Ultrasonography has an ever increasing role in the management of a wide variety of diseases affecting the head and neck. While ultrasonography is most commonly used for imaging of thyroid pathology, it also can be utilized in a host of diagnostic and therapeutic procedures. This article reviews the office-based ultrasound-guided procedures in the head and neck and discusses technical considerations for performing these interventions.
Over the past decade, ultrasonography (US) has become an instrumental component in the diagnostic evaluation of a multitude of head and neck pathologies. The technology can also be beneficial for image guidance during percutaneous and open head and neck procedures. Although US-guided fine-needle aspiration biopsy (FNAB) accounts for the vast majority of these procedures, US guidance can also be used for aspiration of fluid collections and therapeutic injections as well as an intraoperative adjuvant to guide revision surgery. A thorough understanding of the capabilities of interventional US allows optimal management of a wide variety of complex clinical scenarios.
Fine-needle aspiration biopsy
Masses of the head and neck are frequently evaluated by FNAB to establish a diagnosis. Although some head and neck masses are easily palpable and hand-guided FNAB is feasible, many masses are indistinct or not palpable and image-guided FNAB is required. Additionally, it is not uncommon for a thyroid nodule or malignant adenopathy of the neck to be a complex mass with both solid and cystic components. In this situation, US guidance can decrease the chance of a nondiagnostic biopsy by ensuring that the solid component of the mass is sampled during the procedure. US-guided FNAB for nodular disease of the thyroid is the most commonly performed US-guided procedure, but salivary gland masses and cervical adenopathy as well as a wide variety of unusual neck masses may require image guidance for cytologic assessment. In addition to understanding the indications for biopsy and mastering the techniques of performing a US-guided biopsy, it is critical that otolaryngologists possess a thorough understanding of the limitations and potential pitfalls of FNAB in the assessment of masses in these areas.
Thyroid
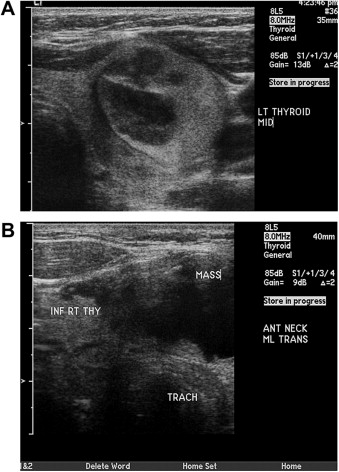
In patients with thyroid nodules, many factors are considered when determining whether or not surgical intervention is required. Because most thyroid nodules are asymptomatic and nonfunctional, the key determinant of the need for surgery is the risk that a nodule represents a neoplasm. Although history, physical examination, and specific US features can assist otolaryngologists in determining the potential for neoplasm, FNAB is considered the most accurate diagnostic evaluation to assess for malignancy ( Fig. 1 ). In patients with larger nodules, palpation-guided FNAB can be easily performed in the outpatient setting without the need for image guidance. But, many thyroid nodules are not easily palpable and image guidance is required to complete the biopsy. Additionally, some palpable thyroid nodules can be complex masses with dominant cystic components. In this scenario, US guidance to ensure sampling of the solid component is valuable to ensure a diagnostic biopsy. Comparisons of palpation-guided and US-guided FNAB for thyroid nodules suggest that US-guided FNAB is more accurate and results in a lower rate of nondiagnostic biopsies. In a review of 376 FNABs of the thyroid, Izquierdo and colleagues reported that for palpable thyroid nodules, US-guided FNAB was 20% more accurate (80%) and had a lower incidence of nondiagnostic specimens (7.1%) when compared with palpation-guided FNAB.
Recently, the National Cancer Institute proposed a 6-tiered classification scheme for the assessment of thyroid FNAB ( Table 1 ). Based on this system, the risk of malignancy for a thyroid nodule is defined and guidelines for management are proposed. In patients with nodules that by FNAB are suggestive of neoplasm, suspicious for malignancy, or malignant, surgery is recommended. It is critical, however, to consider FNAB as only one component of the diagnostic evaluation of a patient with a thyroid nodule. In patients with history, physical examination, or imaging findings suggestive of malignancy, surgery should be recommended even if the FNAB is interpreted as low risk of malignancy.
