Purpose
To evaluate the efficacy and safety of twice-daily, preservative-free ketorolac 0.45% (Acuvail; Allergan, Inc, Irvine, California, USA) administration for treatment of inflammation and pain after cataract surgery.
Design
Prospective, randomized trial.
Methods
Two multicenter, double-masked studies randomized 511 cataract surgery patients (2:1) to receive twice-daily ketorolac 0.45% or vehicle in the operative eye for 16 days, beginning 1 day before surgery. The primary efficacy end point was the percentage of patients with a summed ocular inflammation score of 0 for anterior chamber cell and flare on postoperative day 14. The main secondary efficacy end point was the percentage of patients with no pain on postoperative day 1.
Results
On day 14, 52.5% of ketorolac patients and 26.5% of vehicle patients had an summed ocular inflammation score of 0 ( P < .001). On day 1, 72.4% of ketorolac patients and 39.7% of vehicle patients had a pain score of 0 ( P < .001). Median time to pain resolution was 1 day in the ketorolac group and 2 days in the vehicle group ( P < .001). The percentage of ketorolac and vehicle patients who had a +3-line or more improvement in best-corrected visual acuity from baseline was 60.5% versus 44.0% on day 14 ( P = .002). Overall, adverse events were more prevalent in the vehicle group than in the ketorolac group (48.5% vs 35.2%; P = .004). Burning or stinging (per a composite Medical Dictionary for Regulatory Activities) was reported by 1.5% of ketorolac patients and 0.6% of vehicle patients.
Conclusions
Twice-daily ketorolac 0.45% was well tolerated and effectively treated inflammation and pain following cataract surgery.
Ocular inflammation is a common complication of cataract extraction that is triggered primarily by surgical trauma. The inflammatory response includes activation of the arachidonic acid cascade and synthesis of prostaglandins by cyclooxygenase (COX) isoenzymes. Ocular inflammation can be uncomfortable, and if left untreated, it can cause pain and photophobia and may delay or, occasionally, permanently compromise visual rehabilitation. Uncontrolled inflammation and excessive production of prostaglandins also may result in a breakdown of the blood-retinal barrier and may lead to cystoid macular edema (CME), a frequent cause of visual loss that may occur even after uncomplicated cataract surgery.
Ophthalmic nonsteroidal anti-inflammatory drugs (NSAIDs) commonly are used to treat inflammation and pain after ocular surgery. Ketorolac is an NSAID that has been investigated for its analgesic and anti-inflammatory activities since the mid 1980s. Ketorolac inhibits both COX-1 and COX-2 isoenzymes and originally was formulated for 4-times–daily administration as ketorolac 0.5% (Acular; Allergan, Inc, Irvine, California, USA), indicated for treatment of inflammation following cataract extraction, and ketorolac 0.4% (Acular LS; Allergan, Inc), indicated for treatment of pain and burning or stinging after corneal refractive surgery. A recent study demonstrated the added benefit of perioperative ketorolac 0.4% over postoperative steroid alone in reducing the incidence of CME and macular thickening in cataract surgery patients who were considered to be at low risk of CME. Both ketorolac 0.4% and ketorolac 0.5% solutions, however, contain the preservative benzalkonium chloride, the surfactant octoxynol-40, and the metal-chelating agent sodium edetate and are associated with a high incidence of burning and stinging on instillation.
Ophthalmic ketorolac 0.45% solution (Acuvail; Allergan, Inc) is a new formulation of ketorolac that was developed to preserve the efficacy of prior formulations while enhancing tolerability coupled with a less frequent dosing regimen. Ketorolac 0.45% is preservative free and contains carboxymethylcellulose (CMC), which provides comfort and prolongs drug retention on the ocular surface. The purpose of this study was to evaluate the efficacy and safety of twice-daily ketorolac 0.45% for the treatment of inflammation and pain after cataract extraction.
Methods
Two multicenter, double-masked, vehicle-controlled, randomized trials enrolled patients with cataracts who were scheduled to undergo unilateral phacoemulsification with implantation of a posterior chamber intraocular lens. Study designs for both trials were identical. Patients 18 years of age and older who were likely to complete all study visits were eligible. Patients were excluded from the trials if they had uncontrolled ocular disease, active eye inflammation, a history of chronic or recurrent inflammatory eye disease, prior intraocular surgery other than refractive procedures, or known contraindications to any study medication. Patients also were excluded if they used ophthalmic analgesics, steroids or immunosuppressants, NSAIDs, or prostaglandins within 14 days before randomization or had a history of current or past use of tamsulosin hydrochloride (Flomax; Boehringer Ingelheim Pharmaceuticals, Inc, Ridgefield, Connecticut, USA, and Astellas Pharma US, Inc, Deerfield, Illinois, USA).
