Purpose
To report the outcomes of autologous cultivated limbal epithelial transplantation using the healthy part of the affected eye or the fellow eye as a source of limbal stem cells in patients with unilateral, partial limbal stem cell deficiency (LSCD).
Design
Retrospective, nonrandomized, interventional case series.
Methods
setting : L. V. Prasad Eye Institute, Hyderabad, India. study population : Patients with unilateral, partial LSCD who underwent autologous cultivated limbal epithelial transplantation between 2001 and 2011. intervention : The limbal biopsy was taken either from the healthy part of the limbus of the same eye (ipsilateral group) or from the healthy fellow eye (contralateral group). Cells were cultivated using a xeno-free explant culture technique, and cultivated cells were transplanted onto the affected surface. primary outcome measure : Success of cultivated limbal epithelial transplantation, defined as a completely epithelialized, avascular, and clinically stable corneal surface.
Results
Seventy eyes of 70 patients were studied. The mean follow up was 17.5 ± 7 months. In 34 eyes the limbal biopsy was taken from the ipsilateral eye and in the remaining 36 eyes from the contralateral eye. Clinical success was achieved in 70.59% of eyes in the ipsilateral group and 75% of eyes in the contralateral group ( P = .79). Limbal transplant survival rates at the final follow-up visit were 65.1% ± 0.09% in the ipsilateral group and 53.6% ± 0.12% in the contralateral group ( P = .74).
Conclusions
Ocular surface restoration in partial LSCD is possible with cell-based therapy. Outcomes are similar irrespective of whether the limbal biopsy is taken from the healthy part of the ipsilateral eye or the contralateral eye.
The epithelium of the cornea is the first surface of the eyeball exposed to the external environment, and it constantly undergoes a process of renewal. A healthy, functional corneoscleral limbus is considered to be essential to normal corneal epithelial homoeostasis. The limbus is believed to be a repository of stem cells, which constantly replenish the cells lost during epithelial turnover. Limbal stem cell deficiency (LSCD) clinically manifests with recurrent or persistent epithelial defects, vascularization, pannus formation, conjunctivalization of the corneal surface, and loss of normal corneal clarity.
Cell-based therapy using limbal stem cell transplantation (LSCT) for restoration of the ocular surface in limbal stem cell deficiency has been used with good results at various centers across the world. Our group has reported a success rate of 71% at a mean follow-up of 3 years in a series of 200 eyes with unilateral total LSCD treated with autologous cultivated limbal epithelial transplantation. Similarly, in 50 eyes with unilateral LSCD following a failed primary procedure, we have reported a success rate of 66% at a mean follow-up of 2.3 years using repeat autologous cultivated limbal epithelial transplantation. However, limited literature exists on management of partial LSCD.
The conventional paradigm of cultivated limbal epithelial transplantation in unilateral LSCD rests on harvesting a limbal biopsy from the contralateral eye, cultivating it in a laboratory, and transplanting the resultant epithelial sheet onto the affected eye. In cases with partial LSCD, there are clinically normal–appearing areas of the limbus in the affected eye. We hypothesized that it may be possible to harvest limbal stem cells from the healthy part of the limbus in eyes with partial LSCD and cultivate them ex vivo for transplantation onto the same eye. We have been using the healthy part of the limbus in eyes with partial LSCD as a source of stem cells for cultivated limbal epithelial transplantation for many years. To the best of our knowledge, no study thus far has reported such a procedure, or compared the outcomes with conventional cultivated limbal epithelial transplantation using the contralateral healthy eye as the source of limbal biopsy. This led us to the study question: Does the source of limbal biopsy (ipsilateral or contralateral eye) affect the outcome of autologous cultivated limbal epithelial transplantation for unilateral, partial LSCD? Our hypothesis was that it does not.
The purpose of this study was to compare outcomes of autologous cultivated limbal epithelial transplantation for unilateral, partial LSCD, using the healthy part of the affected eye or the fellow eye as a source of limbal stem cells in patients with partial LSCD.
