reasons of consistency in clinical comparison, size characteristics of choroidal melanoma were defined as small (1.0 to 3.0 mm in apical height and at least 5.0 mm in basal diameter), medium (2.5 to 10 mm in height and 16 mm or less in largest basal diameter), and large (greater than 10 mm in height or greater than 16 mm in largest basal diameter and at least 2 mm or greater in height).
Methodology for Collaborative Ocular Melanoma Study Trials
A process of certification to establish clinical center uniformity required repeated certification of each investigator, clinical coordinator, plaquing surgeon, enucleating surgeon, examining ophthalmologist, radiation oncologist, radiation physicist, echographer, photographer, ophthalmic pathologist, and visual acuity examiner.
Patient eligibility and enrollment were determined by a rigid protocol that included
A complete ophthalmic and systemic evaluation.
Color photographs and fluorescein angiography to document tumor size and characteristics.
Standardized echography, including A and B scan evaluation.
Eligibility was confirmed and randomization provided by the Central Study Coordinating Center after full ophthalmologic, radiation, and medical oncology review.
Collaborative Ocular Melanoma Study Protocol Compliance
Overall protocol compliance in the COMS requiring radiation therapy for large tumors was >98% and nearly 95% for medium tumors. Data were collected on standardized forms and submitted within a specific time frame to the COMS central coordinating center and to specific resource centers.
Collaborative Ocular Melanoma Study Small Choroidal Melanoma Observational Study
This component of the study was an observation series of otherwise healthy adults with small choroidal melanomas. The primary endpoints were 5-year mortality and tumor growth. The overall 5-year mortality was low. Five-year all-cause mortality was 6.0% (95% confidence interval [CI], 2.7% to 9.3%) and 8-year all-cause mortality was 14.9% (95% CI, 9.6% to 20.2%.1
Of the small choroidal melanomas initially observed, 21% demonstrated growth by 2 years and 31% by 5 years.2 Factors associated with time to growth were greater initial tumor thickness and diameter, presence of orange pigment, absence of drusen, and absence of retinal pigment epithelial alteration adjacent to the tumor. These observations have also been noted in other large case series of small choroidal melanomas and atypical choroidal nevi. In a separate study, Shields et al. found increased tumor thickness (greater than 1 mm), proximity to the optic nerve, visual symptoms, presence of orange pigment, and presence of subretinal fluid to be predictive of future growth (Fig. 15.1).3
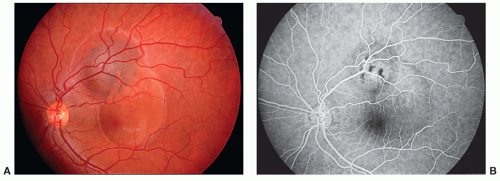 FIGURE 15.1 Small melanocytic choroidal mass with associated serous subretinal fluid. (A) Clinical appearance showing surface lipofuscin and macular involvement with serous fluid. (B) Fluorescein angiogram demonstrating abnormal hyperfluorescence at the level of the choroid with blocked fluorescence due to lipofuscin over the mass. Note reduced fluorescence underlying the serous detachment extending into the foveal region. |
Collaborative Ocular Melanoma Study Medium Choroidal Melanoma Trial
The medium tumor trial compared enucleation to radioactive I125 plaque application. Patients included in the study met the following criteria (Fig. 15.2):
Apical height between 2.5 and 10 mm and basal diameter of 16 mm or less
Visual acuity of at least 20/200 in fellow eye
No neovascular glaucoma
No iris involvement with tumor
No angle involvement with tumor
Clear ocular media
Tumor must not be contiguous with optic disk
Tumor within 2 mm of optic disk must fit within a 90 degree angle with the apex at the center of the optic disk
The tumor must be “plaqueable” in the opinion of the ophthalmologist
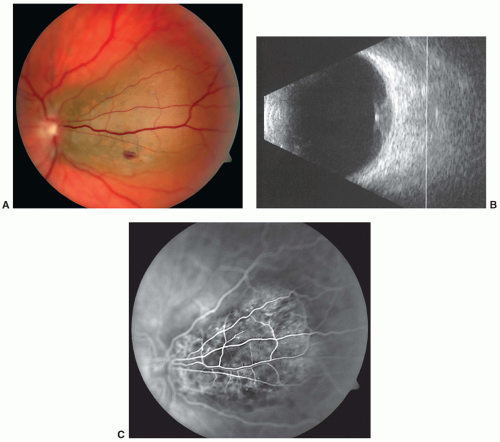 FIGURE 15.2 Juxtapapillary choroidal melanoma excluded from enrollment in the COMS due to proximity to the optic nerve. (A) Clinical appearance showing the tumor involving 180 degrees of the nerve. (B) Ultrasonogram in B mode demonstrating low reflective dome-shaped mass with overlying serous fluid. (C) Fluorescein angiogram of juxtapapillary mass showing mottled hyperfluorescence at the level of the choroid. |
Patients evaluated in the COMS were excluded for the following indications (Fig. 15.3):
Use of immunosuppressive therapy
Previous treatment for choroidal melanoma
Previous intervention in the eye that was tumor related
Previous fine needle biopsy of suspected tumor
Extrascleral extension of >2 mm
Diffuse, “ring,” or multiple melanoma
Other known primary tumors except cervical carcinoma in situ or nonmelanotic skin cancers
Any disease compromising survival
Involvement of 50% or more of the ciliary body with tumor
Tumor contiguous with optic nerve
Contraindications to surgery or radiation therapy
Contraindication to anesthesia if enucleation required
A total of 22% of patients evaluated for the study were deemed to be ineligible for enrollment. The most common reasons for exclusion were proximity of the tumor to the optic disk (40%), one or more primary cancers (20%), and melanoma that was primarily in the ciliary body (11%).
