Purpose
To evaluate the intraoperative use of handheld Fourier-domain optical coherence tomography (OCT) during Descemet stripping automated endothelial keratoplasty (DSAEK) to assess the donor-host interface.
Design
Prospective, observational case series.
Methods
Six patients undergoing DSAEK surgery were included. OCT scans of the cornea were performed intraoperatively after insertion of the donor disc, after instillation of air in the anterior chamber beneath the disc, after vent incisions in the host cornea in each quadrant, following air-fluid exchange at the end of operation, and on day 1 after surgery. The central 3 mm of each cornea was scanned. The broadest gap between donor and host cornea (interface space) was measured.
Results
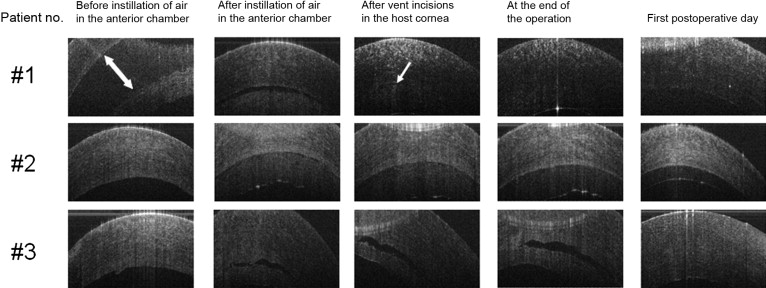
Adequate readings could be obtained from all patients without any complications. In 2 patients there was a decrease in the width of the interface space after each surgical step documented by the OCT scans. At the end of their operation, no interface space was detectable. In 2 patients, interface space disappeared after the vent incisions and did not reappear during the further course of the surgery. In further 2 patients the separation between the host and donor was still detectable at the end of the operation. All patients had no detectable interface gap on day 1.
Conclusions
Handheld anterior segment OCT can be used to assess the host-donor interface in lamellar corneal transplantation surgery. Donor adherence can occur in spite of residual interface space at the end of surgery. Further studies should be conducted to answer the question of which surgical steps are useful in assisting with donor adhesion.
Corneal endothelial transplantation has rapidly gained popularity since posterior lamellar keratoplasty was first reported in animal studies by Ko and Feldman (Ko W, Feldman S. Experimental posterior lamellar transplantation of the rabbit cornea. ARVO, Sarasota, FL, 1993) and then introduced clinically by Melles and Terry. The technique and instrumentation have undergone a number of modifications and became the foundation for Descemet stripping (automated) endothelial keratoplasty (DS(A)EK) described by Price. In this procedure, manual (or automated) lamellar dissection is used to prepare the endothelial graft for transplantation. The advantages of this transplantation technique compared to penetrating keratoplasty, in selected cases, include reduced donor rejection and refractive errors and greater tectonic strength.
Despite modifications to the technique, such as injection of air into the anterior chamber, the usage of a Lindstrom LASIK roller to help remove fluid from the graft interface, midperipheral corneal (vent) incisions to drain remaining interface fluid, and increased duration of a complete anterior chamber air fill, dislocation of the donor disc from the host cornea may occur in up to 82% of cases. Following dislocation, further intervention is needed to reposition the graft and in some cases replace the dislocated graft with a new endothelial graft or even a penetrating keratoplasty. Intraoperative and postoperative changes in the donor-host interface have not been studied. Evaluation of the donor-host interface in DSAEK surgery is needed. This may allow the effect on the interface of future modifications to the technique to be evaluated in order to reduce donor dislocation.
Optical coherence tomography (OCT) is a multidimensional interferometric optical signal acquisition and processing method that allows for high-quality cross-sectional imaging of tissue in micrometer resolution within the eye. This technique has become a valuable diagnostic tool not only for retinal disease, but also for anterior segment evaluation. Recently, high-speed Fourier-domain OCT (FD-OCT) has been developed, offering a much better spatial resolution with improved sensitivity compared to the preceding time-domain OCT. FD-OCT allows high-speed, high-resolution imaging of weakly backscattering biological tissues in vivo and can therefore detect changes within a 10-μm range in corneal tissue.
In this pilot study, we used the handheld FD-OCT to evaluate the intraoperative feasibility and to assess possible intraoperative and postoperative changes at the host-donor interface in DSAEK procedures. Understanding these events may lead to deeper insight into the pathophysiology of donor disc attachment.
Methods
A prospective observational, single-center pilot case series was performed at the Department of Ophthalmology, University Hospital Zurich. Consecutively scheduled adult patients for DSAEK surgery were included. No exclusion criteria were applied.
The main outcome measure was the yield of intraoperative and postoperative anterior segment FD-OCT scans within a circle with a diameter of 3 mm of the central cornea. Secondary outcome measures were the amount of separation between the host cornea and donor disc (interface space), postoperative donor dislocation rate, and the occurrence of any adverse event. Interface assessment was performed at different stages during and after DSAEK surgery. Time to preservation (ie, the time interval between death and harvesting the donor cornea) was noted in hours. The endothelial cell count of the donor cornea was performed by employing a Leitz Diavert modular inverted microscope (Ernst Leitz Wetzlar GMBH, Wetzlar, Germany). A portable pachymetry device (Corneo-Gage Plus multifunction pachymeter, Sonogage, Inc, Cleveland, Ohio, USA) was used to measure intraoperative donor cornea thickness in micrometers.