| Suggested Category | Alternate Category | Risk of Malignancy |
|---|---|---|
| Benign | <1% | |
| Atypia of undetermined significance | Indeterminant follicular lesions rule out neoplasm Atypical follicular lesion Cellular follicular lesion | 5%–10% |
| Neoplasm | Suspicious for neoplasms | 20%–30% |
| Suspicious for malignancy | 50%–75% | |
| Malignant | 100% | |
| Nondiagnostic | Unsatisfactory | — |
In addition to the cytologic assessment of FNAB in a patient with suspected well-differentiated thyroid cancer, assessment for thyroglobulin in the saline washout of the needle after biopsy of a mass can be performed. Especially if a mass is suspected to be recurrent disease and has negative cytology, this technique can be a useful method to confirm the presence of disease. This technique can be used on masses suspected to be local or nodal recurrences, with the greatest benefit in lesions smaller than 1 cm. After a 1-mL saline washout, a thyroglobulin of greater than 4 to 10 ng/mL has been established as indicative of disease, but false-positive results can occur. This technique is valid even in patients who have antithyroglobulin antibodies. Analysis for BRAF can also be completed on material obtained by FNAB in patients suspected of having papillary thyroid cancer. In the future, such an assessment may be important in surgical planning because patients with BRAF mutations are known to have more aggressive disease.
In a fashion similar to thyroglobulin washout in patients with well-differentiated thyroid cancer, calcitonin washout can be performed in patients suspected of having primary or recurrent medullary thyroid cancer. In 36 patients suspected of having medullary thyroid cancer, the sensitivity and specificity of calcitonin washout has been reported as 100%, with FNAB cytologic evaluation having a sensitivity of 62% and specificity of 80%. Although a calcitonin greater than 36 pg/mL is indicative of medullary thyroid cancer, others have found that patients with benign thyroid conditions can have calcitonin washout as high as 67 pg/mL and that in cases of medullary thyroid cancer the calcitonin washout was extremely high.
Parathyroid
Unlike nodular disease of the thyroid, which routinely undergoes cytologic assessment, rarely is it necessary to perform FNAB for parathyroid pathology. For patients with hyperparathyroidism, the need for surgery is based on the metabolic sequelae of the disease rather than the concern that the disease represents malignancy. The success of parathyroidectomy for hyperparathyroidism is high with cure rates greater than 95%, obviating FNAB to confirm suspected lesions as parathyroid in origin.
In the small subset of patients who have persistent or recurrent hyperparathyroidism after prior surgical explorations, FNAB can play a role in the localization of the disease. In cases of persistent/recurrent disease, the pathology is usually located in the previously dissected central compartment. Subsequently, use of FNAB to confirm that suspicious lesions in previously operated fields are of parathyroid origin can be beneficial before revision surgery. When performing FNAB to confirm parathyroid disease, consider obtaining a parathyroid hormone washout of the aspirate in addition to cytologic assessment. Agrawal and colleagues reported limitations with cytologic evaluation of suspected parathyroid lesions by FNAB. In their series of 53 patients undergoing FNAB of suspected parathyroid lesions, the cytologic evaluation was able to identify parathyroid cells in only 40% of aspirates, with 28% of the aspirated being nondiagnostic. Although the features of monomorphic cells with stippled nuclear chromatin in the absence of atypia, mitosis, or prominent nucleoli are suggestive of parathyroid origin, distinguishing parathyroid from thyroid tissue can be problematic especially if there is not any colloid in the specimen. Erbil and colleagues assessed the role of parathyroid hormone washout on the FNAB of lesions of the central compartment. Lesions suspected of parathyroid origin could be consistently discriminated from thyroid pathology with the parathyroid lesions having an average parathyroid hormone level of 4700 pg/mL compared to 48 pg/mL in the thyroid lesions.
Salivary Gland
A wide variety of benign and malignant neoplasms can affect the major and minor salivary glands. Additionally, some non-neoplastic diseases can present as a salivary gland mass. The vast majority of salivary gland neoplasms are located in the parotid gland. The use of FNAB for salivary gland neoplasms is controversial, but it should be considered in the diagnostic evaluation of a patient with a salivary gland mass. Opponents of FNAB of salivary gland neoplasms feel that surgical excision should be performed for all tumors and that cytologic diagnosis does not significantly alter the treatment plan. Proponents of FNAB of salivary gland neoplasms feel that cytologic information assists in determining the risk of malignancy, allowing for optimal surgical planning and patient counseling preoperatively.
