surrounding extraocular muscles.11 The hydrophilic GAGs cause edematous expansion of eye muscles and other orbital tissues. Some orbital fibroblasts and muscle cells will differentiate into adipocytes (adipogenesis), further increasing the orbital volume.12 A heterogeneous population of orbital fibroblasts among patients may provide the basis for variability in clinical activity. In addition to their function as antigen-presenting cells, B-cells are also precursors to antibody-producing plasma cells.
TABLE 17.1 Clinical features of hyperthyroidism | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
sparing of muscle insertions is typical.20 The inferior and medial recti tend to be enlarged more than the superior and lateral recti. The enlarged recti muscle bellies are best visualized on a coronal orbital image (see Fig. 17.4). Abnormally enlarged extraocular muscles are seen in up to 90% of patients radiographically, but diplopia occurs in only one-third.21 Imaging is helpful to distinguish fat-predominant versus muscle-predominant orbital expansion. Significant crowding at the orbital apex can result in congestive and compressive optic neuropathy. This is particularly dangerous in the absence of exophthalmos. Signs of compressive optic neuropathy include decreased visual function, optic disc edema or pallor, color desaturation, or an afferent pupillary defect. TAO is more severe in older patients and in males.22 Compressive optic neuropathy does not occur in children.4 Rarely, patients suffer concomitant autoimmune myasthenia gravis, which presents as variable blepharoptosis, diplopia, or saccadic fatigue.
TABLE 17.2 Manifestations of thyroid-associated orbitopathy | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 FIGURE 17.1 Mild-to-moderate asymmetrical disease. Bilateral upper eyelid swelling, conjunctival injection, and chemosis. Right upper and lower eyelid retraction. |
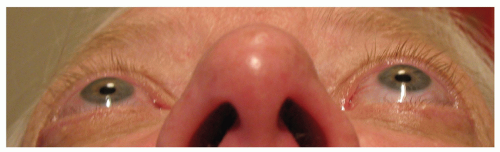 FIGURE 17.2 Moderate-to-severe asymmetrical disease. Submental view of left exophthalmos. |
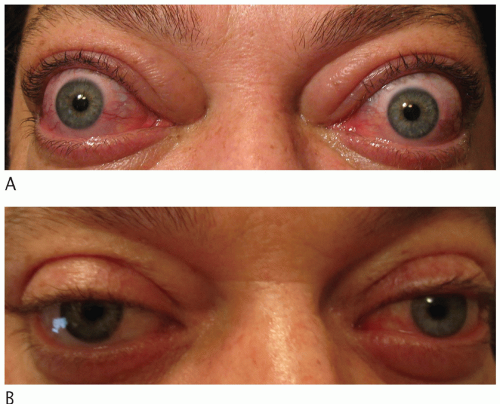 FIGURE 17.3 (A) Vision-threatening symmetrical disease. Upper and lower eyelid swelling and retraction, conjunctival injection and chemosis, restrictive strabismus and exophthalmos, and compressive optic neuropathy. (B) Six months after high-dose steroids, surgical decompression, strabismus repair, and eyelid retraction repair. |
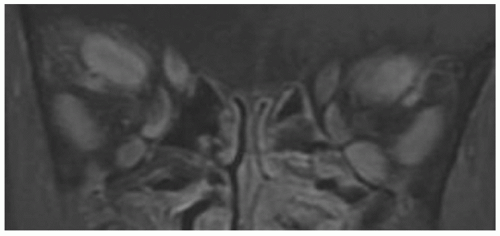 FIGURE 17.4 Coronal T1-weighted, fat-suppressed, gadolinium-enhanced magnetic resonance image of enlarged extraocular muscle bellies from vision-threatening thyroid-associated orbitopathy. |
comanaged with internists or endocrinologists whose goals are to stabilize thyroid function with antithyroid drugs (ATDs) and to help in the decision-making process regarding if and when thyroid ablation is required. Oral thioamides (methimazole, carbimazole, or propylthiouracil) are commonly used, and randomized, controlled studies support initial therapy with methimazole for efficacy and tolerability.31 The ATD administration regimens are either titration or a block-and-replace strategy. Thyroid ablation, whether by surgical thyroidectomy or radioiodine (I-131), is typically used when thyroid levels are unstable on ATDs. Thyroidectomy (total, near total, or subtotal) may be preferable for patients that exhibit a goiter or thyroid gland enlargement, but risks include hypoparathyroidism and permanent damage to the recurrent laryngeal nerve. The main disadvantage of radioiodine ablation is the increased risk and severity of TAO in susceptible patients.32 This phenomenon is worse in smokers and likely related to the high concentration of thyroid antigens released during necrosis of thyroid follicular cells. An oral administration of 5 to 15 mCi results in an absorbed radiation dose of 50 to 100 Gy. A study of 450 patients shows that the rate for TAO progression during radioiodine ablation is 15% but can be mitigated with a short course (1 to 3 months) of oral steroids.33 Posttreatment hypothyroidism should also be avoided.34 Patients who are nonsmokers and lack evidence of TAO can probably undergo radioiodine ablation without steroid prophylaxis. A recent randomized, placebo-controlled study found that Ginkgo biloba extract decreases radiation-induced genotoxic damage during radioiodine therapy.35
TABLE 17.3 Clinical activity score (CAS) to quantify disease activity | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
analysis of TSI is preferable to using specific values as thresholds for intervention. When the TSI levels begin to decrease and plateau, this indicates disease stabilization. The values typically never return to normal levels. Neuroimaging with computed tomography or magnetic resonance imaging can help confirm the diagnosis of TAO, especially for euthyroid patients (see Fig. 17.4).
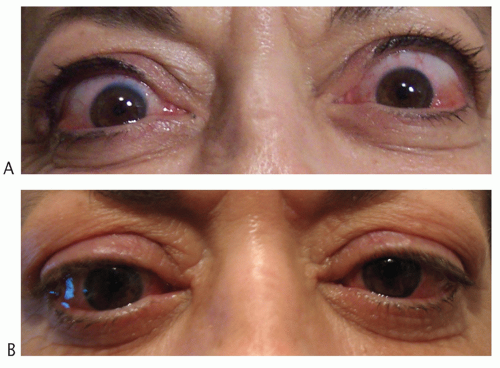 FIGURE 17.5 (A) Bilateral upper eyelid retraction left greater than right. (B) Two months after bilateral upper eyelid recession (posterior transconjunctival mullerectomy). |
(EUGOGO) using major and minor criteria.33 (See Table 17.4 for an overview of management options based on disease severity.)
TABLE 17.4 Management of thyroid-associated orbitopathy based on disease severity | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
reduce GI symptoms. Overall, HDSs decrease the quality of life for most patients.58 Contraindications to HDSs include uncontrolled diabetes, severe hypertension, recent hepatitis, and pregnancy. As the disease stabilizes and the dose is tapered, rebound inflammation can occur.30
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