Study Treatments
Patients were randomized in a 2:1 ratio to receive either ketorolac 0.45% or vehicle in the operative eye for 16 days, beginning 1 day before cataract surgery and continuing to 14 days after the surgery day. On the day before surgery, patients instilled 1 drop of study medications twice daily approximately 12 hours apart. On the day of surgery, patients had a total of 6 drops of study medications, 1 drop on awakening, 3 drops each 20 minutes apart starting 2 hours before surgery, 1 drop before discharge, and 1 drop 12 hours after the first dose in the morning. Patients continued to instill 1 drop of study medications twice daily approximately 12 hours apart for 14 days after the surgery day. Acetaminophen was allowed as a rescue analgesic medication. Topical steroids were not allowed during the study. All patients received topical gatifloxacin 0.3% (Zymar; Allergan, Inc) 4 times a day in the operative eye for 9 days, starting 1 day before surgery. Beginning 1 hour before surgery, 3 drops of tropicamide 1% (Tropicamide Ophthalmic Solution, USP; Alcon Laboratories, Inc, Fort Worth, Texas, USA) and phenylephrine 2.5% (Phenylephrine Hydrochloride Ophthalmic Solution 2.5%; Alcon Laboratories, Inc) were instilled in the operative eye every 15 minutes to provide sufficient mydriasis.
Cataract Surgery
All patients underwent planned, unilateral, single-procedure, uncomplicated, extracapsular cataract extraction with posterior chamber intraocular lens implantation under topical or intracameral anesthesia, or both. Use of capsular stains was prohibited.
Outcome Measures
Patient screening was conducted during the month preceding cataract surgery, and randomization was performed 1 to 3 days before surgery. Patients were evaluated on postoperative days 1, 3, 7, and 14. The primary efficacy end point was the percentage of patients with a summed ocular inflammation score (SOIS) of 0 for anterior chamber cell and flare on day 14. The main secondary efficacy end point was the percentage of patients with no pain (grade = 0) on postoperative day 1. Additional study end points were the time to postoperative ocular pain resolution, proportion of patients completing the study without using any additional medications for inflammation or pain, treatment failure rate, pupil size after irrigation and aspiration, and safety. Visual acuity was evaluated as an ad hoc analysis.
Anterior chamber cells were graded on a 6-point scale, and anterior chamber flare was graded on a 5-point scale ( Table 1 ). The SOIS was calculated as the sum of scores for anterior chamber cells and flare in the operative eye and ranged from 0 (no inflammation) to 8 (severe inflammation). Patients called an interactive voice response system diary twice daily during the 2 weeks after the day of surgery, once in the morning and once in the evening approximately 1 hour after the study drug instillation. Using the interactive voice response system, patients rated the level of ocular pain on a 5-point scale (0 = none, 1 = mild, 2 = moderate, 3 = severe, 4 = intolerable) and stated if they have taken additional medications for inflammation, pain, or both. When additional medications were taken, a prespecified, last-observation-carried-forward algorithm was implemented to impute new values for the affected time points in the analysis of SOIS and pain scores. Time to resolution of ocular pain was analyzed by Kaplan-Meier estimation of the median. Treatment failure was defined as an anterior chamber cell score of 3 or more, an anterior chamber flare score of 3 or more, or an ocular pain score of 3 or more. Horizontal and vertical pupil diameters were measured immediately after irrigation and aspiration. Pupil area was calculated as π × 0.5 the horizontal diameter × 0.5 the vertical diameter. Best-corrected visual acuity (BCVA) was measured in Snellen equivalents using a logarithmic visual acuity chart at a test distance of 3 m.
| Anterior Chamber Cells | Anterior Chamber Flare | ||
|---|---|---|---|
| Grade | Cell Count | Grade | Flare |
| 0 | 0 | 0 | None |
| +0.5 | 1 to 5 | +1 | Faint |
| +1 | 6 to 15 | +2 | Moderate (clear iris and lens) |
| +2 | 16 to 25 | +3 | Marked (hazy iris and lens) |
| +3 | 26 to 50 | +4 | Intense (presence of fibrin or plastic aqueous) |
| +4 | >50 | ||
Statistical Analysis
Data from the 2 clinical trials were pooled for the purpose of presentation in this article. Missing values were imputed by last observation carried forward for anterior chamber inflammation, but were considered missing for pain on day 1. Between-group differences for the outcome variables were analyzed with a 2-sided Pearson chi-square or Fisher exact test. A P value < .05 was considered a significant difference.