Surgical Technique
Surgeries were performed under general anesthesia by 2 surgeons (M.M.B., C.K.) according to following protocol. All donor corneas were harvested from enucleated whole globes using the same technique. Donor corneas were mounted on the Moria automated lamellar therapeutic keratectomy anterior chamber system (Moria S.A., Antony, France), the epithelium was removed, pachymetry performed, and the tissue dissected with a Moria Carriazo Barraquer microkeratome. A 350-μm and 300-μm keratome plate was used for corneas thicker than 550 μm and thinner than 550 μm, respectively. Calculated donor thickness (depth of microkeratome plates subtracted from initial pachymetry) was recorded. Donor tissue was then trephined using a 7.5- or 8.0-mm Hanna trephine (Moria SA, Antony, France). After fashioning a temporal 5.5-mm sclerocorneal tunnel, Descemet membrane was scored with a Moria DSAEK Price hook and stripped from the stroma with a Moria DSAEK stripper. A Busin glide spatula (Moria SA) was used to insert the donor disc into the eye. The sclerocorneal tunnel was sutured with 10-0 nylon. Air was injected underneath the donor tissue using a 25-gauge needle. Four vent incisions were placed in the host cornea within the donor margin but well outside the center of the graft. A Lindstrom roller (BD Medical, Franklin Lakes, New Jersey, USA) was used to center the donor tissue. If necessary, further air was injected to achieve a full air fill, which was left for 10 minutes. A 70% air fill was then achieved by partially exchanging air for balanced saline solution. Atropine drops (Atropine 1% SDU Faure; Novartis, Basel, Switzerland) and Tobradex (tobramycin, dexamethasone; Alcon, Huenenberg, Switzerland) ointment were administered. Postoperatively, patients postured face-up overnight with the eye pad left intact.
Optical Coherence Tomography Scans
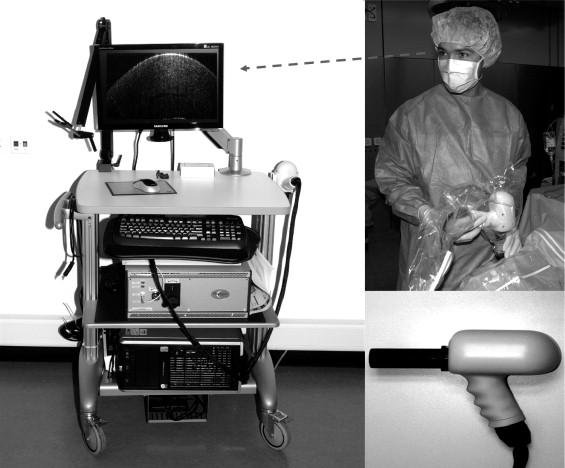
The Bioptigen Spectral Domain Ophthalmic Imaging System (Bioptigen Inc, Durham, North Carolina, USA) with the anterior segment optical bore on a handheld probe was utilized to perform intraoperative and postoperative scans ( Figure 1 ). Preoperatively, the handheld probe including the connection cable was sealed within a sterile bag ( Figure 1 ). The bag was tightened around the optical bore with sterile tape. A hole was cut into the bag at the laser aperture to enable OCT measurements. The scan protocol included centered radial volume scans of 3 mm in diameter, consisting of 100 B-scans and 1000 A-scans per B-scan. In order to yield multiple reproducible scans, the Purkinje central corneal reflex was used to obtain perfect alignment of the central A-scan and the corneal apex.
Intraoperative OCT scans were performed by 2 experienced ophthalmologists (P.B.K., M.N.M.) 1) directly after insertion of the donor disc; 2) after instillation of air in the anterior chamber; 3) after vent incisions in the host cornea in each quadrant; and 4) at the end of surgery. OCT measurements were performed in a sterile environment without any contact to the surgical site in all patients. A fifth set of OCT scans were done on the first postoperative day with the patient in a supine position.
Analysis
All OCT scans were evaluated in nonchronological order by 2 independent observers (P.B.K., M.M.B.). The broadest interface width between donor and host was measured employing a prototype of a caliper tool provided by the manufacturer. The mean of both measurements was recorded. If there was no concordance between the observers (ie, >10% difference between the first and the second measurement), scans were re-evaluated independently by both observers.
Results
Six eyes of 5 female and 1 male subjects undergoing DSAEK surgery for Fuchs endothelial dystrophy (3 patients), endothelial failure in a penetrating graft for keratoconus (1 patient), pseudophakic bullous keratopathy (1 patient), and endothelial failure after multiple previous intraocular surgeries (1 patient) were examined. Mean age was 70 years, ranging from 59 to 83 years. Images of the donor-host interface were obtained from all patients at each imaging session ( Figure 2 ). The interface width was able to be measured as shown in the Table and Figure 3 in all patients. The calculated donor thickness, time to preservation, and endothelial count/mm 2 are shown in the Table .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


