Purpose
To compare the effects of 1 year of treatment with trimethoprim/sulfamethoxazole (TMP-SMZ) vs a placebo in reducing the risk of toxoplasmic retinochoroiditis recurrences during a 3-year follow-up period.
Design
Randomized, double-masked clinical trial.
Methods
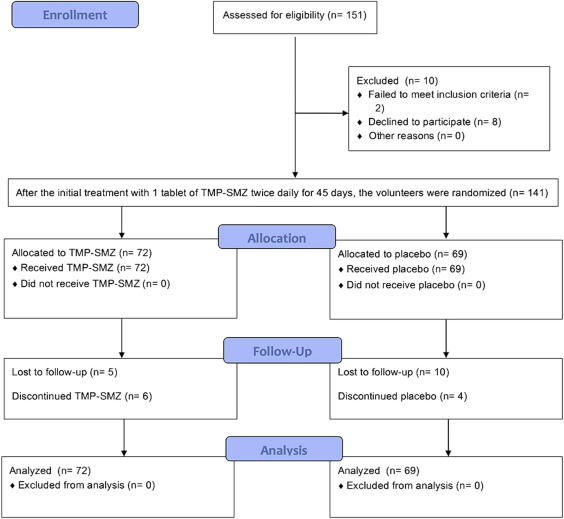
This cohort included 141 volunteers recruited in Campinas, Brazil. Inclusion criterion was unilateral active recurrent toxoplasmic retinochoroiditis. All volunteers were treated with 1 tablet of TMP-SMZ (160 mg/800 mg) twice daily for 45 days, and all lesions healed after this treatment. After this initial treatment, the volunteers were randomly assigned to Group 1 (1 TMP-SMZ tablet every 2 days for 311 days) or Group 2 (1 identical placebo tablet containing starch with no active ingredients every 2 days for 311 days). At the second- and third-year follow-up appointments, none of the volunteers received treatment unless a new recurrence episode had occurred. The primary outcomes were recurrent toxoplasmic retinochoroiditis within the first year of follow-up and recurrent toxoplasmic retinochoroiditis within the third year of follow-up.
Results
The cumulative probability of recurrence at 1, 2, and 3 years of follow-up were, respectively, 13.0% (9/69), 17.4% (12/69), and 20.3% (14/69) in the placebo group and 0% (0/72) in the TMP-SMZ group ( P < .001, log-rank test). There was no case of multiple recurrences in the same individual. No treatment-limiting toxicity or side effects were observed in either group. New recurrences were more frequent among female volunteers.
Conclusions
TMP-SMZ may be used safely for prophylaxis of recurrent toxoplasmic retinochoroiditis, with long-term benefits.
Ocular toxoplasmosis is responsible for most cases of infectious posterior uveitis in the world and is an important cause of blindness and visual impairment.
The exact causes and pathogenesis of recurrences in ocular toxoplasmosis are not known. During the chronic phase of toxoplasmic infections, short and usually self-limiting periods of parasite reactivation regularly occur and cause the typical presentation of recurrent toxoplasmic retinochoroiditis. The mechanisms of action involved in the switch from latent to proliferative forms of parasites are not well understood. Numerous hypothetical triggers have been suggested, including immune response and hormonal status of the host, human leukocyte antigen type, autoimmune or hypersensitivity reactions to exposed toxoplasmic antigens, and parasite-related factors, such as the mechanical rupture of cysts caused by parasite multiplication, the release of toxins or lytic enzymes by the parasite, or reinfections with other strains of parasites.
It has been postulated that recurrences are associated with the proliferation of live organisms that emerge from tissue cysts. Over time, the viability of tissue cysts in the retina decreases and the cysts eventually die, reducing the pool of cysts from which reactivation can occur. As a consequence, the probability of recurrences decreases after each active episode. This factor supports the argument that an increased risk of recurrence appears during the first year following active retinochoroiditis. Other factors that have been argued as having an influence on recurrences include changes in tissue cysts with reduced release of parasites or antigens, trauma, endocrine fluctuations, and transient humoral or cellular immunoreactivity.
