Purpose
To evaluate the use of topography-guided conductive keratoplasty in eyes with keratoconus.
Design
Interventional case series.
Methods
We examined 21 eyes in 21 patients with advanced keratoconus. Topography-guided conductive keratoplasty was performed with intraoperative monitoring of corneal astigmatism using a surgical keratometer. Uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BSCVA), corneal topography, manifest refraction, intraocular pressure (IOP), corneal endothelial cell counts, complications, and eventual outcomes were evaluated.
Results
UCVA (logarithm of the minimal angle of resolution [logMAR]), which was 1.65 ± 0.49 preoperatively, improved to 1.04 ± 0.64 at 1 week ( P < .001) and 1.12 ± 0.61 at 1 month after surgery ( P < .001). BSCVA, which was 1.02 ± 0.56 preoperatively, improved to 0.76 ± 0.65 at 1 week ( P = .026) and 0.76 ± 0.60 at 1 month after surgery ( P = .003). Manifest refraction, which was −15.13 ± 6.66 diopters (D) before surgery, declined to −9.97 ± 6.71 D at 1 month after surgery ( P = .002). Although corneal topography reverted to the preoperative pattern and UCVA and BSCVA also regressed toward preoperative values, 12 of 21 eyes were better able to tolerate and conduct normal daily activities using contact lenses. Five subjects have undergone or are considering corneal transplantation after unsatisfactory postoperative results. No serious perioperative complication was observed.
Conclusions
Topography-guided conductive keratoplasty may be effective in reshaping corneal configuration in eyes with keratoconus, without serious complications, and possibly contributed to avoiding or delaying corneal transplantation.
Keratoconus is a progressive disorder characterized by central or paracentral thinning and protrusion of the cornea. Keratoconus is usually diagnosed in the second or third decade of life, and as long as the disease is mild to moderate, the refractive error is typically corrected by wearing spectacles or contact lenses. However, as the disease progresses, correction with contact lenses becomes impossible in some patients.
Surgical approaches for advanced keratoconus have long been limited to corneal transplantation. Excimer laser–assisted corneal refractive surgery is relatively contraindicated for keratoconus eyes, because it can induce keratectasia postoperatively, resulting in more severe protrusion of the cornea, exacerbation of irregular astigmatism, and decreased visual acuity, especially after laser in situ keratomileusis.
Recently, additional surgical options for keratoconus have been proposed. Corneal cross-linking, which is the instillation of riboflavin solution followed by ultraviolet A (UVA) irradiation, halts the progression of keratoconus. Implantation of phakic intraocular lenses (IOL) is also effective in the correction of refractive errors in eyes with keratoconus; however, it is only appropriate for mild-to-moderate cases with good best spectacle-corrected visual acuity (BSCVA). The insertion of intracorneal ring segments can improve the uncorrected visual acuity (UCVA) of eyes with mild keratoconus and improve the BSCVA of eyes with moderate-to-advanced keratoconus.
Conductive keratoplasty (CK) is a novel method to reshape corneal configuration using radiofrequency energy. The efficacy of CK is attributed to the electrically conductive properties of the corneal stroma. The high-frequency energy is delivered to the cornea through a thin probe that penetrates 90% of the corneal stroma. The resistance to current flow through the tissue generates heat, resulting in a homogeneous thermal footprint, with controlled shrinkage of the surrounding collagen lamellae. For the correction of hyperopia or presbyopia, thermal spots placed on the mid-peripheral cornea cause a “belt-tightening” effect, which increases the curvature of the central cornea, inducing myopic shift.
The use of CK for modeling of the keratoconic cornea has previously been reported by 2 clinicians. Alió and associates reported 3 cases of keratoconus or post-LASIK keratectasia that showed an improvement in visual acuity (1 or 2 lines) in response to CK, alone or in combination with intracorneal ring segments. Lyra and associates reported treatment results for 25 eyes with keratoconus, in which 8 or 16 thermal spots were placed at 4.0 and 5.0 mm in the optical zone. The authors reported that BSCVA improved about 4 lines and manifest refraction improved 1 to 3 diopters (D). Both investigators placed thermal footprints at regular intervals on the concentric ring in most cases.