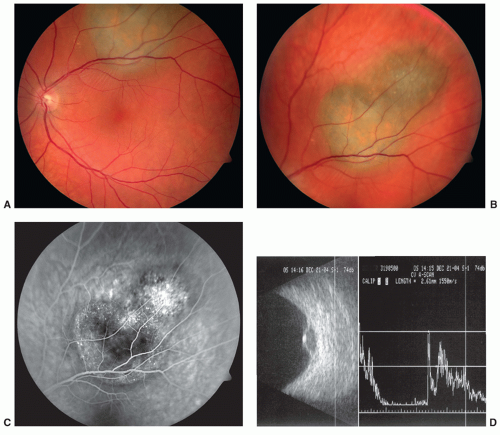 FIGURE 15.3 Medium choroidal melanoma with orange pigment, beginning to affect macular function. (A) Clinical appearance of choroidal mass with overlying lipofuscin beginning to exert traction on paramacular retina. (B) Margins of tumor are ill-defined with an irregular contour. (C) Fluorescein angiogram showing more specific contour of the mass, abnormal hyperfluorescence with partial blocking effect from orange pigment, and dot-like fluorescence indicating Bruch’s membrane alteration. (D) Ultrasonogram in B mode showing dome-shaped low reflective mass with an A-mode height measurement of 2.61 mm. |
Brachytherapy
Plaque radiotherapy remains in widespread use throughout the world as the most common method of delivering therapeutic doses of radiation to intraocular tumors, including choroidal melanoma. High-energy sources such as cobalt have been replaced by lower energy radioisotopes including iridium-192, ruthenium-106, palladium-103, and iodine-125. There are a number of reasons why iodine-125 was the radioisotope chosen for the COMS. Eleven millimeters of lead is needed to block 50% of emitted photons from a plaque employing cobalt, whereas only 1 mm of gold can arrest all radioactive emission from an iodine-125 containing plaque. Although some investigators utilize different radioisotopes for various tumor shapes and volumes, the most commonly employed radioactive isotope is iodine-125. With a half-life of 60 days, this isotope is relatively safe for both the patient and the operating surgeon and can be incorporated into the plaque structure on site with a high degree of accuracy and reproducibility. Iodine-125 can provide sufficient dose rates to tumors without exposing the sclera to excessive radiation.
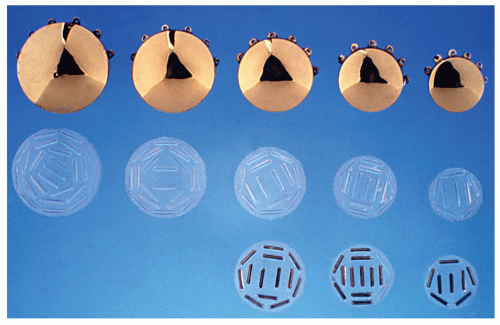 FIGURE 15.4 Structure of iodine-125 radioactive plaques employed in brachytherapy for choroidal melanoma. Seeds, silastic inserts, and gold backing disassembled. Plaque sizes range from 12 to 20 mm in diameter. |
Plaque dosimetry for individual tumors is provided by the ocular oncologist and radiation oncologist in conjunction with the radio-physicist, and according to precise clinical measurements obtained through ophthalmoscopy, ocular imaging, and echography, plaques are constructed to cover the tumor base with a 2.0 mm margin greater than the largest tumor base dimension (Fig. 15.4). At the time of surgery, plaque placement is facilitated by either transillumination of the tumor margins or standard indirect ophthalmoscopic localization techniques with or without ultrasound assistance. The plaque is then secured to the sclera and the final position verified by either intraoperative echography or an indirect ophthalmoscopic-fiberoptic system (Fig. 15.5).
Brachytherapy is usually applied to medium category tumors with the aim of treating the tumor apex with ˜8,500 cGy, with dose delivery over 3 to 7 days (Fig. 15.6). Brachytherapy in the COMS employed iodine-125 plaques.
Complications of plaque therapy include treatment failure due to tumor recurrence, radiation vasculopathy, cataract formation, vitreous hemorrhage, optic neuropathy, and diplopia resulting from ocular muscle manipulation during plaque placement and removal.