Silveira and associates and Commodaro and associates assert that further research is required to evaluate the possible beneficial effect of long-term treatments on the prevention of ocular toxoplasmosis recurrences. It has been hypothesized that long-term treatment with trimethoprim-sulfamethoxazole (TMP-SMZ) suppresses the proliferation of the occasional parasites that emerge from tissue cysts, thus allowing for the establishment of effective host control before the parasite can proliferate to an extent that causes clinically apparent lesions.
An interesting report by Silveira and associates with a 10-year follow-up period suggested that the prophylactic treatment effect disappears when the treatment is stopped; however, their results must be considered carefully. It was an open-label trial (non-placebo-controlled, nonmasked) with a loss of follow-up of 50%. This prophylactic treatment may provide good effects in a follow-up period shorter than 10 years, though the former study was not able to detect this. This finding suggests the need for additional follow-up studies.
In our previous publication, 1 year of intermittent treatment with trimethoprim (160 mg)/sulfamethoxazole (800 mg) in the form of 1 tablet every 2 days reduced the rate of recurrent toxoplasmic retinochoroiditis.
The purpose of this trial was to compare the effects of 1 year of treatment with TMP-SMZ vs placebo on reducing the risk of toxoplasmic retinochoroiditis recurrences in 3 years of follow-up after a recurrent episode.
Methods
This study was a single-center, prospective, randomized, double-masked clinical trial. Ethics committee approval (institutional review board) was obtained, and all participants gave informed consent (National Bioethics Commission of Brazil Identifier No.: 0613.0.146.000-10). The trial was registered in October 2011 and began in November 2011 (Influence of Trimethoprim-Sulfamethoxazole on the Recurrence of Ocular Toxoplasmosis. Clinicaltrials.gov Identifier No.: NCT01449877 ; http://clinicaltrials.gov/show/NCT01449877 ).
The original manuscript (first report) included the first 100 subjects who completed the 1-year follow-up. This cohort included all 151 subjects recruited from a uveitis clinic at a public hospital in Campinas, Brazil. The only incentive provided was free medication. The subjects were followed up for at least 36 months. The inclusion criterion was unilateral active recurrent toxoplasmic retinochoroiditis (defined as a new focal area of necrotizing retinochoroiditis with active inflammation either adjacent to or remote from preexisting retinochoroidal scars, with IgG that was positive for toxoplasmosis). There were no IgM+ cases. Subjects who were under 18 years of age, were immunocompromised (eg, AIDS patients), were undergoing immunosuppressive treatments, or had concomitant retinochoroiditis from other causes (eg, tuberculosis) were excluded.
All subjects were treated for active toxoplasmic retinochoroiditis with 1 tablet of TMP-SMZ (160 mg/800 mg) twice daily for 45 days, and all lesions healed after this treatment (there were no subjects with unhealed lesions). Subsequently, 10 subjects dropped out of the study ( Figure 1 ). The remaining subjects were randomly assigned to Group 1 (1 TMP-SMZ tablet every 2 days for 311 days) or to Group 2 (1 identical placebo tablet containing starch with no active ingredients every 2 days for 311 days). The regimen was chosen empirically based on a mix of 3 factors: the local experts’ experience, patient compliance, and a previous report by Silveira and associates regarding toxoplasmic retinochoroiditis prophylaxis. It was not based on pharmacokinetic data.
Randomization was 1:1. It was stratified by sex, and block sizes of 4 were used. One nurse generated the random allocation sequence, and another nurse enrolled and assigned the participants to the interventions in a masked fashion. Compliance with the drug regimen was evaluated by a count of the number of remaining tablets.
At the second-year and third-year follow-up appointments, the subjects did not receive treatment unless a new recurrence episode had occurred. Recurrences were treated with 1 tablet of TMP-SMZ (160 mg/800 mg) twice daily for 45 days. Patients were instructed to attend follow-up consultations every 3 months or when they experienced symptoms consistent with recurrent disease, such as redness, decreased vision, eye pain, and photophobia. Five patients in Group 1 and 10 patients in Group 2 missed their follow-up visits because they moved to other cities. Six patients in Group 1 and 4 patients in Group 2 discontinued interventions.
The trial was sponsored by the São Paulo State Research Foundation (FAPESP), Protocol No. 2010/15980-2. Trimethoprim/sulfamethoxazole tablets cost US $0.31 each and placebo tablets cost US $0.15 each.