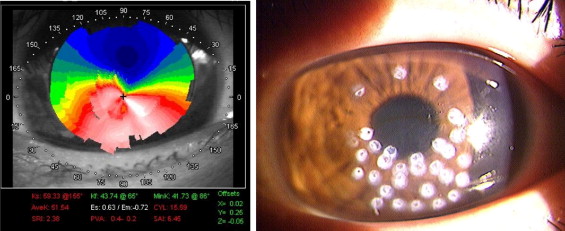
We performed CK on the keratoconic cornea using a modified procedure. The tip of the delivery probe was placed more proximal to the pupillary center, approximately 3 to 5 mm in diameter. The pattern of application was modified according to the preoperative and intraoperative corneal shape. In most cases, the thermal footprints generated were concentrated in the inferior area of the cornea, where most of the protrusion occurs in the keratoconic cornea, resulting in flattening of the curvature and alignment of the cornea, according to individual corneal shape ( Figure 1 ). We named this modified CK procedure topography-guided conductive keratoplasty. Topography-guided conductive keratoplasty was successful in reshaping the irregularity of advanced keratoconus quite effectively, reducing irregular astigmatism and improving visual acuity.
In this manuscript, we report our experience using topography-guided conductive keratoplasty for advanced keratoconus, and we also discuss its indications and unsolved issues and possible solutions regarding this method.
Methods
Patients
Twenty-one eyes in 21 patients (20 male, 1 female; mean age, 34.7 ± 11.7 years; subjective refraction: −15.13 ± 6.66 D) with advanced keratoconus were enrolled. All patients were referred to or visited our institutes for corneal transplants because of extreme protrusion of the cornea and subsequently poor corrected visual acuity and/or contact lens intolerance. Two eyes had previously undergone cataract extractions and IOL implantations, and 1 eye had previously undergone the implantation of intracorneal ring segments.
Keratoconic Conductive Keratoplasty Procedure
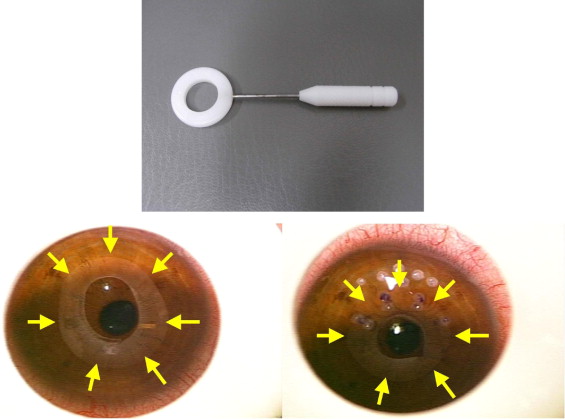
The ViewPoint CK System (Refractec, Inc, Irvine, California, USA) consists of a radiofrequency energy–generating console; a hand-held, reusable, pen-shaped hand piece attached to a removable cable and connector; a foot pedal that controls the release of radiofrequency energy; and a speculum that provides a large surface for the electrical return path. A single-use, disposable, stainless-steel keratoplast tip is attached to the probe (Refractec, Inc); this tip delivers the current directly to the corneal stroma. The radiofrequency generator (RCS-200, Refractec, Inc) emits macropulses up to 1 second in duration. Each macropulse consists of micropulses, which are essentially 350-kHz sinusoidal waveforms. The amplitude of a set of micropulses is varied by changing the power setting on the CK unit. Typical clinical settings are 60% power (eg, 200 volt peak-to-peak) and 600-ms macropulse duration.
All surgeries were performed by the same surgeon (K. Tsubota), who was certified by Refractec, Inc. After the instillation of 4% xylocaine eye drops as topical anesthesia, the topography-guided conductive keratoplasty procedure was performed. The delivery probes were placed to make thermal spots, while simultaneously monitoring intraoperative changes using a keratoring (Handaya Co Ltd, Tokyo, Japan). The surgeon preplanned the spot placement pattern according to the topography map before surgery. Then, after making several initial spots, the surgeon examined the corneal configuration using the keratoring ( Figure 2 ). When the configuration of keratoring was not round, the additional spots were placed to the appropriate area. The entire corneal thickness was assessed preoperatively, and the delivery probes were inserted perpendicularly as per the manufacturer’s protocol. In areas where corneal thickness was less than 450 μm, the delivery probes were inserted obliquely, at angles of 45 to 60 degrees into the stroma, centrifugally from thinner point to thicker point, as needed, to avoid damaging the endothelium or penetrating the anterior chamber. These procedures were repeated until the configuration of the pupillary area became symmetrical ( Figure 2 ).
