Purpose
To report the effect of repeated corneal swabbing in patients with microsporidial keratoconjunctivitis.
Design
Retrospective noncomparative case series.
Methods
Sixteen eyes of 14 healthy patients with microsporidial keratoconjunctivitis were diagnosed based on the detection of microsporidia in corneal scrapings using Gram stain, the modified Kinyoun acid-fast stain, or both. Polymerase chain reaction plus gene analysis of the microsporidian 16S ribosomal RNA had been performed in 10 patients who sought treatment between 2010 and 2011. Some of the lesions were scraped for procurement of specimens. The remaining lesions were wiped off gently by cotton swabs. Repeated swabbing was performed if infection persisted or new lesions were observed at follow-up. To prevent secondary bacterial infection, 0.3% norfloxacin or 0.25 % chloramphenicol were prescribed.
Results
The mean age was 52.2 years. All patients had the characteristic disseminated, punctate, slightly elevated, white epithelial lesions. The denser white lesions could be removed easily after gentle swabbing, and most epithelium remained intact. The 10 cases with positive polymerase chain reaction results were all identified to be Vittaforma corneae . The mean number of corneal swabbing was 3.3, and the mean disease resolution time was 6.6 days. No patients had recurrence or loss of visual acuity at last follow-up.
Conclusions
Repeated swabbing effectively can eradicate corneal epithelial microsporidial lesions in approximately 1 week. It is easy to perform, less painful, and more acceptable for the patients.
Microsporidia are spore-forming, obligate intracellular eukaryotic pathogens that infect both invertebrate and vertebrate. Recent genome-wide analyses support that these organisms evolved from ancestral sexual fungi. They are considered to be opportunistic pathogens of humans by causing infections in various organs, including the eyes. In the past, ocular involvement manifested as epithelial keratoconjunctivitis in patients with AIDS and as stromal keratitis in immunocompetent individuals.
The prevalence of microsporidial keratoconjunctivitis in immunocompetent individuals has been known to increase significantly in recent years. However, no conclusive regimen for the treatment of this disease has been documented. Successful results were reported for topical treatment with fumagillin with or without oral albendazole. But because fumagillin acts in a parasitistatic rather than a parasiticidal manner, it required a prolonged treatment in some cases. Other treatment options include oral albendazole monotherapy, topical fluoroquinolone monotherapy, 0.1% propamidine isethionate, 0.02% polyhexamethylene biguanide (PHMB), and topical 1% voriconazole.
The characteristic appearance of microsporidial keratoconjunctivitis is the development of multiple whitish, slightly elevated epithelial lesions. Smear of these lesions usually revealed abundant microsporidial spores. Debridement of corneal epithelium can debulk the micro-organisms, and this seems to be effective on the disease treatment in some cases. We found that the denser the whitish epithelial lesions, the easier for them to be wiped off by cotton swabs. After swabbing, most of the epithelium not involved remained intact. The current study aimed specifically at the effectiveness and benefits of repeated corneal swabbing for the treatment of microsporidial keratoconjunctivitis.
Methods
This retrospective, noncomparative case series included 16 eyes of 14 patients treated between May 2006 and August 2011 at the Department of Ophthalmology, Taipei Veterans General Hospital. Microsporidial keratoconjunctivitis was diagnosed based on the presence of microsporidial spores by staining procedures. All patients underwent repeated corneal swabbing. Patients who underwent keratectomy with a blade to remove all the epithelium within the involved area were excluded.
For collecting specimens, a few whitish epithelial lesions were scraped from each patient after topical anesthesia using either a no. 26 needle or sterile McPherson Micro-Tying forceps (Albert Heiss, Tuttlingen, Germany) under a slit-lamp biomicroscope. This caused only small epithelium defects. The scraped epithelial specimens were smeared on slides and stained with Gram stain, modified Kinyoun acid-fast stain, or both. The remaining whitish epithelial lesions on the cornea were wiped gently with cotton swabs. This action was like erasing a chalkboard. The cotton swab was put in a 1.5 mL microcentrifuge tube (Molecular BioProducts, San Diego, California, USA) for polymerase chain reaction (PCR) analysis. DNA was extracted using the Gentra Puregene kit (Qiagen, Valencia, California, USA). Microsporidial PCR analysis using panmicrosporidian primers with targeting on the 16S rRNA was processed according to procedures described by Joseph and associates. The PCR products were cloned with a TOPO TA cloning kit (Invitrogen, Carlsbad, California, USA) and were sequenced at Mission Biotech (Taipei, Taiwan).