Results
Patient Demographics and Disposition
Five hundred eleven patients were enrolled into 2 phase 3 trials between October 2007 and April 2008 at 48 investigational sites. Most patients (293/511; 57.3%) were female, and the median age was 70 years, ranging from 28 to 94 years ( Table 2 ). There were no statistically significant differences in gender ( P = .712), age ( P = .091), race ( P = .194), or iris color ( P = .284) between patients randomized to ketorolac 0.45% or vehicle.
| Vehicle (n = 171) | Ketorolac 0.45% (n = 340) | P Value | |
|---|---|---|---|
| Female, n (%) | 100 (58.5) | 193 (56.8) | .712 |
| Age (years) | .091 | ||
| Median | 68 | 70 | |
| Range | 35 to 85 | 28 to 94 | |
| Race, n (%) | .194 | ||
| White | 141 (82.5) | 295 (86.8) | |
| Nonwhite | 30 (17.5) | 45 (13.2) | |
| Iris color | .284 | ||
| Light | 108 (63.2) | 198 (58.2) | |
| Dark | 63 (36.8) | 142 (41.8) |
All enrolled patients were included in the intent-to-treat population. Of 511 patients, 423 (82.8%) patients completed the study ( Table 3 ). The most frequent reasons for discontinuation were adverse events in both treatment groups, followed by lack of efficacy in the vehicle group. A modified intent-to-treat population was used for the analysis of efficacy end points ( Table 3 ). This population was defined as all randomized patients who underwent cataract extraction with posterior chamber intraocular lens implantation in the operative eye. The safety population included all randomized patients who received at least 1 dose of study drugs ( Table 3 ).
| Vehicle | Ketorolac 0.45% | |
|---|---|---|
| Patients enrolled, n | 171 | 340 |
| Patients completed study, n (%) | 116 (67.8) | 307 (90.3) |
| Reasons for discontinuations, n (%) | ||
| Adverse events (ocular) | 30 (17.5) | 12 (3.5) |
| Protocol violation | 5 (2.9) | 7 (2.1) |
| Lack of efficacy | 10 (5.8) | 0 (0) |
| Lost to follow-up | 0 (0) | 1 (0.3) |
| Other b | 10 (5.8) | 13 (3.8) |
| Patients in efficacy analysis set, c n (%) | 161 (94.1) | 328 (96.5) |
| Patients in safety analysis set, n (%) | 163 (95.3) | 330 (97.0) |
a Acuvail; Allergan, Inc, Irvine, California, USA
b Included nonocular adverse events, consent withdrawal, placement of postsurgical patch, personal reasons, and presurgical or postsurgical use of disqualifying medications.
Efficacy Outcomes
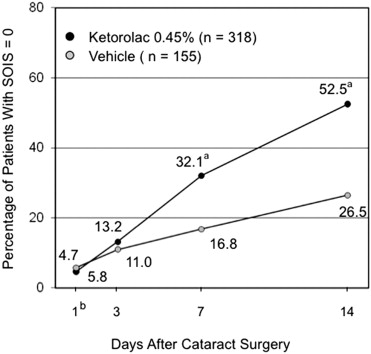
The percentage of ketorolac and vehicle patients with an SOIS of 0 was, respectively, 32.1% (102/318) versus 16.8% (26/155) on day 7 ( P < .001) and 52.5% (167/318) versus 26.5% (41/155) on day 14 ( P < .001; Figure 1 ). The percentage of patients with an SOIS of 0.5 or less was significantly higher in the ketorolac 0.45% group compared with the vehicle group on days 3 (120/318 [37.7%] vs 37/155 [23.9%]; P = .003), 7 (205/318 [64.5%] vs 55/155 [35.5%]; P < .001), and 14 (252/318 [79.2%] vs 73/155 [47.1%]; P < .001). On day 1, 233 of 322 (72.4%) of ketorolac patients and 62 of 156 (39.7%) vehicle patients had a pain score of 0 ( P < .001).
