Purpose
To evaluate the effects of transpupillary thermotherapy and intravitreal bevacizumab injection on serous macular detachment and cystoid macular edema (CME) associated with circumscribed choroidal hemangioma.
Design
Retrospective, interventional case series.
Methods
We reviewed the records of 12 patients with circumscribed choroidal hemangioma treated with transpupillary thermotherapy and/or intravitreal injection of bevacizumab. We assessed changes in best-corrected visual acuity (BCVA), central foveal thickness by optical coherence tomography, and resolution of serous macular detachment and CME.
Results
Six of 8 patients treated with transpupillary thermotherapy showed complete resolution of serous macular detachment and CME and the median minimal angle of resolution (logMAR) BCVA improved from 0.85 to 0.35 ( P = .026). Among these 6 patients, 1 had no recurrence for 86 months and 5 had sustained resolution of serous macular detachment for a mean duration of 32.8 months before recurrence. Among the 9 patients treated with bevacizumab (including 5 patients who had transpupillary thermotherapy as a primary treatment), 5 showed resolution of serous macular detachment and the median logMAR BCVA improved from 0.7 to 0.5 ( P = .042). Among these 5 patients, 3 had sustained resolution for a mean duration of 5.7 months and 2 showed recurrent serous macular detachment after 3 and 12 months.
Conclusion
Transpupillary thermotherapy and intravitreal bevacizumab appear effective in the management of symptomatic circumscribed choroidal hemangioma, although recurrence of serous macular detachment and CME developed after long-term follow-up of transpupillary thermotherapy, and the duration of treatment effectiveness appears to be short with bevacizumab.
Circumscribed choroidal hemangioma produces visual symptoms attributable to the accumulation of submacular fluid or intraretinal cystoid edema. Management depends upon symptom severity and the presence of exudative retinal detachment. As symptomatic cases of circumscribed choroidal hemangioma are associated with an unfavorable visual prognosis, treatment should be considered when symptoms present.
A number of different treatment modalities including laser photocoagulation, cryotherapy, radiotherapy, transpupillary thermotherapy, and photodynamic therapy (PDT) have been used in the management of circumscribed choroidal hemangioma. Recently, anti–vascular endothelial growth factor (VEGF) has emerged as a treatment option for circumscribed choroidal hemangioma–associated exudative retinal detachment or macular edema, especially for subfoveal lesions. Although PDT with verteporfin appears to produce the best clinical results in terms of safety and efficacy, it is an expensive therapy and thus impractical for some patients with financial limitations.
In this paper, we evaluate the effectiveness of transpupillary thermotherapy and intravitreal injection of bevacizumab (Avastin; Genentech Inc, South San Francisco, California, USA) on serous macular detachment and cystoid macular edema (CME) associated with circumscribed choroidal hemangioma.
Methods
We retrospectively reviewed the medical records of all patients with circumscribed choroidal hemangioma examined and treated at Yonsei University Eye and ENT Hospital between March 2002 and October 2010. Among the patients with circumscribed choroidal hemangioma, those treated with transpupillary thermotherapy and/or intravitreal injection of bevacizumab for serous macular detachment and CME were selected for analysis. Circumscribed choroidal hemangioma was diagnosed based on clinical appearance, fluorescein or indocyanine green (ICG) angiography, and ultrasonography.
Assessment of patients included the minimal angle of resolution (logMAR) best-corrected visual acuity (BCVA) measurement with the Snellen acuity chart, intraocular pressure measurement, slit-lamp biomicroscopy, dilated funduscopic examination, fluorescein and ICG angiography, B-scan ultrasonography, and optical coherence tomography (OCT) (Stratus III OCT, Carl Zeiss, Dublin, California, USA; or Spectralis HRA + OCT, Heidelberg Engineering, Heidelberg, Germany). B-scan ultrasonography was used to evaluate the thickness of the lesion before and after treatment. OCT was also performed before and after treatment for the evaluation of subretinal fluid or CME and central foveal thickness measurements. The distance between the vitreoretinal interface and retinal pigment epithelial layer at the foveal center was measured to determine central foveal thickness using the Spectralis OCT software. The average central foveal thickness from vertical and horizontal scans of the center of the fovea was used for analysis.
Transpupillary thermotherapy was performed under topical anesthesia via a dilated pupil. Patients were treated with an infrared diode laser at 810 nm with a slit-lamp biomicroscope delivery system. We used the Mainster contact lens in which the actual retinal spot size was 5% greater than the thermotherapy spot size. The spot size was chosen based on the width of the tumor, with 3.0 mm being the most frequently used spot size. Each tumor was covered entirely with confluent laser spots, with power ranging from 400 to 800 mW to induce a grayish reaction with 1 minute of exposure at each spot. The center of the macula was spared during transpupillary thermotherapy in cases involving the fovea.