Collaborative Ocular Melanoma Study Medium Tumor Results
Of the 1,317 patients enrolled in the study of medium-sized choroidal melanomas, 660 were assigned to enucleation and 657 to iodine-125 brachytherapy. The primary outcome was mortality at 5 and 10 years (Table 15.1). Eighty-one percent of patients had been followed for 5 years and 32% for 10 years at the end of the 11.5-year accrual period. The unadjusted estimated 5-year survival rates were 81% and 82%, respectively, with no clinical or statistical difference in survival rates overall (Table 15.2). Five-year rates of death with histopathologically proven melanoma metastasis were 11% and 9% following enucleation and brachytherapy, respectively (Table 15.3).4 The power of the study was sufficient to indicate that neither treatment was likely to increase or decrease mortality rates by as much as 25% relative to the other.
While there was no significant survival advantage conferred by removal of the eye, the visual results of patients receiving treatment with radioactive I125 plaque did show significant visual impairment due to radiation-related complications, particularly radiation retinopathy. At 3 years, 50% of patients had a loss of 6 or more lines of visual acuity and 43% had a visual acuity less than 20/200.5 The risk factors for visual loss at 3 years included
Apical tumor height >5.0 mm
Distance to foveal avascular zone < 2.0 mm
History of diabetes
Presence of tumor-associated retinal attachment
Tumor not dome shaped
By 5 years following brachytherapy for choroidal melanoma, treatment failure resulting in enucleation occurred in 12.5% of patients. Treatment failure was the most common reason for enucleation within 3 years, and beyond 3 years, ocular pain was most common. The
risk factors for treatment failure included older age at enrollment, larger tumors, and increasing proximity of the tumor to the fovea. Treatment failure was associated weakly with poorer survival. Almost all surviving patients retained good visual acuity in the fellow eyes throughout 5 years following treatment for choroidal melanoma.6
risk factors for treatment failure included older age at enrollment, larger tumors, and increasing proximity of the tumor to the fovea. Treatment failure was associated weakly with poorer survival. Almost all surviving patients retained good visual acuity in the fellow eyes throughout 5 years following treatment for choroidal melanoma.6
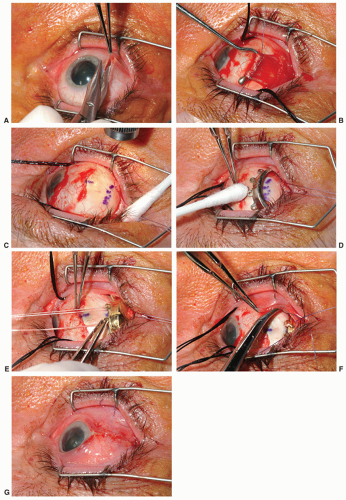 FIGURE 15.5 Surgical placement of an I-125 radioactive plaque in the treatment of a choroidal melanoma in the right eye. (A) The conjunctiva is peritomized laterally to permit access to the tumor situated posteriorly lying in the 9:00 meridian. (B) The lateral rectus muscle is placed on colored Vicryl suture and removed from its insertion. (C) The anterior border of the tumor is identified by transillumination, indirect ophthalmoscopy, or intraoperative ultrasound and marked on the scleral surface. (D) A plaque without radioactivity identical to the proposed I-125-containing plaque is placed to cover the marked sclera and suture points are noted. (E) The “dummy” plaque is removed and replaced with the radioactive plaque which is secured with Mersilene suture. (F) The lateral rectus muscle is temporarily tied into the inferior fornix to be later resutured to the original insertion at the time of plaque removal and (G) the conjunctiva is closed. |
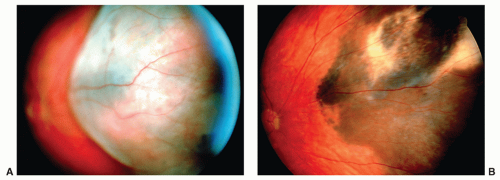 FIGURE 15.6 Medium choroidal melanoma treated by iodine-125 plaque radiotherapy. (A) Before treatment with I-125 plaque radiotherapy. (B) The same tumor 2 years following treatment. Note the treatment has reduced the tumor to a flat pigmented remnant over this time interval. |
TABLE 15.1 All-Cause Mortality Data for Collaborative Ocular Melanoma Study (COMS) Medium Tumors (COMS Report #18) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||
TABLE 15.2 Five-Year Mortality By Treatment And Age For Collaborative Ocular Melanoma Study Medium Tumor Patients | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 15.3 Death with Confirmed Melanoma Metastasis for Collaborative Ocular Melanoma Study Medium Tumor Patients | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
Collaborative Ocular Melanoma Study Large Choroidal Melanoma Trial
Enucleation of eyes containing choroidal melanoma does not necessarily prevent metastatic disease from presenting years later. The observations of Zimmerman et al.7 and McLean et al.8 raised the question of whether globe manipulation during enucleation disseminated viable tumor cells to produce metastases. This premise is often referred to as “The Zimmerman hypothesis.” Adjunctive treatments have been proposed for large choroidal melanoma to reduce the possibility of tumor dissemination during enucleation. These have included pre- and post-enucleation irradiation of the globe and orbit as well as cryotherapy, chemotherapy, immunotherapy, and combinations thereof. The COMS was the first prospective randomized management strategy to assess preoperative radiation preceding enucleation. The primary outcome measure was mortality at 5 and 10 years.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