Topical antibiotics were prescribed 4 times daily to prevent secondary infection after corneal scraping. The topical antibiotics were tapered or discontinued according to epithelium healing condition. Each patient was followed up every day or every other day in the first week and then once or twice weekly until their epithelial lesions disappeared completely. Repeated swabbing was performed whenever the epithelial lesions were observed. If the intraocular pressure (IOP) was normal (≤ 21 mm Hg), low-potency topical corticosteroid (0.02% fluorometholone) 4 times daily was prescribed at the beginning to decrease ocular surface inflammation and to prevent subsequent development of nummular anterior stromal infiltration. The topical corticosteroid was discontinued after resolution of the keratoconjunctivitis.
Results
The Table shows the clinical characteristics, treatment details, and outcomes. Of these 14 patients, Patients 1, 2, 3, 5, 6, and 7 were reported previously. They are also included here with more detailed information of treatment. There were 8 (57%) men and 6 (43%) women with a mean age of 52.2 years, ranging from 23 to 78 years. Nine (64.3%) of these patients had a history of exposure to hot springs, 1 (7.1%) patient wore contact lenses, 2 (14.3%) patients had soil contact, and the other 2 (14.3%) patients had a history of swimming in public pools. None had a history of trauma or contact with animals. Eleven (78.6%) of these patients were misdiagnosed in another hospital: 8 (57.1%) patients as having acute conjunctivitis, 1 (7.1%) patient as having scleritis, and 2 (14.3%) patients as having herpes keratitis. Patient 6 had a long history of infection and she was treated for more than 1 month before her first visit to our department. Both Patients 6 and 12 had bilateral involvement. Patient 6 demonstrated infection in both eyes at presentation. Patient 12 initially showed infection in his left eye. Then, at follow-up 13 days later, the right eye was also involved. The follow-up periods in this study ranged from 5 days to 47 months, with median of 1 month.
| No. | Age (y) | Sex | Initial BCVA | PCR Results | Treatment | Time to Resolution (Days) | Final BCVA | |
|---|---|---|---|---|---|---|---|---|
| No. of Corneal Swabbings | Topical Antibiotics | |||||||
| 1 | 71 | M | L: 20/63 | ND | 3 | 0.3% norfloxacin | 4 | 20/20 |
| 2 | 23 | M | L: 20/63 | ND | 3 | 0.3% norfloxacin | 5 | 20/20 |
| 3 | 55 | M | R: 20/200 | ND | 5 | 0.3% norfloxacin | 7 | 20/20 |
| 4 | 25 | F | R: 20/25 | ND | 3 | 0.3% norfloxacin | 11 | 20/20 |
| 5 | 48 | F | L: 20/25 | Vc | 4 | 0.3% norfloxacin | 6 | 20/20 |
| 6 | 68 | F | R: 20/20 | Vc | 4 | 0.3% norfloxacin | 6 | 20/20 |
| L: 20/25 | ND | 4 | 0.3% norfloxacin | 6 | 20/20 | |||
| 7 | 62 | M | R: 20/100 | Vc | 3 | 0.3% norfloxacin | 7 | 20/20 |
| 8 | 55 | F | R: 20/25 | Vc | 4 | 0.3% norfloxacin | 7 | 20/20 |
| 9 | 55 | M | R: 20/30 | Vc | 3 | 0.3% norfloxacin | 9 | 20/25 |
| 10 | 55 | M | L: 20/20 | Vc | 2 | 0.3% norfloxacin | 5 | 20/20 |
| 11 | 36 | F | R: 20/32 | Vc | 2 | 0.25% chloramphenicol | 6 | 20/20 |
| 12 | 60 | M |
|
| 4 | 0.25% chloramphenicol | 8 | 20/16 |
| 2 | 0.25% chloramphenicol | 4 | 20/20 | |||||
| 13 | 40 | F | L: 20/20 | Vc | 3 | 0.25% chloramphenicol | 7 | 20/20 |
| 14 | 78 | M | R: 20/63 | Vc | 4 | 0.25% chloramphenicol | 8 | 20/25 |
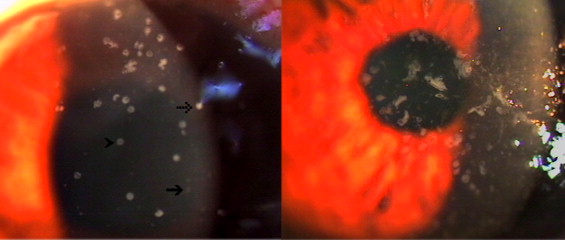
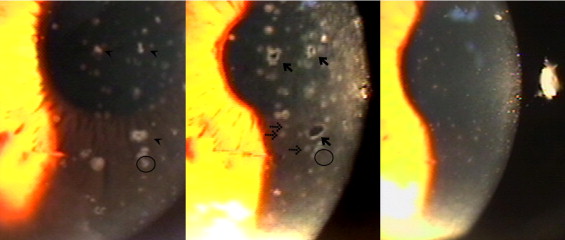