Intravitreal injection of bevacizumab was performed in the operating room using an aseptic technique to minimize the risk of infection. The eye was topically anesthetized with 0.5% proparacaine drops (Alcane; Alcon Laboratories, Fort Worth, Texas, USA) and prepared using 5% povidone-iodine. Bevacizumab 1.25 mg was injected 3.0 or 3.5 mm posterior to the limbus through the pars plana using a 30-gauge needle, after which optic nerve head perfusion was confirmed immediately by indirect ophthalmoscopy.
General patient data collected included age, sex, history of systemic illnesses, and previous ocular problems. Ocular data included visual acuity, tumor location, and largest tumor diameter and thickness (in millimeters, measured by B-scan ultrasonography). OCT data included the presence of subretinal fluid, CME, and central foveal thickness.
Data were analyzed for changes in visual acuity and resolution of subretinal fluid and CME, changes in central foveal thickness as determined by OCT, and changes in tumor thickness at initial and final visits.
Results
From 2002 to 2010, 51 patients with choroidal hemangioma were identified, of which 43 had circumscribed tumors. Of these 43 patients, 30 were treated for symptomatic circumscribed choroidal hemangioma. Six patients were treated with gamma-knife surgery, and 1 patient had vitrectomy surgery for extensive exudative retinal detachment. Three patients were treated with PDT, and 20 patients were treated with transpupillary thermotherapy and/or intravitreal injection of bevacizumab. Of these 20 patients, 12 were followed up for a minimum of 3 months and were included in our analysis. Eight patients were treated with transpupillary thermotherapy, and 9 patients were treated with intravitreal bevacizumab injection. Among those receiving transpupillary thermotherapy, additional treatments were performed if serous macular detachment or CME persisted 2 months following initial transpupillary thermotherapy. Five of the 8 patients who had undergone serial transpupillary thermotherapy also received intravitreal bevacizumab injection because of recurrent or persistent serous macular detachment.
None of the patients included in our analysis had been previously treated for circumscribed choroidal hemangioma except for 1 patient (Patient 10), who had undergone barrier photocoagulation around the tumor at another hospital.
Outcome of Transpupillary Thermotherapy
The demographics, ocular characteristics, and treatment results of the 8 patients who received transpupillary thermotherapy as their primary treatment are shown in Table 1 .
| No. | Age | Sex | Tumor Location | No. of TTT | Visual Acuity (Snellen) | Initial Basal Dia (mm) | Initial Ht. (mm) | Last Ht. (mm) | SMD Resolution (Duration, mo) | CME | Add IVB | FU (mo) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre TTT | Post TTT | Pre TTT | Post TTT | |||||||||||
| 1 | 40 | M | SF | 2 | 20/2000 | 20/1000 | 8.5 | 3.4 | 3.3 | Complete (17) | Yes | No | No | 62 |
| 2 | 35 | F | PP | 2 | 20/200 | 20/100 | 10.6 | 4.7 | 4.7 | Complete (12) | No | No | No | 26 |
| 3 | 48 | F | PP | 3 | 20/60 | 20/25 | 6.8 | 3 | 2.2 | Complete (86) | No | No | No | 92 |
| 4 | 63 | M | PF | 2 | 20/400 | 20/50 | 8.5 | 3.4 | 3.4 | Complete (40) | Yes | No | Yes | 52 |
| 5 | 60 | M | SF | 3 | 20/200 | 20/100 | 9.4 | 3.5 | 3.5 | Persistent | No | No | Yes | 39 |
| 6 | 62 | M | PP | 2 | 20/50 | 20/25 | 7.2 | 1.2 | 1.2 | Complete (50) | Yes | No | Yes | 71 |
| 7 | 45 | M | PF | 3 | 20/100 | 20/30 | 7.5 | 3.5 | 3.5 | Complete (45) | No | No | Yes | 53 |
| 8 | 48 | M | PF | 3 | 20/40 | 20/40 | 9.5 | 3.7 | 3.7 | Persistent | No | No | Yes | 29 |
The mean age at first treatment was 50.1 years (median, 48; range, 35–63 years), and mean greatest tumor diameter and thickness were 8.5 mm (median, 8.49; range, 6.8–10.6) and 3.3 mm (median, 3.5; range, 1.2–4.7 mm), respectively. The mean number of treatments received was 2.5 (median, 2.5; range, 2–3), and patients were followed up for a mean duration of 53 months (median, 52.5; range, 26–92) ( Table 1 ).