Immediately after the procedure, all eyes received topical diclofenac sodium (Stafulmin, Kowa Company, Limited, Aichi, Japan), levofloxacine (Cravit, Santen, Osaka, Japan), and 0.3% hyaluronic acid (Hyalein, Santen) 5 times per day for 1 week after surgery.
Postoperative Examinations
Postoperative examinations were performed 1 day, 1 week, 1 month, 3 months, 6 months, and 1 year after surgery. The UCVA, BSCVA, manifest refraction, corneal topography, intraocular pressure (IOP), and corneal endothelial count were measured, in addition to routine ophthalmologic and funduscopic examinations. Corneal topography was evaluated by TMS-4 (Tomey, Aichi, Japan). Corneal endothelial cells were counted with a specular microscope (Noncon Robo SP-9000, Konan, Hyogo, Japan).
Eighteen eyes were followed up for 3 months, 11 for 6 months, and 8 reached the 1-year postoperative examination. Four cases transferred to other clinics were interviewed by phone regarding any difficulties in visual performance, plans for additional surgical treatment, and their ability to wear contact lenses 1 year after the surgery.
Statistical Analyses
For statistical analysis, the Wilcoxon test was used. P values < .05 were deemed to indicate statistical significance.
Results
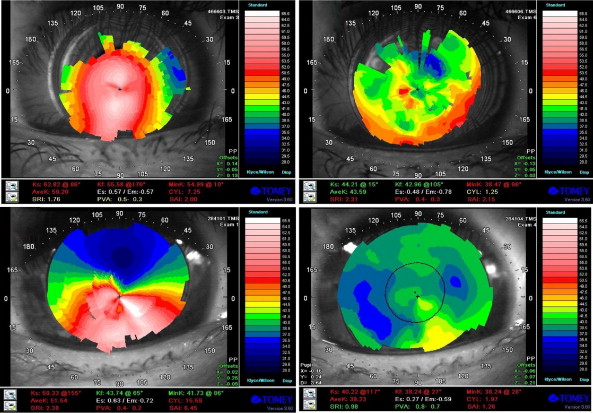
The individual patients’ data and outcomes of the topography-guided conductive keratoplasty are shown in the Table . Of the 21 eyes, corneal transplantation was avoided or delayed in 15 eyes (71.4%). We indicate the changes in corneal topography of typical cases in Figure 3 .
| Case | Age | Gender | Previous Surgery | Preop UCVA | Preop BSCVA | Preop MR | Preop Kave | Postop Best Achieved UCVA (Time After TGCK) | Postop Best Achieved BSCVA (Time After TGCK) | Postop Kave (Same Time Point as BSCVA) | Outcome at the Final Examination Point (Time of Final Evaluation) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 27 | M | — | 1.7 | 0.8 | −18.0 | 61.75 | 0.4 (1 wk) | 0.0 (6 mo) | 60.93 | CT (2 y) |
| 2 | 23 | M | — | 1.4 | 0.4 | −12.0 | 61.125 | 1.2 (1 d) | 0.2 (3 mo) | 52.5 | CL (1 y) |
| 3 | 17 | M | — | 0.4 | −0.1 | −12.0 | 49.875 | 0.5 (1 wk) | −0.1 (6 mo) | 46.125 | CL (1 y) |
| 4 | 28 | M | — | 1.7 | 1.0 | −9.0 | 50.625 | 0.2 (1 wk) | 0.0 (1 wk) | 43.125 | CL (1 y) |
| 5 | 32 | M | ICRS | 1.2 | 1.0 | −12.0 | 57.00 | 0.5 (1 wk) | 0.5 (1 wk) | 37.875 | (1 mo) |
| 6 | 42 | M | IOL | 1.3 | 1.0 | −23.0 | 68.875 | 1.1 (1 wk) | 0.8 (1 wk) | 54.755 | Repeated TGCK, CT (6 mo) |
| 7 | 20 | M | — | 1.7 | 0.7 | −10.0 | 44.02 | 1.0 (1 wk) | 0.7 (1 wk) | 32.155 | CT (6 mo) |