Initial symptoms included red eye, pain, blurry vision, epiphora, and swelling of the eyelid. Tenderness of the preauricular lymph nodes was noted in 2 (14.3%) patients. Slit-lamp biomicroscopy disclosed mild to severe conjunctivitis in all patients. All patients manifested with typical multiple, whitish, raised epithelial lesions, varying in size and without stromal involvement. Four typical patterns of the epithelial lesions were noted: (1) smaller, faint white dot or round lesions, (2) denser white round-to-oval lesions, (3) bizarre shape (pleomorphic lesions, varying in size, and usually larger than the round-to-oval type), and (4) target-like lesions with a transparent hollow center ( Figure 1 ). After swabbing, the denser white lesions usually disappeared. Some left a punched-out epithelial defect ( Figure 2 ). The defects with a white rim resembled the target-like lesions, which always had disappeared at follow-up. The smaller faint lesions that could not be removed with swabbing became larger and more prominent. Some new faint lesions developed immediately after swabbing. Both lesions usually also had disappeared at follow-up. The noninvolved epithelium normally remained intact after a gentle swabbing. At follow-up, the lesions that reappeared were not always at the same location as previously observed ( Figure 2 ). In addition to the typical lesions, the right eye of Patient 12 also had tiny elevated epithelial lesions with a coarse punctate surface that stained poorly with fluorescein. These lesions had similar morphologic features as those of Thygeson superficial punctate keratitis.
Results of microsporidial PCR studies on corneal scrapes obtained from 11 eyes of 10 patients revealed 250- to 280-bp amplicon. The gene sequences in all cases disclosed similarity of 99% to 100% compared with the Vittaforma corneae ( V. corneae ) 16S rRNA ( www.ncbi.nLm.nih.gov/GenBank ). The sequences of clinical specimens from the left eye of Patient 12 and from Patients 5 and 10 were identical to the GenBank sequence of V. corneae (accession number HM854229.1). The other sequences have been deposited into GenBank (accession numbers JX049113, JX049114, JX049115, and JX049116).
The mean number of corneal swabbings was 3.0 in patients with 0.25% chloramphenicol and 3.5 in patients with 0.3% norfloxacin ( Table ). All except Patient 14 were prescribed 0.02% fluorometholone. Rapid improvement in clinical signs and symptoms was observed after repeated swabbing. The resolution time, defined as the time to reach complete disappearance of epithelial lesions, was approximately 1 week (mean, 6.6 days; range, 4 to 11 days). An identical mean of 6.6 days was obtained from patients treated with norfloxacin and patients treated with chloramphenicol. No systemic antibiotic was prescribed to any of these patients. No patient lost best-corrected visual acuity or had recurrence at the last follow-up.
Elevation of IOP was noted in Patients 13 and 14, who had no history of glaucoma. Both patients showed no inflammation in the anterior chamber. Patient 13 had an IOP of 23 mm Hg in both eyes at presentation. The IOP elevated to 39 mm Hg in the left diseased eye on the third day of treatment and the IOP in the other eye was 20 mm Hg. Brimonidine tartrate ophthalmic solution 0.15% then was prescribed and fluorometholone was discontinued. The active corneal lesions subsided after treatment for 4 days and the IOP decreased to 21 mm Hg. Without using any antiglaucoma agents, the IOP remained normal during the remaining 1 month of follow-up. Patient 14 had elevated IOP to 26 mm Hg in the diseased right eye and 14 mm Hg in the left eye at the first clinic visit. According to his old chart, IOP was normal in both eyes previously. The latest measurement was 14 mm Hg in the right eye and 13 mm Hg in the left 7 months previously. We did not prescribe him any antiglaucoma agent. The high IOP persisted for 1 week and then declined to 14 mm Hg after resolution of the keratitis. Fluorometholone was not prescribed until the IOP returned to normal.
Fine keratic precipitates were observed in 5 eyes in the late stages of the disease. Nummular anterior stromal infiltrates were noted in 2 eyes. Both findings disappeared gradually with treatment with 0.02% fluorometholone.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