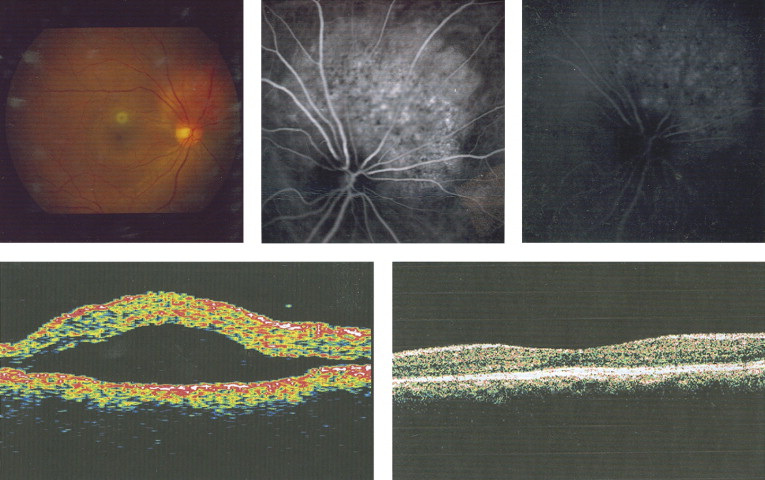
Of the 8 patients with serous macular detachment in the transpupillary thermotherapy group, 6 achieved complete resolution following treatment. Three patients (Patients 1, 4, and 6) in the transpupillary thermotherapy group had concomitant CME with serous macular detachment, all of whom had resolution of CME. Of the 6 patients who had complete resolution of serous macular detachment, 5 had a recurrence after a mean 32.8 months (median, 45 months; range, 12–50), whereas 1 (Patient 3) had complete resolution of serous macular detachment for 86 months without recurrence ( Figure 1 ) . The overall mean duration of resolution of serous macular detachment was 41.7 months (median, 42.5 months).
All 6 patients who had complete resolution of serous macular detachment had improved BCVA, from a median logMAR BCVA of 0.85 to 0.31 ( P = .027, Wilcoxon signed rank test). The overall median logMAR BCVA of the 8 patients in this group also demonstrated significant improvement, from 0.85 to 0.35 ( P = .026, Wilcoxon signed rank test) after transpupillary thermotherapy.
There was no significant decrease in tumor size after transpupillary thermotherapy regardless of whether or not resolution of serous macular detachment or CME occurred.
Outcome of Bevacizumab Treatment
The demographics, ocular characteristics, and treatment results of the 9 patients who were treated with intravitreal bevacizumab injection are shown in Table 2 . Of the 9 patients in this treatment group, 4 received intravitreal injection of bevacizumab as the primary treatment for serous macular detachment associated with circumscribed choroidal hemangioma, while 5 initially underwent transpupillary thermotherapy and received intravitreal bevacizumab injection as a secondary treatment for recurrent serous macular detachment.
| No. | Age | Sex | Tumor Location | TTT to IVB (mo) | No. of IVB | Visual Acuity (Snellen) | SMD Resolution (Duration, mo) | CFT (μm) | CME | FU (mo) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre IVB | Post IVB | Pre IVB | Post IVB | Pre IVB | Post IVB | ||||||||
| 4 | 67 | M | SF | 42 | 2 | 20/200 | 20/200 | Complete (7) | 525 | 353 | Yes | Yes | 7 |
| 5 | 59 | M | SF | 16 | 2 | 20/400 | 20/200 | Persistent | 317 | 447 | Yes | Yes | 19 |
| 6 | 67 | M | PP | 52 | 3 | 20/100 | 20/40 | Complete (12) | 444 | 251 | Yes | Yes | 18 |
| 7 | 50 | M | PF | 45 | 2 | 20/100 | 20/100 | Persistent | 308 | 322 | Yes | Yes | 4 |
| 8 | 48 | M | PF | 22 | 2 | 20/60 | 20/60 | Persistent | 394 | 215 | No | No | 4 |
| 9 | 46 | F | EF | NA | 1 | 20/30 | 20/20 | Complete (4) | 415 | 232 | No | No | 4 |
| 10 | 44 | F | PP | NA | 1 | 20/800 | 20/20 | Complete (6) | 923 | 199 | No | No | 6 |
| 11 | 29 | F | EF | NA | 1 | 20/50 | 20/50 | Persistent | 430 | 206 | No | No | 3 |
| 12 | 47 | F | SF | NA | 2 | 20/200 | 20/100 | Complete (3) | 514 | 330 | No | No | 11 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