Methods
Study Design and Subjects
This was a retrospective, nonrandomized, interventional case series. This study was approved by the Ethics Committee of L. V. Prasad Eye Institute, Hyderabad, India, and was conducted in strict adherence to the tenets of the Declaration of Helsinki. Prior written informed consent was obtained from all patients or guardians, as appropriate for the surgical procedure. Charts of all patients who underwent cultivated limbal epithelial transplantation for the treatment of limbal stem cell deficiency between January 1, 2001, and December 31, 2011 were reviewed. Patients who underwent autologous cultivated limbal epithelial transplantation for unilateral (defined as no clinical signs of ocular surface disease in the other eye) and partial LSCD (defined as superficial corneal vascularization, diffuse fluorescein staining of the corneal surface with or without persistent epithelial defects, conjunctivalization of the corneal surface involving the visual axis, and absence of the palisades of Vogt in less than 360 degrees of the limbus) were included in this study.
The following exclusion criteria were applied: (1) patients who had bilateral LSCD or had allogeneic limbal transplantation; (2) patients with dry eye disease (Schirmer test without anesthesia of <10 mm in 5 minutes); (3) patients with no visual potential, as determined by clinical examination and electrophysiological testing; (4) patients with untreated concurrent problems, such as entropion, trichiasis, glaucoma, and infection; (5) patients with age at injury of less than 8 years.
Data Collection
The following parameters were collected: age and sex of the patient; date and etiology of LSCD; details of prior surgery (if any); best-corrected visual acuity (Snellen) at presentation and at each follow-up visit; extent of symblepharon (in clock hours); extent of limbal involvement (in clock hours); duration between injury and cultivated limbal epithelial transplantation; details of surgery performed, including source of limbal biopsy (ipsilateral or contralateral eye); duration of follow-up; and ocular surface status at each visit. Patients were divided into 2 groups, based on whether the limbal biopsy was obtained from the healthy part of the ipsilateral eye or from the contralateral eye.
Outcome Measures
The primary outcome measure in each group was success of cultivated limbal epithelial transplantation, defined as a completely epithelialized, avascular, and clinically stable corneal surface. Failure was defined as recurrence of superficial corneal vascularization, persistent epithelial defects, or conjunctivalization of the cornea. Survival time was calculated from the date of surgery to the date of failure or last follow-up, as per the outcome. Secondary outcome measures were change in best-corrected visual acuity (BCVA) and complications, if any, in each group.
Technique of Limbal Biopsy
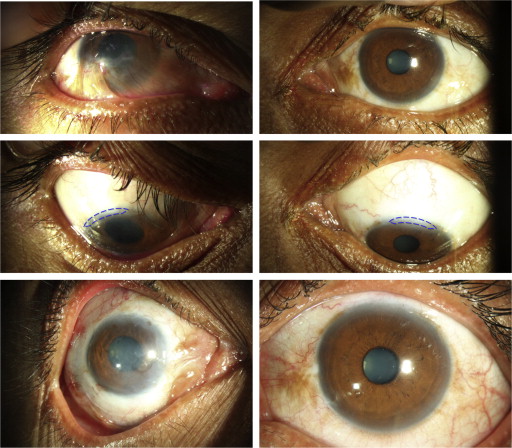
A collage of clinical photographs showing the difference in limbal biopsy techniques in the 2 groups is shown in Figure 1 . The choice of the source of limbal biopsy—either from the healthy part of the limbus of the affected eye or from the healthy contralateral eye—was made at the discretion of the operating surgeon (V.S.S.), who has extensive experience in limbal stem cell transplantation techniques. For the limbal biopsy, a limbus-based conjunctival flap was raised, and dissection in the subconjunctival plane was carried out toward the limbus, extending 1 mm into clear cornea. Conjunctiva posterior to the pigmented palisades was incised, and less than 2 clock hours of pigmented limbus tissue was obtained ( Supplemental Video , available at AJO.com ).
Technique of Limbal Culture
Our technique of limbal culture has been described earlier. Briefly, the biopsied tissue was transported in human corneal epithelium medium to the stem cell laboratory, where it was shredded into small pieces and placed on the basement membrane side of de-epithelialized human amniotic membrane. A feeder cell–free submerged explant culture system was used to obtain a confluent monolayer of epithelial cells, usually at 10-14 days.