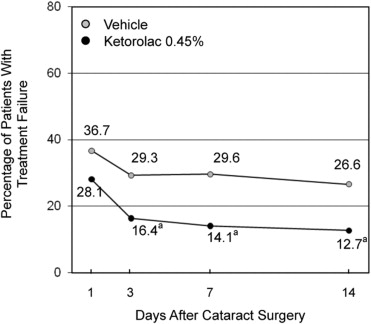
Median time to postoperative ocular pain resolution was 1.0 day in patients treated with ketorolac 0.45% and 2.0 days in patients treated with vehicle ( P < .001). The percentage of patients completing the study without using additional medications for inflammation or pain was 81.2% (264/325) in the ketorolac 0.45% group and 57.1% (92/161) in the vehicle group ( P = .001). The rate of treatment failure was significantly higher in patients treated with vehicle compared with those treated with ketorolac 0.45% on days 3, 7, and 14 ( Figure 2 ; P ≤ .001). The mean ± standard deviation pupil size after irrigation and aspiration was similar in the ketorolac 0.45% and vehicle groups (39.7 ± 12.4 mm 2 vs 38.7 ± 13.9 mm 2 ; P = .441). At baseline, the median BCVA was 20/40 (range, 20/12.5 to 20/800) in the ketorolac group and 20/50 (range, 20/10 to 20/400) in the vehicle group ( P = .321). The percentage of ketorolac and vehicle patients who had a +3-line or more improvement in BCVA from baseline was, respectively, 54.4% (167/307) versus 39.1% (54/138) on day 7 ( P = .003) and 60.5% (182/301) versus 44.0% (51/116) on day 14 ( P = .002; Figure 3 ).
Safety
Overall, the incidence of adverse events was significantly higher in the vehicle group than in the ketorolac 0.45% group (79/163 [48.5%] vs 116/330 [35.2%]; P = .004; Table 4 ). Elevation of intraocular pressure (IOP) was the only statistically significant adverse event that had a higher incidence in the ketorolac 0.45% group than in the vehicle group (19/330 [5.8%] vs 3/163 [1.8%]; P = .048). However, only 2 of 19 cases of increased IOP in the ketorolac group were considered treatment-related adverse events, and all but 1 case began on the first postoperative day ( Table 5 ). Compared with ketorolac patients, vehicle patients had significantly higher incidences of conjunctival hyperemia (15/330 [4.5%] vs 23/163 [14.1%]; P < .001), eye pain (14/330 [4.2%] vs 25/163 [15.3%]; P < .001), photophobia (3/330 [0.9%] vs 16/163 [9.8%]; P < .001), anterior chamber inflammation (1/330 [0.3%] vs 6/163 [3.7%]; P = .006), eyelid edema (0/330 [0%] vs 3/163 [1.8%]; P = .036), facial pain (0/330 [0%] vs 3/163 [1.8%]; P = .036), and uveitis (0/330 [0%] vs 3/163 [1.8%]; P = .036; Table 4 ). There were no other incidences of adverse events that were significantly different between groups.
| Vehicle (n = 163) | Ketorolac 0.45% (n = 330) | P Value | |
|---|---|---|---|
| All, n (%) | 79 (48.5) | 116 (35.2) | .004 |
| Increased IOP | 3 (1.8) | 19 (5.8) | .048 |
| Anterior chamber cell | 10 (6.1) | 17 (5.2) | NS |
| Conjunctival hyperemia | 23 (14.1) | 15 (4.5) | <.001 |
| Eye pain | 25 (15.3) | 14 (4.2) | <.001 |
| Iritis | 12 (7.4) | 14 (4.2) | NS |
| Anterior chamber flare | 8 (4.9) | 12 (3.6) | NS |
| Corneal edema | 10 (6.1) | 11 (3.3) | NS |
| Foreign-body sensation | 9 (5.5) | 11 (3.3) | NS |
| Headache | 6 (3.7) | 10 (3.0) | NS |
| Burning/stinging a | 1 (0.6) | 5 (1.5) | NS |
| Increased lacrimation | 4 (2.5) | 4 (1.2) | NS |
| Conjunctival hemorrhage | 1 (0.6) | 4 (1.2) | NS |
| Blurred vision | 1 (0.6) | 4 (1.2) | NS |
| Photophobia | 16 (9.8) | 3 (0.9) | <.001 |
| Conjunctival edema | 4 (2.5) | 3 (0.9) | NS |
| Eye irritation | 4 (2.5) | 3 (0.9) | NS |
| Eye pruritus | 3 (1.8) | 3 (0.9) | NS |
| Anterior chamber fibrin | 2 (1.2) | 2 (0.6) | NS |
| Anterior chamber inflammation | 6 (3.7) | 1 (0.3) | .006 |
| Iris hemorrhage | 2 (1.2) | 1 (0.3) | NS |
| Eyelid edema | 3 (1.8) | 0 (0) | .036 |
| Facial pain | 3 (1.8) | 0 (0) | .036 |
| Uveitis | 3 (1.8) | 0 (0) | .036 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