| 8 | 27 | M | — | 1.7 | 0.4 | −10.875 | 56.75 | 0.7 (1 d) | 0.0 (1 mo) | 49.215 | (6 mo) |
| 9 | 26 | M | — | 2.0 | 2.0 | 0 | 58.25 | 0.7 (1 d) | 0.4 (1 mo) | 57.5 | CL (3 mo) |
| 10 | 44 | M | — | 1.7 | 0.7 | −21.75 | 43.79 | 1.0 (1 wk) | 0.7 (1 mo) | 33.6 | Repeated TGCK, CL (1y) |
| 11 | 53 | M | — | 1.4 | 0.5 | −17.0 | 47.765 | 0.1 (1 wk) | 0.1 (1 wk) | 50.0 | (3 mo) |
| 12 | 19 | F | — | 1.4 | 0.4 | −6.5 | 62.425 | 0.1 (1 wk) | 0.1 (1 wk) | 49.25 | Repeated TGCK, CL (1y) |
| 13 | 45 | M | — | 2.0 | 1.4 | −14.0 | 62.935 | 1.4 (1 mo) | 0.3 (6 mo) | 52.33 | CL (1 y) |
| 14 | 45 | M | — | 2.0 | 1.7 | −28.5 | 52.105 | 2.0 (1 d) | 1.0 (1 y) | n.m. | CL (1 y) |
| 15 | 29 | M | — | 1.7 | 1.4 | −6.25 | 69.085 | 1.2 (1 d) | 1.5 (1 mo) | 53.485 | Repeated TGCK (6 mo) |
| 16 | 35 | M | — | 1.0 | 0.5 | −7.5 | 47.625 | 0.2 (1 mo) | 0.0 (1 wk) | 39.25 | CXL at 2 mo (1 y) |
| 17 | 48 | M | — | 2.0 | 1.5 | −18.0 | 47.95 | 2.0 (1 d) | 0.8 (3 mo) | 48.28 | Repeated TGCK, CT (6 mo) |
| 18 | 37 | M | IOL | 1.5 | 1.2 | −17.0 | 56.88 | 0.3 (6 mo) | 1.0 (1 wk) | 46.5 | CL (3 mo) |
| 19 | 28 | M | — | 1.7 | 1.7 | 0 | 39.05 | 0.8 (1 d) | 0.8 (1 wk) | 55.455 | CL, (CT) (3 mo) |
| 20 | 61 | M | — | 2.0 | 1.4 | −28.0 | 61.125 | 1.5 (1 d) | 1.3 (3 mo) | 64.24 | CT (1 y) |
| 21 | 27 | M | — | n.m. | 1.7 | −16.0 | n.m. | 1.7 (1 d) | 1.5 (1 wk) | 53.75 | CL (6 mo) |
Uncorrected Visual Acuity
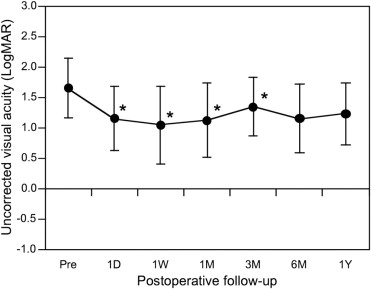
The mean ± standard deviation of UCVA (logarithm of the minimal angle of resolution [logMAR]) was 1.65 ± 0.49 preoperatively, 1.15 ± 0.52 at 1 day ( P = .001 compared to the preoperative value), 1.04 ± 0.64 at 1 week ( P < .001), 1.12 ± 0.61 at 1 month ( P < .001), 1.34 ± 0.48 at 3 months ( P = .008), 1.15 ± 0.57 at 6 months ( P = .050), and finally 1.23 ± 0.51 at 1 year after surgery ( P = .273; Figure 4 ).
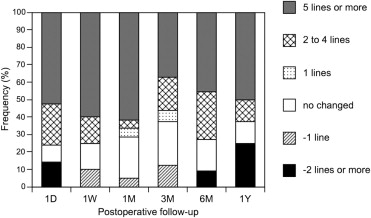
When we compared the postoperative to preoperative UCVA values in individual subjects, postoperative UCVA improved more than 5 lines in 11 of 20 eyes (60%), 3 lines in 1 eye (5.0%), and 2 lines in 2 eyes (10.0%) at 1 week after surgery. However, postoperative UCVA was unchanged in 3 eyes (15.0%) and decreased 1 line in 2 eyes (10.0%) at 1 week after surgery. At the 1-month examination, the frequency of eyes with improved UCVA was not grossly changed, although it decreased slightly thereafter. Eyes with improved UCVA accounted for 60% to 70% of cases throughout the follow-up period ( Figure 5 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