Technique of Limbal Transplantation
Symblepharon release was done, if it prevented insertion of an eye speculum. Peritomy was performed and fibrovascular pannus excision was carried out, starting from the peri-limbal sclera and proceeding inward onto the cornea. Apparently healthy areas of limbus were not disturbed. The human amniotic membrane with the monolayer of cultivated epithelial cells was transferred to the ocular surface with the epithelial side facing up, and was secured to the surface using either sutures or fibrin glue (TISSEEL Kit; Baxter AG, Vienna, Austria).
Postoperative Management
Topical medication included 1% prednisolone acetate eye drops, started 8 times per day and tapered to once daily by 4-6 weeks, as well as 0.3% ciprofloxacin hydrochloride eye drops used 4 times a day until resolution of epithelial defect. Patients were followed up on day 1, 7, 42, and 90 postoperatively and thereafter at 3- or 6-month intervals as required. A complete ocular examination was performed at each visit.
Statistical Analysis
We used the R 2.14.1 statistical software for Windows (open source, available from http://www.r-project.org/ ) for all computations. The Shapiro-Wilk test was used to test normality of data. Baseline parameters in both groups were compared using Wilcoxon rank sum test for continuous nonparametric variables and Fisher exact test for categorical variables. Kaplan-Meier survival curves were generated and survival probability was reported in percentages (± standard error) for success of limbal transplantation in each group. A multivariate Cox proportional hazards model analysis was then carried out to look for the association between various clinical factors (age, sex, laterality, etiology of injury, previous surgical procedures, duration between injury and transplantation, presenting visual acuity, lid abnormalities, extent of limbal involvement, extent of symblepharon, source of limbal tissue, type of surgical procedure) and failure of transplantation.
Results
Patient Demographics
The study included 70 eyes of 70 patients. The mean follow-up period was 17.5 ± 7 months. The mean age of the patients was 24 ± 12.5 years. The male-to-female ratio was 4:1. In 36 eyes the limbal biopsy was taken from the contralateral eye and in the remaining 34 eyes from the ipsilateral eye. The baseline characteristics in the 2 groups are shown in Table 1 . Both groups were similar in terms of age, sex, etiology of LSCD, duration of injury prior to surgery, extent of LSCD, severity of vision loss, and preoperative visual acuity. In addition to cultivated limbal epithelial transplantation, 14 and 17 eyes in the ipsilateral and contralateral eye (as a source of limbal biopsy) groups, respectively, underwent symblepharon release simultaneously.
| Ipsilateral Group | Contralateral Group | P Value | |
|---|---|---|---|
| Median age (y) | 27.5 | 25.5 | .254 a |
| Sex | .374 | ||
| Female | 5 | 9 | |
| Male | 29 | 27 | |
| Etiology | .472 | ||
| Alkali injury | 16 | 21 | |
| Acid injury | 10 | 6 | |
| Chemical (unknown) injury | 2 | 1 | |
| Thermal injury | 3 | 5 | |
| Mechanical trauma | 2 | 2 | |
| OCP | 1 | 0 | |
| Idiopathic | 0 | 1 | |
| Duration (in months) | .553 a | ||
| Mean | 34.3 | 27.5 | |
| Median | 6.5 | 7 | |
| Vision loss | .309 | ||
| Mild (BCVA >20/60) | 3 | 8 | |
| Moderate (BCVA 20/60-20/200) | 16 | 16 | |
| Severe (BCVA <20/200) | 15 | 12 | |
| Extent of LSCD (clock hours) | .245 a | ||
| Mean | 6.53 | 7.11 | |
| Median | 6 | 6 | |
| Persistent epithelial defect | >.99 | ||
| Present | 1 | 2 | |
| Absent | 33 | 34 | |
| Symblepharon (clock hours) | .358 a | ||
| Mean | 2.79 | 1.88 | |
| Median | 0 | 0 | |
| Lid abnormalities | >.99 | ||
| Entropion | 6 | 2 | |
| Ankyloblepharon | 2 | 0 | |
| Ptosis | 1 | 0 | |
| Previous surgery | .317 | ||
| None | 19 | 16 | |
| One | 6 | 14 | |
| More than 1 | 9 | 6 | |
| Surgery done | .638 | ||
| LSCT | 20 | 19 | |
| LSCT + symblepharon release | 14 | 17 | |
| Median preoperative visual median BCVA (logMAR) | 1 | 0.89 | .249 a |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