Data were collected using a medical history form completed by the physician during the first medical examination. Best-corrected visual acuity (BCVA) based on ETDRS charts, as well as biomicroscopy, tonometry, indirect ophthalmoscopy with location of scars, recurrence of toxoplasmic retinochoroiditis, and medical events, were all recorded on a standardized form by a member of the medical staff in a masked fashion. Side effects were defined as any symptoms, signs, or biochemical abnormalities possibly related to treatment.
The primary outcomes were recurrent toxoplasmic retinochoroiditis within the first year of follow-up and recurrent toxoplasmic retinochoroiditis within the third year of follow-up.
Sample size calculations based on presumed recurrence rates of 0% in the treatment group and 15% in the placebo group indicated that a sample size of 35 in each group would be significant for detecting a difference of this magnitude with a power of 80% and type 1 error probability of 5%. However, to account for losses in follow-ups and based on feedback obtained after the study was begun, 151 subjects were enrolled.
Descriptive statistics were calculated. Continuous data were expressed as the mean, median, and standard deviation (SD). Between-group differences of continuous variables were compared using the Mann-Whitney U test, and categorical variables were compared using χ 2 test or Fisher exact test when appropriate. The probabilities of recurrence and of missing follow-up visits were assessed using the Kaplan-Meier survival analysis (log-rank test). Intention-to-treat analyses were conducted using SPSS, version 21 (IBM Corporation, Armonk, New York, USA). P values were 2-tailed. Statistical significance was set at .05.
Results
Between August 24, 2011 and February 1, 2013, 141 subjects were enrolled at a public hospital in Campinas, São Paulo State, Brazil and were randomized either to therapy using trimethoprim/sulfamethoxazole (72 subjects) or to placebo (69 subjects) ( Figure 1 ). The mean age was 33 (SD 13) years, and 75 subjects (53.2%) were female. Age, sex distributions, lesion location, and the frequency of contralateral lesions were similar between the 2 groups ( Table 1 ). The mean interval between the pre-enrollment recurrence episode and the recurrence observed during study follow-up was 263 (SD 219) days (median: 144 days).
| Patients Treated With TMP-SMZ (N = 72) | Patients Treated With Placebo (N = 69) | P | |
|---|---|---|---|
| Age (y), mean (SD), median | 32 (13), 33 | 33 (14), 33 | .329 a |
| Male-to-female ratio | 36:36 | 30:39 | .438 b |
| Macular involvement/peripheral involvement at study entry, n | 22/50 | 24/45 | .593 b |
| Contralateral scars c | 10 | 7 | .495 b |
The Kaplan-Meier survival analysis was used to compare missed follow-up visits between the 2 groups. No significant difference was found. The cumulative probability of missing follow-ups at 3 years was 14.5% (10/69) in the placebo group (mean follow-up of 984 days) and 6.9% (5/72) in the TMP-SMZ group (mean follow-up of 1046 days; P = .139, log-rank test).
Kaplan-Meier survival analysis was used to compare recurrence between the 2 groups ( Figure 2 ). A significantly higher probability of recurrence was observed in the placebo group relative to the TMP-SMZ group. The cumulative probability of recurrence at 1, 2, and 3 years of follow-up was, respectively, 13.0% (9/69), 17.4% (12/69), and 20.3% (14/69) in the placebo group and 0% (0/72) in the TMP-SMZ group ( P < .001, log-rank test). There were no cases of multiple recurrences in the same individual.
The mean changes in BCVA within 36 months were 22 (SD 20) letters (range −4 to 54) in the TMP-SMZ group and 22 (SD 18) letters (range −19 to 54) in the placebo group ( P = .768, Table 2 and Figure 3 ).
| Patients Treated With TMP-SMZ (N = 72) | Patients Treated With Placebo (N = 69) | P | |
|---|---|---|---|
| Baseline BCVA b | 55 (SD 21) letters (20/80) | 53 (SD 20) letters (20/100) | .151 a |
| BCVA after 36 months b | 78 (SD 18) letters (20/32) | 74 (SD 19) letters (20/32) | .225 a |
| Change in BCVA c | 22 (SD 20) letters | 22 (SD 18) letters | .136 a |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