Given the wide variety of benign neoplasms as well as low-grade and high-grade malignancies that can affect the salivary glands, limitations exist regarding the ability of FNAB to establish a definitive diagnosis. Although some benign neoplasms, such as pleomorphic adenoma and Warthin tumor, can be accurately diagnosed by FNAB, other pathologies are more difficult to specifically classify on FNAB. For example, differentiating a cellular pleomorphic adenoma from a low-grade basal cell adenocarcinoma cannot be accomplished. Additionally, determining the exact pathologic subtype of a high-grade carcinoma is not possible ( Table 2 ). The ability of US-guided FNAB of salivary gland neoplasms to distinguish benign from malignant tumors is high, with Bajaj and colleagues reporting a sensitivity of 85%, specificity of 96%, and overall accuracy of 94%. Others have proposed core biopsy as the preferred technique for assessment of salivary gland neoplasms. Buckland and colleagues reported 100% accuracy for US-guided core biopsy, with nearly all the masses in the series having undergone a prior FNAB that was nondiagnostic. The slightly more invasive nature of a core biopsy must be considered before implementing routine use of this technique. Overall, there is little doubt that FNAB can play a vital role in the assessment of select patients with a salivary gland mass.
| Erroneous FNAB Result | Actual Diagnosis |
|---|---|
| Benign lymphoid tissue | Acinic cell carcinoma Lymphoma Warthin tumor |
| Non-neoplastic gland | Acinic cell carcinoma Pleomorphic adenoma Squamous cell carcinoma, mucoepidermoid carcinoma Warthin tumor |
| Pleomorphic adenoma | Adenoid cystic carcinoma |
| Basal cell adenoma | Basal cell adenocarcinoma Adenoid cystic carcinoma |
| Adenoid cystic carcinoma | Pleomorphic adenoma Basal cell adenoma |
Lymph Node
Although a lateral neck mass may represent a wide variety of pathology, it is frequently the result of an enlarged lymph node. In patients with cervical lymphadenopathy, infectious, inflammatory, and neoplastic diagnoses must be considered. A patient’s age, recent health status, history of exposure to carcinogens, and clinical characteristics of the mass are important factors in determining the probability that a neck mass may be malignant. FNAB is frequently performed on cervical lymphadenopathy to assess for malignancy before surgical excision of the mass. If possible, the surgeon should avoid the clinical scenario of performing an excisional biopsy of a lymph node and being surprised by the final pathology revealing carcinoma.
As with thyroid, parathyroid, and salivary gland pathology, US guidance for FNAB of cervical lymphadenopathy offers significant benefit. For malignant adenopathy, significant necrosis can be present and US guidance to the more solid areas of the lymph node can produce a higher yield of diagnostic biopsies. Conversely, in patients with presumed cervical lymphadenitis, US guidance can be used to access small areas of suppuration within the node to obtain a specimen for gram stain and cultures. Even in cases of suspected benign disease resulting in cervical lymphadenopathy, biopsy may play a role in establishing a diagnosis. Kim and colleagues reported on the use of US-guided core biopsies of cervical adenopathy in patients without known malignancy. Diagnostic specimens were obtained in 94% with a reported accuracy of 98% based on histologic confirmation of excisional biopsies or regression of suspected benign lesions. The histologic diagnoses included reactive hyperplasia in 44 patients, tuberculosis in 37 patients, Kikuchi disease in 25 patients, metastasis in 16 patients, lymphoma in 16 patients, normal in 7 patients, and toxoplasmosis in 1 patient.
Drainage procedures
Fluid collections are frequently encountered in the head and neck region. These collections may be the consequence of an infection with abscess formation, hemorrhage into an existing cyst, or a postoperative complication. US-guided drainage may be an appropriate intervention, depending on the clinical scenario, and allow an otolaryngologist to avoid an open surgical procedure for the management of the disease ( Fig. 2 ). Chang and colleagues reported successful management of deep neck abscesses in 14 patients using US-guided drainage. Especially in patients with well-defined, unilocular abscesses, US drainage with or without drain placement should be considered without concern of complicating a future open drainage procedure if required.



